
Abstract
In the pathogenesis of atherosclerosis, oxidative stress plays a major role in plaque instability, rupture, and erosion, which subsequently leads to thrombus formation and causes total infarct-related artery (IRA) occlusion. We investigated the relationship between spontaneous reperfusion (SR) of IRA and oxidative stress in patients with anterior ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention. A total of 341 consecutive patients with anterior STEMI were prospectively included in the present study. Patients were divided into 2 groups according to their thrombolysis in myocardial infarction (TIMI) flow grade: SR group (66 patients, TIMI flow 3) and non-SR group (275 patients, TIMI flow 0-2). On multivariate logistic regression analysis, oxidative stress index (β = 0.868, 95% confidence interval [CI] = 0.806-0.934, P < .001), neutrophil to lymphocyte ratio, uric acid, mean platelet volume, Killip 2 to 4 class, and initial SYNTAX score were independently associated with SR. Oxidative stress as well as inflammation may play a pivotal role in the pathogenesis of SR in patients with STEMI.
Keywords
Introduction
In patients with acute ST-segment elevation myocardial infarction (STEMI), urgent restoration of blood flow in infarct-related coronary artery (IRA) is related to improved survival. 1 In several reports, it has been demonstrated that patients who underwent primary percutaneous coronary intervention (pPCI) had a better outcome if they had thrombolysis in myocardial infarction (TIMI) 3 patency before pPCI. 2,3 Moreover, pre-pPCI spontaneous reperfusion (SR) of IRA in patients with STEMI is a major determinant of after pPCI TIMI 3 flow, which is related to an improved prognosis. 3 –5
Oxidative stress, defined as the impaired balance between oxidant and antioxidant systems, plays a crucial role in the pathogenesis of both atherosclerosis and acute coronary syndromes including STEMI. 6 –8 Although total antioxidant status (TAS) reflects the total effect of all antioxidants in the plasma and body, 9 total oxidant status (TOS) shows the total effect of all oxidants. 10
Oxidative stress is one of the major contributors to atherosclerotic plaque instability with inflammation process. 11 The principal mechanisms of total coronary occlusion and acute STEMI are plaque rupture, erosion, and subsequent thrombus formation. 11 It was shown that plasma oxidants and oxidized low-density lipoprotein (LDL) levels increased in patients with erythrocyte-rich thrombi following STEMI. 12 Furthermore, oxidative stress is also associated with no-reflow following pPCI, which is a predictive of cardiovascular events in patients with STEMI. 8,13 Based on these findings, we investigated the relationship between SR of IRA and oxidative stress markers, such as TAS, TOS, and oxidative stress index (OSI) in patients with anterior STEMI undergoing pPCI.
Materials and Methods
Study Population
We prospectively included 341 consecutive patients with anterior STEMI who underwent pPCI (mean age: 54.5 ± 11.6 years) between July 2013 and May 2014. This study is a continuation of our previous study that investigated the relation between oxidative stress and contrast-induced nephropathy in patients with STEMI. 14 Additionally, we included 52 more patients to the study population during the lead time. Patients were divided into 2 groups: SR group (n = 66) and non-SR group (n = 275). The STEMI was defined as resting chest pain lasting ≥30 minutes, together with new or presumed new ST-segment elevation in ≥2 contiguous leads with a cutoff point ≥0.2 mV in anterior leads. The diagnosis was confirmed by coronary angiography in all patients. All patients received standard contemporary coronary artery disease (CAD) treatment of aspirin, clopidogrel, β-blockers, angiotensin-converting enzyme inhibitors, and statins.
