
Abstract
Despite current guidelines recommendations about anticoagulant prophylaxis, many studies have shown an high venous thromboembolism (VTE) incidence in patients undergoing total hip and knee arthroplasty. A number of anticoagulants are currently available, but they have some limitations that affect their applicability and consequently their effectiveness. Several new oral anticoagulants (NOACs) have been developed in an attempt to overcome these limitations. Apixaban is a NOAC that selectively inhibits the coagulation factor Xa; it is approved for the prevention of VTE after total hip replacement and total knee replacement surgery. This review examines the results of main trials designed to test efficacy and safety of apixaban in major elective orthopedic surgery.
Keywords
Introduction
Venous thromboembolism (VTE) is a frequent and potentially fatal complication after elective major orthopedic surgery: several studies have shown that 5% to 36% of patients undergoing total hip replacement (THR) and 40% to 85% of patients undergoing total knee replacement (TKR) will develop venographically confirmed deep venous thrombosis in the absence of an adequate prophylaxis, and approximately 0.1% to 0.7% of them will have fatal pulmonary embolism (PE). 1,2
Consequently, national and international guidelines strongly recommend routine anticoagulant thromboprophylaxis to prevent VTE following THR and TKR for a minimum of 10 to 14 days rather than no antithrombotic prophylaxis. Recommended drugs for these patients are low-molecular-weight heparins (LMWHs), fondaparinux, dabigatran, rivaroxaban, low-dose unfractionated heparin commonly used in patients with severe renal impairment, adjusted-dose vitamin K antagonists (VKAs), aspirin, and apixaban. 2
The currently available anticoagulants have a well-established efficacy but also have some limitations: parenteral administration (LMWHs and fondaparinux), risk of heparin-induced thrombocytopenia (LMWHs), drugs–food interaction, and need for frequent laboratory monitoring for dose adjustment (VKAs). New oral anticoagulants (NOACs) have been developed to overcome these limitations and thereby improve patient care, especially after early hospital discharge and the need to manage the therapy by the patient himself. 3 –12
Apixaban is an oral, direct, potent, and selective inhibitor of coagulation factor Xa (FXa) that reversibly binds directly to the active site of FXa and exerts anticoagulant and antithrombotic effects by diminishing the conversion of prothrombin to thrombin. 13 Apixaban has an high oral bioavailability (approximately 52%), reaching the peak concentrations in 3 to 4 hours after administration within an 8 to 15 hours for half-life. 14 In addition, it is predominantly eliminated through metabolic pathways and nonrenal mechanisms with minimal potential for drug–drug interactions and the formation of reactive metabolites. 15 These pharmacologic characteristics potentially make apixaban an improved treatment option over other oral FXa inhibitors, parenteral heparins, or VKAs.
The aim of the present review is to summarize the results of studies performed to exploring the efficacy and safety of apixaban for the prevention of thromboembolism after major orthopedic surgery: the Apixaban for the Prevention of Thrombosis-Related Events (ADVANCE) program. 10 –12
Clinical Trials
Phase II
The Apixaban PROphylaxis in Patients undergoing tOtal knee replacement Surgery (APROPOS) clinical trial 16 is a phase II trials conducted to select and validate the optimal apixaban dose to use in the ADVANCE program. Different doses of apixaban, administered once daily or twice daily, were compared to enoxaparin 30 mg twice daily and warfarin standard prophylaxis in 1238 patients with TKR. Apixaban 5, 10, or 20 mg once-daily or 2.5, 5.0, or 10.0 mg twice-daily doses were compared; apixaban and enoxaparin 30 mg prophylaxis was started 12 to 24 hours after surgery, warfarin in the evening of surgery. All symptomatic or asymptomatic VTE (diagnosed by venography of the lower limb) and all-causes mortality have been evaluated as primary efficacy outcome; major bleedings were considered as primary safety outcomes. A significantly lower incidence of deep vein thrombosis (DVT) occurred in the apixaban group than in those receiving enoxaparin or warfarin, with a little dose-related increasing incidence of bleeding events. The best benefit-risk profile was obtained with a 2.5-mg twice-daily apixaban dose compared to enoxaparin and warfarin; thus, this dose was selected for validation in the phase III clinical program (ADVANCE studies).