Patients with a recent history of CAD, late presentation (>12 hours), infectious or inflammatory disease, severe liver or renal disease, neoplasm, or hematological disorders, and treatment with aspirin/clopidogrel/warfarin/unfractionated heparin, low-molecular-weight heparin, and thrombolytic therapy were excluded from the study. Patients taking antioxidant drugs such as diuretics, angiotensin-converting enzyme inhibitors (captopril and zofenopril), β-blockers (carvedilol and nebivolol), and vitamins (such as E and C) were excluded from the study. No dietary variation was present between the groups. Patients taking xenobiotics and alcohol were also excluded from the study. Exclusion criteria were applied to all the groups. The Local Ethics Committee approved the study protocol, and each participant provided written informed consent.
After assessment of detailed medical history and a complete physical examination, the baseline characteristics including age, sex, hypertension, hyperlipidemia, diabetes mellitus, smoking status, family history of CAD, body mass index, and medications were recorded for all patients. Also, Killip classification and the time interval from the onset of symptoms to hospital admission were recorded in all patients. 15 Left ventricle ejection fraction was measured using Simpson method according to the suggestions of the American Society of Echocardiography. 16
Blood Samples
In all patients, antecubital venous blood samples were taken on admission in the emergency department, before the patients were started any medications and transferred to the catheter laboratory. Samples were taken from cubital vein into blood tubes and immediately stored on ice at 4°C. The serum was then separated from the cells by centrifugation at 3000 rpm for 10 minutes. Serum samples were stored at −80°C until analysis of lipid parameters, TOS, and TAS.
Blood counts were measured by a Sysmex K-1000 (Block Scientific, Bohemia, New York) autoanalyzer within 5 minutes of sampling. Plasma triglyceride, LDL, high-density lipoprotein, glucose, uric acid, and creatinine concentrations were measured with an automated chemistry analyzer (Abbott Aeroset, Minnesota) using commercial kits (Abbott). Activity of creatine kinase MB (CK-MB) was measured with an assay that uses 2 monoclonal antibodies (CKMB STAT) on an Elecsys 2010 analyzer (Roche Diagnostics, Basel, Switzerland) by electrochemiluminescence immunoassay. Plasma N-terminal probrain natriuretic peptide was measured by electrochemiluminescence. (Roche Diagnostics, Mannheim, Germany). High-sensitive cardiac troponin T was measured using a fourth-generation assay on an Elecsys 2010/cobas e 411 instrument (Roche Diagnostics).
Measurement of TOS, TAS, and OSI
Total antioxidant status was measured using an automated new-generation, more stable, colored 2,2-azinobis-(3-ethylbenzothiazoline-6-sulfonic acid) radical cation (ABTS+). The ABTS+ is decolorized by antioxidants according to their concentrations and antioxidant capacities. This change in color was measured as a change in absorbance at 660 nm. This process was applied to an automated analyzer, and the assay was calibrated with Trolox. The results were expressed as mmol Trolox equivalent/L. 9
Total antioxidant status was determined using an automated measurement method. The oxidants in the sample oxidize the ferrous ion-o-dianisidine complex to ferric ion. The ferric ion makes a colored complex with xylenol orange in an acidic medium. The color intensity, measured spectrophotometrically, is related to the total amount of oxidant molecules present. The assay was calibrated with hydrogen peroxide (H2O2), and the results were expressed as μmol H2O2 equivalent/L. 10
Oxidative Stress Index Was Calculated by the TOS/TAS Formula
Coronary angiography and thrombolysis in myocardial infarction flow grade
All patients underwent selective coronary angiography using the Judkins technique. Primary PCI procedures were performed with standard femoral approach using a 7F guiding catheter. To achieve maximal dilation, each coronary angiogram was preceded by intracoronary injection of 100 μg nitroglycerine. TIMI flow grade was documented for each patient. 17 TIMI flow grade 0 was defined as complete occlusion with no angiographic visualization of the vessel beyond the site of stenosis, whereas TIMI flow grade 3 was defined as complete filling of the distal vessel by the third cardiac cycle. 17 Angiograms were analyzed according to the presence or absence of SR as defined by TIMI flow grade 3 (vs TIMI grade 0, 1, or 2). 17 Two experienced interventional cardiologists analyzed the TIMI flow grade and IRA assessment; the opinion of a third analyst was obtained, and the final judgment was made by consensus in cases of disagreement. Patients with pre-PCI were divided into 2 groups based on the TIMI flow grade: non-SR was defined as TIMI grade 0, 1, and 2 flows (impaired flow group) and SR was defined as TIMI 3 flow (normal flow group). The coefficient of interobserver variation was 2.4% for IRA evaluation.