Phase III
In the ADVANCE 1, 10 3608 patients following TKR were enrolled; 3195 of them were randomized in a double-blind manner to apixaban 2.5 mg twice daily or enoxaparin 30 mg twice daily, started 12 to 24 hours after surgery and administered for 10 to 14 days. In all, 3184 patients were included in safety analysis and the 72.4% (1157) of the first group and the 70.8% (1130) of the second one were included in primary efficacy analysis. The aim of this trial was to demonstrate the noninferiority of apixaban compared to enoxaparin, but the results of this study failed to achieve the goal.
The primary efficacy outcome occurred in 9.0% (104 of 1157) patients in the apixaban group and 8.8% (100 of 1130) in the enoxaparin group (relative risk [RR] 1.02; 95% confidence interval [CI], 0.78-1.32; P = .06 for noninferiority; difference in risk 0.1%; 95% CI, −2.2-2.4; P < .001). About other efficacy outcomes, the rate of major VTE and all-cause death was, respectively, 2.0% (26 of 1269) and 1.6% (20 of 1216; RR 1.25; 95% CI, 0.70-2.23; difference in risk 0.38%, 95% CI, −0.68-1.40), the rate of symptomatic VTE and VTE-related death was 1.2% (19 of 1599) and 0.8% (13 of 1596; RR 1.46; 95% CI, 0.72-2.95; difference in risk 0.4%, 95% CI, −0.3-1.1), all DVT occurred in 89 (7.8%) of 1142 patients and in 92 (8.2%) of 1122 patients, respectively, all death were 0.2% in both groups (3 of 1599 in the first and 3 of 1596 in the second).
About safety outcome, respectively, in apixaban or enoxaparin group, the rate of adjudicated major bleeding events was 0.7% (11 of 1596) and 1.4% (22 of 1588; with a difference in risk −0.81%, 95% CI, and P = .05), the rate of clinical relevant nonmajor (CRNM) bleeding was 2.2% (35 of 1596) and 3.0% (47 of 1588; with a difference in risk −0.77%, 95% CI) and all bleeding events were 2.9% (46 of 1596) and 4.3% (69 of 1588; adjusted difference in event rates according to type of surgery, −1.46%; 95% CI, −2.75 to −0.17%; P = .03).
In conclusion, the results of ADVANCE 1 support the idea that this NOAC has similar efficacy to enoxaparin 30 mg twice daily with a lower rates of clinically relevant bleeding, even if the noninferiority of apixaban was not demonstrated. Main results of ADVANCE 1 are reported in Figure 1.