Statistical Analysis
Statistical analysis was carried out using SPSS 17.0 for Windows (SPSS Inc, Chicago, Illinois). Data are expressed as mean ± standard deviation. Continuous variables were tested for normality using the Kolmogorov-Smirnov test. An independent simple t test was used in the analysis of continuous variables. Categorical variables were compared using the chi-square test. Multivariate, stepwise backward conditional logistic regression analysis was used to determine the independent predictors of SR. All significant parameters in the univariate analysis were selected in the multivariate model. A receiver–operator characteristic (ROC) curve analysis was carried out to identify the optimal cutoff point of OSI in patients with STEMI and SR. The area under the curve (AUC) was calculated as a measure of the accuracy of the test. A 2-tailed P value <.05 was considered significant.
Results
Infarct-related artery patent and non-IRA patent groups included 66 (19.3%) and 275 (80.7%) patients, respectively. Comparison of baseline, clinical, laboratory, and echocardiographic parameters between the groups is shown in Table 1. Frequencies of the patients with preinfarct angina and Killip 2 to 4 class were higher in the non-SR group than in the SR group (P < .05, for all). Moreover, ejection fraction values of the SR group were higher and initial SYNTAX scores were lower than the non-SR group (P < .05, for both). In-hospital mortality rate of patients with SR was lower compared to patients without SR (1.5% vs 2.5%), but this finding did not reach statistical significance (P > .05).
Comparison of Baseline, Clinical, and Laboratory Characteristics of Groups.
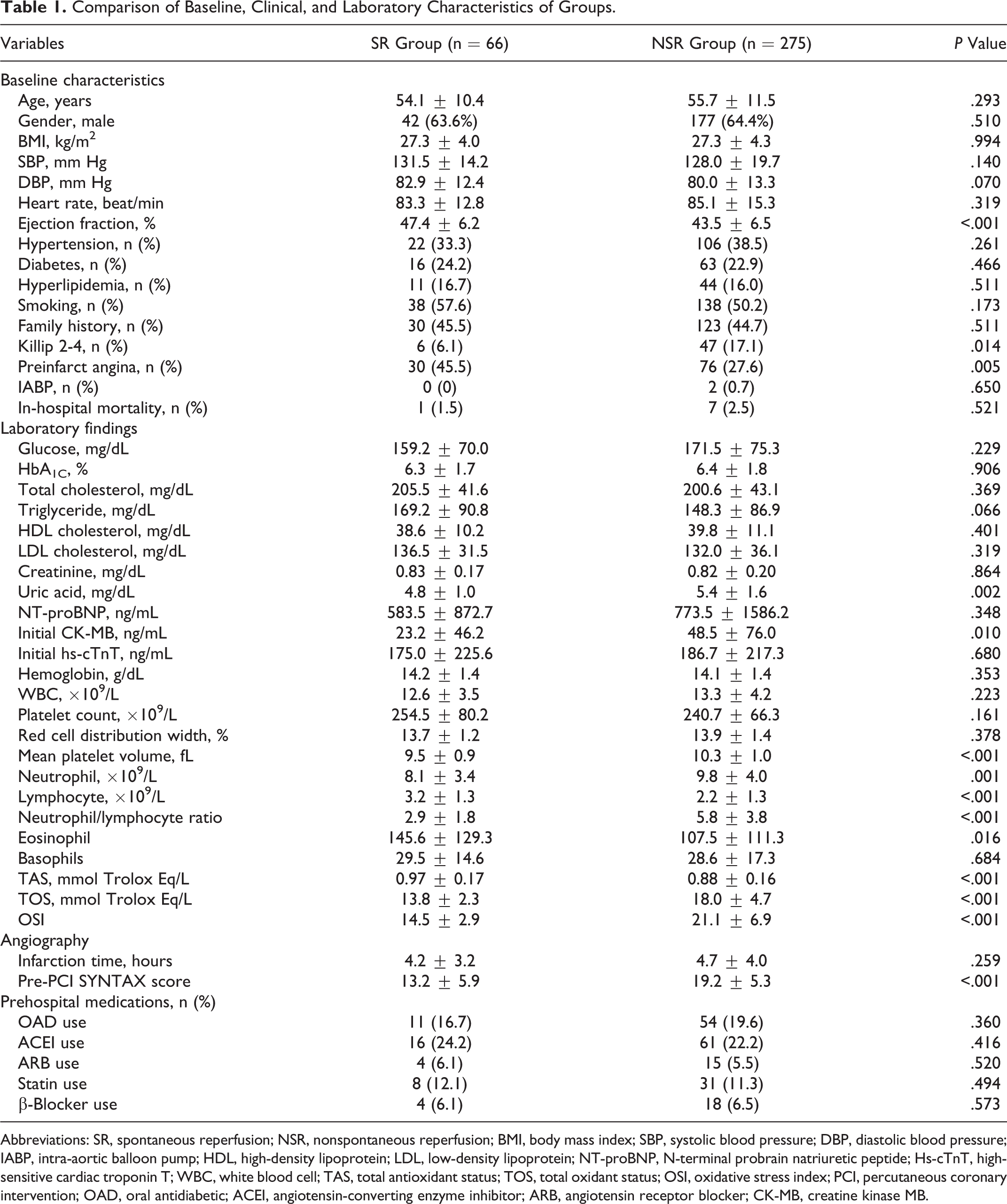
Abbreviations: SR, spontaneous reperfusion; NSR, nonspontaneous reperfusion; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; IABP, intra-aortic balloon pump; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NT-proBNP, N-terminal probrain natriuretic peptide; Hs-cTnT, high-sensitive cardiac troponin T; WBC, white blood cell; TAS, total antioxidant status; TOS, total oxidant status; OSI, oxidative stress index; PCI, percutaneous coronary intervention; OAD, oral antidiabetic; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CK-MB, creatine kinase MB.
Compared to the SR group, eosinophil and TAS levels were significantly lower, whereas TOS and OSI levels, uric acid level, creatinine level, initial CK-MB, neutrophil–lymphocyte ratio, and mean platelet volume (MPV) were significantly higher in the non-SR group (P < .05, for all; Table 1).
Independent Predictors of SR in Anterior STEMI
Oxidative stress index (95% confidence interval [CI]: 0.613-0.800, P < .001), Killip class 2 to 4 (95% CI: 1.114-26.057, P = .036), initial SYNTAX score (95% CI: 0.844-0.972, P < .001), uric acid (95% CI: 0.439-0.813, P = .001), MPV (95% CI: 0.371-0.909, P = .017), and neutrophil–lymphocyte ratio (95% CI: 0.582-0.834, P < .001) were found to be independent predictors for SR on multiple logistic regression analysis (Table 2).
The Independent Predictors of pre-PCI Spontaneous Reperfusion.