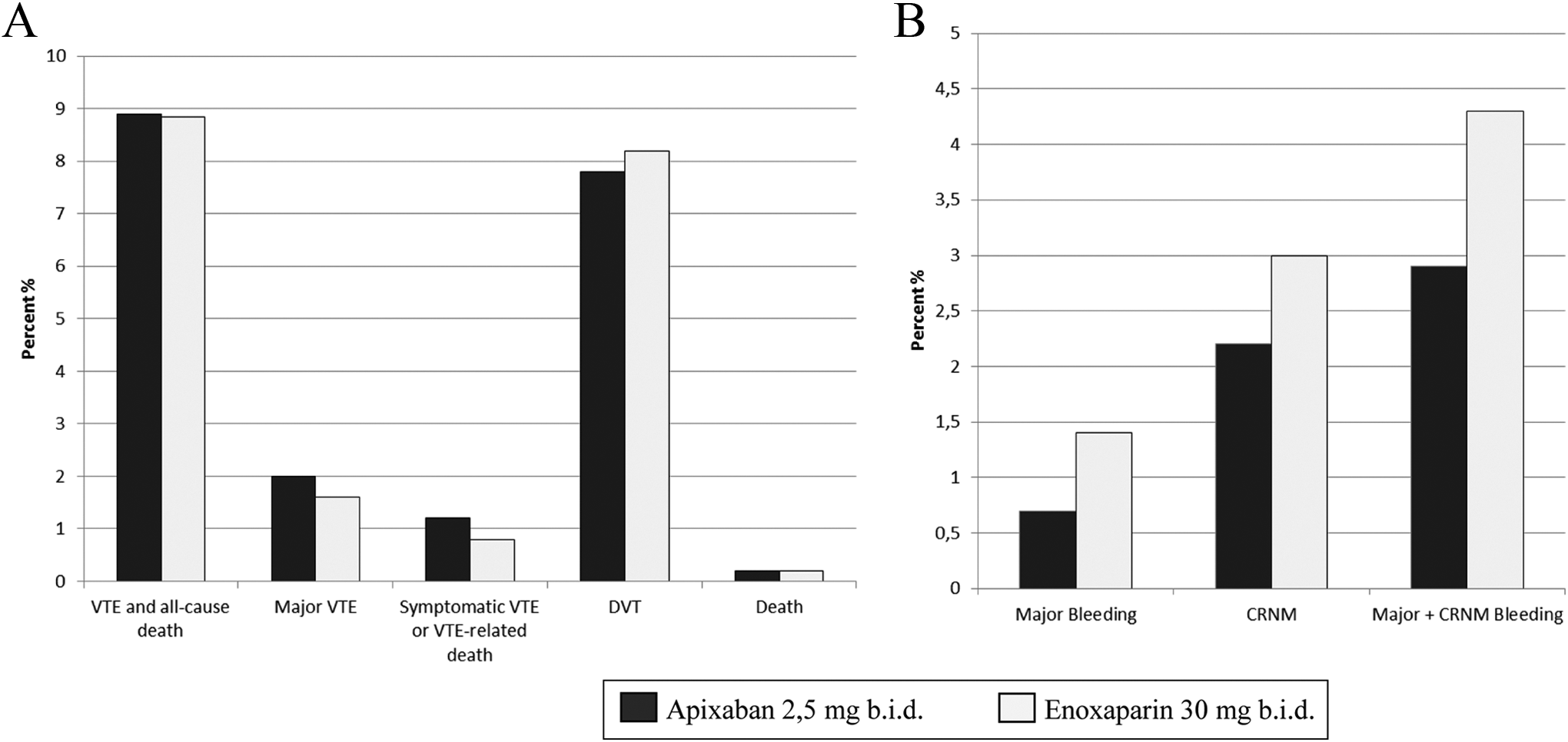
Apixaban for the Prevention of Thrombosis-Related Events (ADVANCE) 1: main efficacy outcomes (A) and main safety outcomes (B).
The ADVANCE 2 clinical trial 11 recruited patients undergoing TKR, but respect to the ADVANCE 1, a different enoxaparin daily dose and timing was planned. In ADVANCE 2, patients were randomized in a double-blind design to receive apixaban 2.5 mg twice daily started 12 to 24 after surgery or enoxaparin 40 mg once daily started 12 hours before surgery (European model). In all, 3057 patients were enrolled and randomized to assume apixaban or enoxaparin for 10 to 14 days.
The rate of all VTE and all-cause death was 15.06% (147 of 976) and 24.37% (243 of 997; RR 0.62, 95% CI, 0.51-0.74, and 1-sided P < .0001 when tested for noninferiority and for superiority) in the apixaban group and in the enoxaparin group, respectively, with a difference in absolute risk of −9.27% (95% CI, −12.74 to −5.79, P < .0001) in favor of apixaban. A reduction in absolute risk of 1.08% for secondary outcome “major VTE and all-cause death” (1.09% in the apixaban group vs 2.17% in the enoxaparin group, RR 0.50, 95% CI, 0.26-0.97, and P = .0186 for superiority) documented a better result for apixaban, while symptomatic VTE and VTE-related death were similar in both groups (0.46%, absolute risk reduction 0%), as well as for all death (0.13% in the apixaban group and 0% in the enoxaparin group).