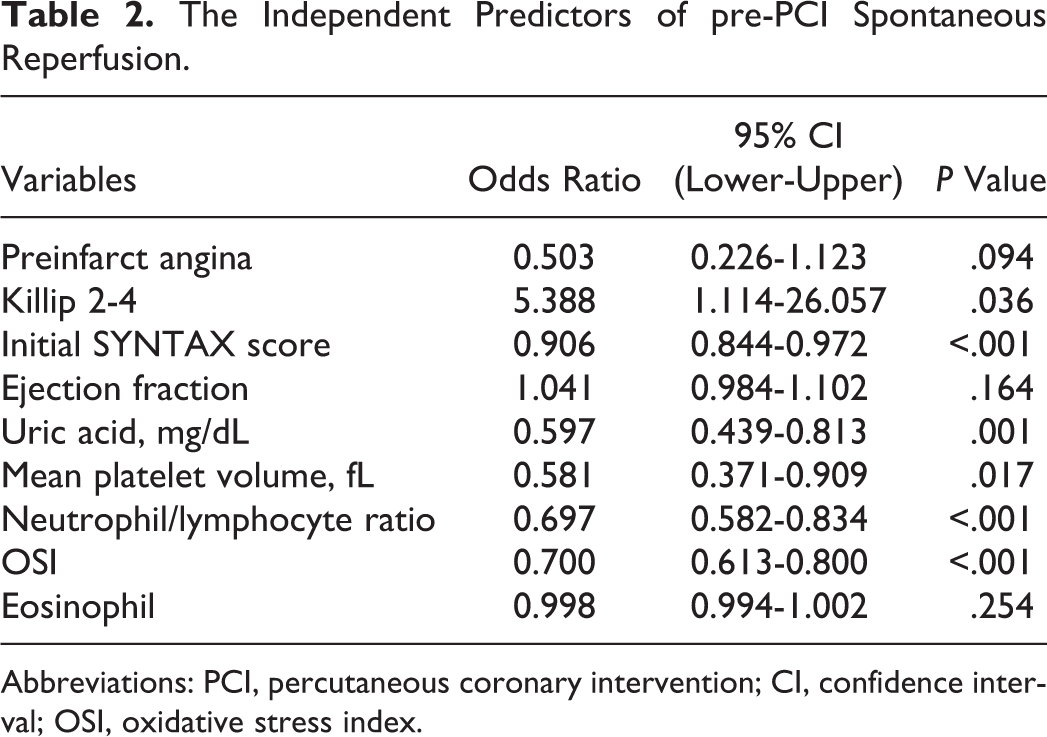
Abbreviations: PCI, percutaneous coronary intervention; CI, confidence interval; OSI, oxidative stress index.
Receiver–operator characteristic Curve Analysis
The cutoff value of OSI obtained by the ROC curve analysis was 15.6 for the prediction of non-SR (sensitivity: 79% and specificity: 78%). The AUC was 0.831 (95% CI: 0.782-0.879, P < .001). The ROC curve for predicting the poor TIMI flow (non-SR) in IRA is shown in Figure 1.
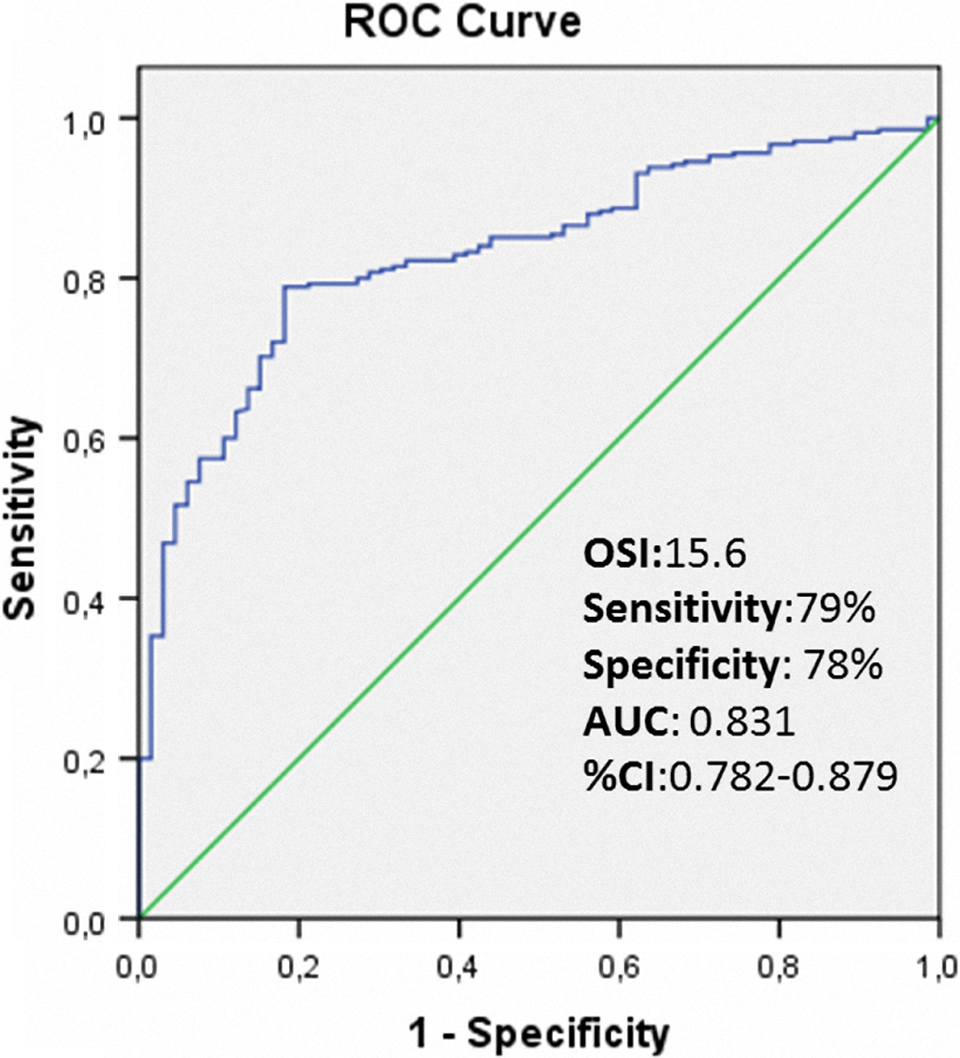
The receiver–operator characteristic (ROC) curve analysis of OSI for predicting the poor thrombolysis in myocardial infarction (TIMI) flow.
Discussion
To the best of our knowledge, this is the first study that investigated the relationship between pre-pPCI IRA patency and oxidative stress in patients with STEMI. Our study shows that increased oxidative stress is a good predictor of poor TIMI flow in IRA.
Coronary blood flow of IRA is an important determinant of prognosis in patients with STEMI. In previous studies, the rate of TIMI grade 3 flow before pPCI occurring spontaneously has been found to be around 15% to 20%. 2,18 In the present study, TIMI grade 3 flow before pPCI was reported in 19.3% of the patients. In several previous studies, it has been demonstrated that patients showing pre-PCI IRA patency had an increased rate of TIMI grade 3 flow after the primary PCI, 3 –5 better improved ST-segment resolution, 3 decreased rates of heart failure and cardiogenic shock, improved both early and late LVEF, decreased morbidity, and reduced short- and long-term mortality. 2,3
Oxidative stress occurs if there is an increased production of oxidizing species or a significant decrease in the effectiveness of antioxidant defenses. In a previous study, it has been reported that oxidant–antioxidant balance was impaired and oxidative stress was increased in patients with acute STMI. 19 Cardiovascular diseases, including STEMI, are associated with increased oxidative stress. 6 Recently, Guerin et al reported that oxidants were increased in occluded vessels during AMI, demonstrating that antioxidants were consumed. 7 It was also demonstrated that oxidative stress was an independent predictor for no-reflow phenomenon following pPCI in patients with STEMI. 8
Although relationship between oxidative stress and coronary flow dynamics is well known in patients with coronary slow flow and STEMI following pPCI, 8,20 this relationship has not been not investigated in patients with STEMI with and without SR before pPCI. The present study showed that oxidative stress was increased in patients without SR in IRA compared with patients showing IRA patency. We also showed that increased oxidative stress was a negative predictor of SR in anterior STEMI. The role of oxidative stress in pre-pPCI SR pathogenesis is not yet fully understood. Oxidative stress may facilitate thrombus formation causing total occlusion in IRA. 11,21 –25 Activity of reactive oxygen species in the vessel wall is thought to play a crucial role in the formation of oxidized LDL, which is a major contributor to the pathogenesis of atherosclerosis. 21 The relationship between oxidative stress and endothelial function may mediate impaired coronary flow. As the duration of disease increases, oxidative stress causes augmentation in vulnerability of fibrous cap of plaques to rupture, which consecutively progresses stable CAD to unstable angina and myocardial infarction. 22 Moreover, it has been shown that myeloperoxidase-derived reactive oxygen increased the release of tissue factor leading to a thrombotic state. 23 Therefore, increased oxidative stress in the preinfarction period can be reduced in the probability of SR by activating thrombus formation in IRA and by impairing endothelial function. On the other hand, thrombus formation leading to total occlusion in IRA may increase oxidative stress in patients with STEMI. 12 In a previous study, it has been reported that oxidants were increased in patients with acute coronary syndrome, demonstrating that antioxidants are consumed. 24 Also, previous studies showed that plasma pro-oxidant myeloperoxidase and oxidized-LDL levels were increased in patients with erythrocyte-rich thrombi. 12 Moreover, ischemia results in impaired antioxidant defense system in patients with STEMI. 7,24 Therefore, oxidative stress may facilitate thrombus formation leading to total occlusion in IRA and also oxidative stress may be increased as a result of the total occlusion in IRA.
The present study also showed that pre-pPCI SR of IRA was associated with neutrophil to lymphocyte ratio, MPV, uric acid, and Killip class 2 to 4 besides oxidative stress. It has been demonstrated that neutrophil to lymphocyte ratio was a useful marker to predict early and late clinical outcomes in patients with STEMI undergoing pPCI. 25 Neutrophil to lymphocyte ratio is also an independent predictor of both no-reflow phenomena after pPCI and SR in IRA before pPCI. 26,27 On the other hand, MPV is a well-known risk factor for cardiovascular disease. 