The rates of safety outcomes were reduced but without statistically significant differences in apixaban versus enoxaparin group: adjudicated major bleeding events were 0.6% in the apixaban group versus 0.9% in the enoxaparin group (absolute risk reduction −0.33 [−0.95-0.29], P = .30), adjudicated clinically relevant nonmajor bleeding events were 2.9% versus 3.8% (absolute risk difference −0.91 [−2.20-0.38], 95% CI, P = .166), and adjudicated major or clinically relevant nonmajor bleeding events were 3.5% versus 4.8% (absolute risk difference −1.24% [−2.66-0.18], P = .088).
Overall, the ADVANCE 2 trial demonstrated that apixaban 2.5 mg twice daily is an anticoagulant treatment more effective than enoxaparin 40 mg once daily in VTE prevention after TKR, without significant increased risk of bleeding. Main results of ADVANCE 2 are reported in Figure 2.
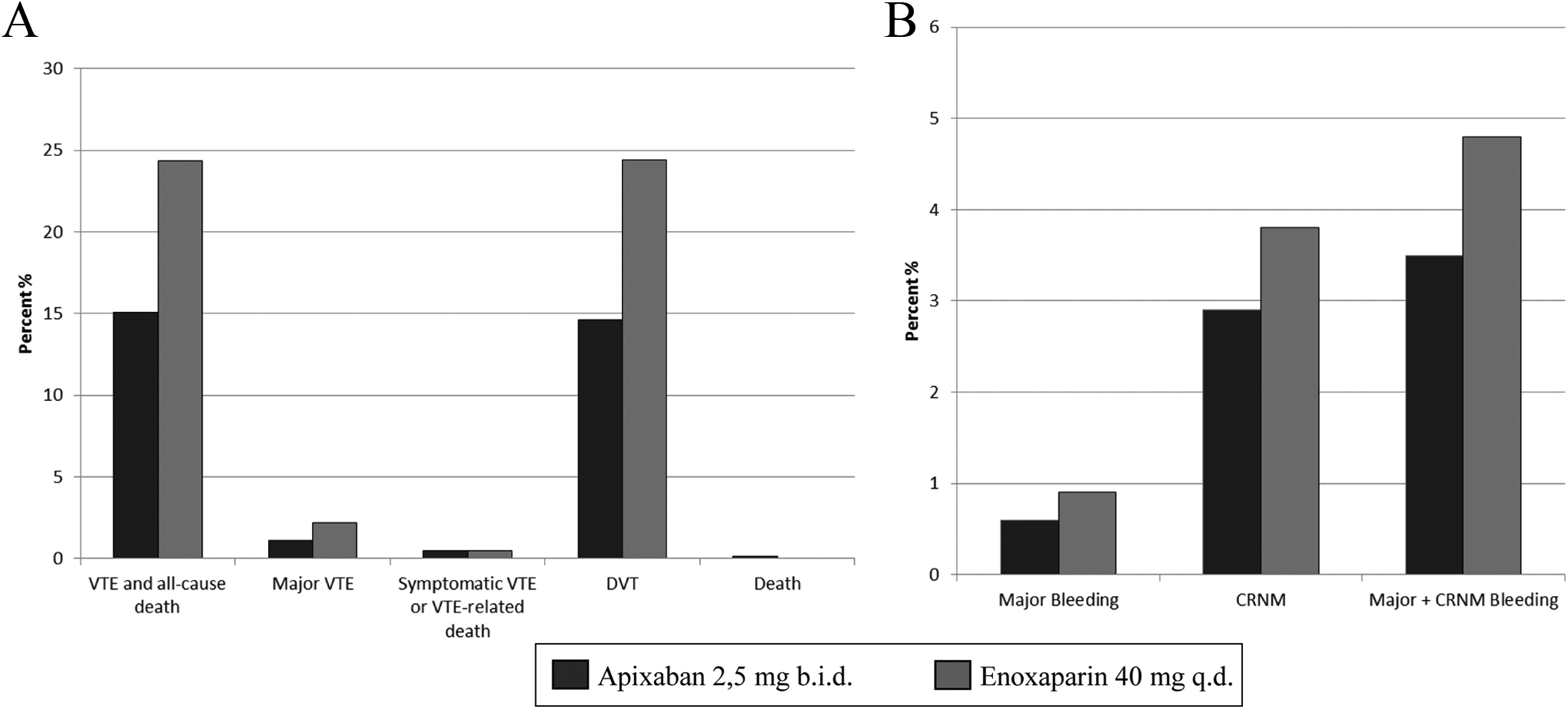
Apixaban for the Prevention of Thrombosis-Related Events (ADVANCE) 2: main efficacy outcomes (A) and main safety outcomes (B).