28 Moreover, recent studies demonstrated that uric acid and MPV levels are independent predictors for SR of IRA in patients with STEMI. 27,29 Our study agrees with previous studies that investigated the relationship between SR with neutrophil to lymphocyte ratio, uric acid, and MPV.
According to recent reports, there is a strict correlation between oxidative stress and the pathogenesis of diabetes as well as hypertension and cardiovascular diseases. 30 Moreover, oxidative stress causes a complex dysregulation of cell metabolism and cell-to-cell homeostasis, which leads to insulin resistance and β-cell dysfunction. 30 On the other hand, endothelial dysfunction is an important component of diabetic vascular complications, and several studies have reported that reactive oxidant species play a crucial role in the pathogenesis of diabetic vasculopathy. 31 As a consequence, these mechanisms have important contributions in the pathophysiology of type 2 diabetes and its vascular complications including myocardial infarction. 30,31 However, in the present study, when the patients were divided into subgroups according to their diabetic status, we did not observe any difference in plasma oxidative stress parameters. Nonetheless, larger scale studies investigating the role on reperfusion pathophysiology of oxidative stress in diabetic patients with myocardial infarction are needed.
Study Limitations
The use of previous antioxidant medications such as statins, β-receptor blockers, and angiotensin-converting enzyme inhibitors may affect oxidative stress. 32,33 However, in our study, the frequency of previous statin use was similar between the groups. The patients taking antioxidant drugs such as zofenopril, captopril, and nebivolol were excluded from the study. Also, smoking may have a role in oxidative stress. In the present study, the rate of previous smoking was not different between the groups.
Conclusions
In patients with anterior STEMI who underwent primary PCI, oxidative stress on admission is independently associated with SR of IRA as well as neutrophil to lymphocyte ratio, MPV, uric acid, and Killip class 2 to 4. Oxidative stress as well as inflammation may play an important role in the pathogenesis of SR in patients with STEMI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.