The ADVANCE 3 clinical trial 12 enrolled patients undergoing THR: 5407 patients were randomized in a double-blind manner to receive either apixaban 2.5 mg twice daily or enoxaparin 40 mg once daily, for 5 weeks after surgery.
Apixaban demonstrated to significantly reduce the primary efficacy end point in all VTE and death from any cause, 1.4% and 3.9%, absolute difference in risk −2.5% (−3.5 to −1.5), P < .001. The secondary efficacy end points occurred less in the apixaban group than in the enoxaparin group but without statistically significant differences (major VTE): 0.5% and 1.1%, respectively, absolute difference in risk −0.7% (−1.3 to −0.2), P = .01; symptomatic VTE and death from VTE were 0.1% and 0.4%, absolute difference in risk −0.2% (−0.6-0.06), P = .11; all DVT were 1.1% and 3.6%; death were 0.1 and <0.1, respectively.
About safety outcomes, the rate of adjudicated major bleeding events, CRNM, and all bleeding events was similar in both the treatment groups. Overall, apixaban has proven to be more effective and as safe as enoxaparin in preventing VTE after THR. Main results of ADVANCE 3 are reported in Figure 3.
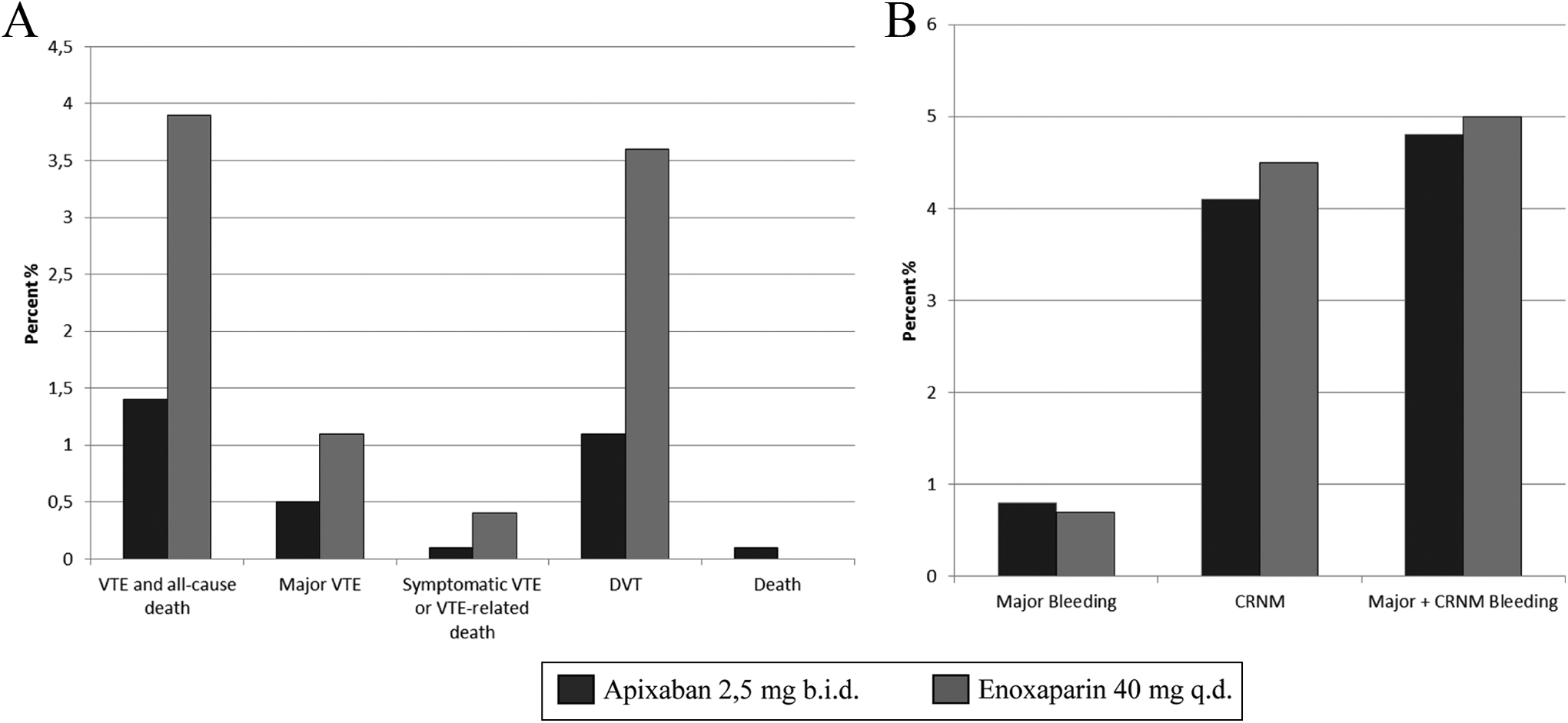
Apixaban for the Prevention of Thrombosis-Related Events (ADVANCE) 3: main efficacy outcomes (A) and main safety outcomes (B).
A recently published meta-analysis 17 analyzed the results of trials APROPOS, ADVANCE 1-2-3, and ADOPT (Study of Apixaban for Prevention of Thrombosis-related Events in Patients with Acute Medical Illness), 18 another study of efficacy and safety of apixaban versus enoxaparin in patients hospitalized for congestive heart failure, acute respiratory failure, and other conditions that increase risk of VTE and reported a higher rate of death and PE in patients treated with apixaban, even in the presence of a better primary efficacy and safety outcome. In fact in ADVANCE 1, 16 had PE in the apixaban group and 7 in the enoxaparin group; in ADVANCE 2, 4 had PE in the apixaban group and 0 in the enoxaparin group; in ADVANCE 3, 5 patients treated with apixaban (2 for PE) and 2 treated with enoxaparin died. These results are not interpretable: more detailed studies, with a greater harmonization of groups, might better explain these concepts.
Analyzing homogeneous groups of patients (like TKR), the difference between the enoxaparin regimen used in ADVANCE 1 and ADVANCE 2 led to an interesting consideration. In ADVANCE 1, enoxaparin 30 mg twice daily seems to be better in VTE prevention than apixaban but it is associated with increased bleeding; conversely in ADVANCE 2, apixaban was more efficacious than enoxaparin 40 mg once daily with the same level of safety. It is not possible to do this evaluation in patients undergoing THR because in this condition apixaban was compared only with enoxaparin 40 mg/death. In conclusion, apixaban 2.5 mg twice daily started after TKR and THR appears more effective than enoxaparin used in accordance to European model, without increased bleeding.
Conclusion
Apixaban is a new anticoagulant inhibiting FXa; it has a good oral bioavailability and it is administered orally in a fixed dose without need of routine coagulation monitoring and minimal drug and food interactions. These characteristics and the relevant results of the ADVANCE program demonstrating a good efficacy and safety profile of apixaban after major orthopedic surgery make its use extremely feasible for VTE prophylaxis after TKR and THR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.