
Abstract
The risk of thromboembolic events after hip revision arthroplasty might be higher than in primary hip arthroplasty. However, evidence regarding the use of thromboprophylaxis in revisions is scarce. The purpose of this study is to determine whether thromboprophylaxis recommendations for primary arthroplasty produce similar results in hip revision arthroplasty. This comparative cohort study retrospectively analyzed consecutive patients undergoing primary hip arthroplasty and hip revision surgery between March 2004 and December 2015, who received thromboprophylaxis according to local clinical practice guidelines for primary hip arthroplasty. The prevalence of deep vein thrombosis and pulmonary embolism and the presence of major bleeding events were assessed during hospitalization and at 3 months after discharge and compared between groups. The overall prevalence of thromboembolic events in the hip revision surgery cohort and in the primary hip cohort was 1.62% and 1.35%, respectively (P = .801). The 38.4% of hip revision patients and 20.3% of primary hip patients presented major bleeding events. Thromboembolic disease outcomes with the use of a standardized thromboprophylaxis regimen were similar in both cohorts, regardless of the high variability of hip revision surgery and the increased risk of complications. Implementation of this regimen is recommended in patients requiring joint replacement revision surgery.
Keywords
Introduction
Growing life expectancy and standardization of perioperative care has increased the number of primary hip arthroplasties performed worldwide. 1,2 As the conclusive outcome of primary procedures is revision surgery, 3 –5 the number of hip revision arthroplasties has increased by 30% in the last 10 years. 1,6,7 While complications after primary hip arthroplasty are widely known and have been successfully managed, the literature regarding hip revision arthroplasty is limited. 2,8 –10
In hip revision surgery, surgical time and insult to soft tissues are higher than in primary procedures. Therefore, there is an elevated risk of complications such as infection, thromboembolic events, major bleeding, and death, 6,11,12 which makes difficult to assess an appropriate risk–benefit balance in the prevention of thromboembolic disease.
From observational retrospective studies on different regimes of thromboprophylaxis, it has been reported that the prevalence of thromboembolic disease after revision surgery ranges between 0.4% and 1.7%. 11 –13 However, the literature available regarding the use of thromboprophylaxis in hip revision surgery does not allow to establish a standardized protocol for prevention of thromboembolic disease in these patients, 14 while for the primary hip arthroplasty, the evidence is extensive. 15
Our main hypothesis is that clinical practice guidelines designed for primary hip arthroplasty yield comparable outcomes when implemented in hip revision arthroplasty. Therefore, the purpose of this study is to determine whether the use of this protocol of pharmacologic and mechanic thromboprophylaxis produces similar results in terms of thromboembolic disease and major bleeding events in primary and revision procedures.
Materials and Methods
This retrospective cohort study analyzed adult patients (18 years and older) who underwent primary or revision hip arthroplasty, for any cause, between March 2004 and December 2015, at an academic general hospital in the department of orthopedics and received thromboprophylaxis during the postoperative period according to local clinical practice guidelines.
Patients receiving chronic anticoagulation therapy, blood dyscrasias, or coagulation disorders, patients requiring additional surgical procedures during hospitalization, patients undergoing conversion to joint arthroplasty for osteosynthesis failure, and patients with a history of primary joint arthroplasty for oncologic pathology were excluded.
All consecutive patients who underwent hip revision arthroplasty and met the inclusion criteria during the period of study were included in the revision cohort. The primary hip arthroplasty cohort comprised patients who underwent this procedure during the same period and were randomly selected from the Institutional Arthroplasty Registry database, considering a 1:3 ratio.
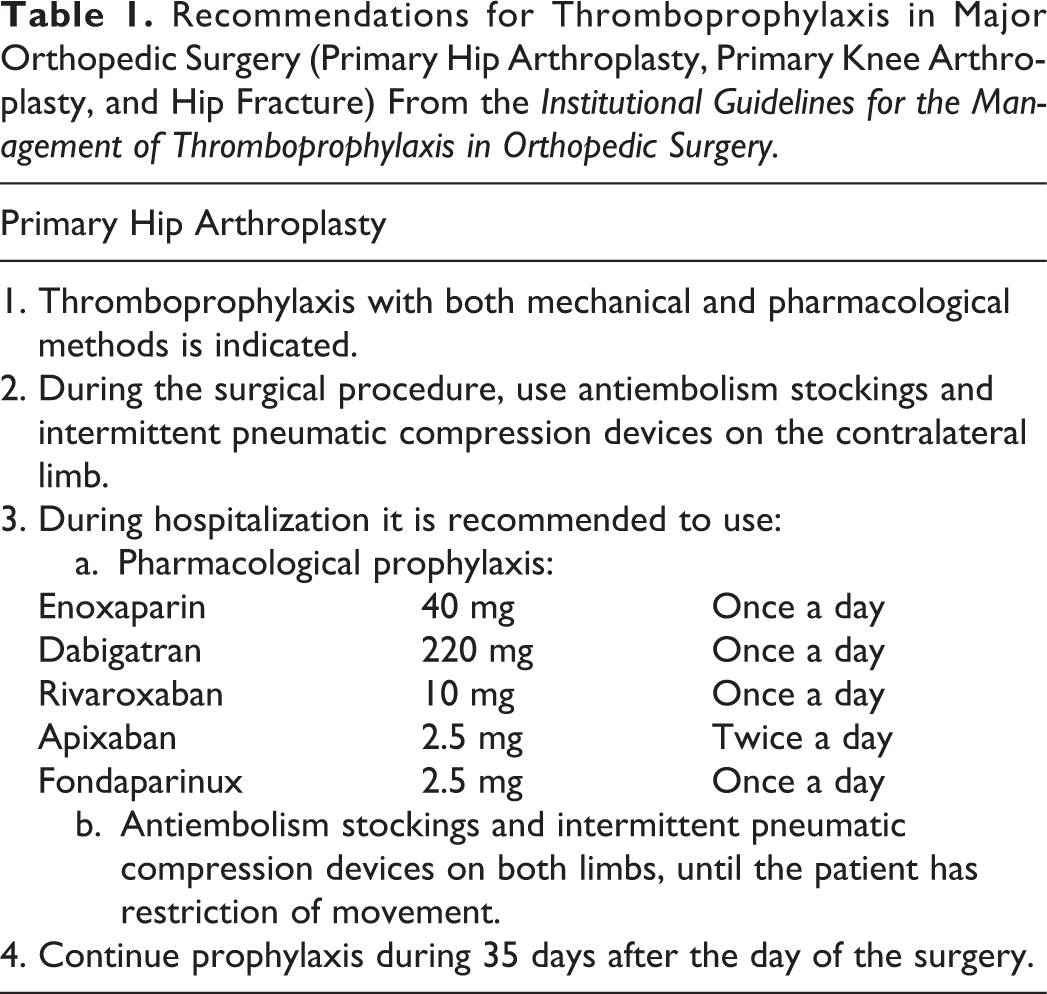
Venous thromboembolism prophylaxis was performed according to local clinical practice guidelines, which includes the use of mechanical and pharmacological strategies. As mechanical methods, both stockings and intermittent pneumatic sequential graduated compression to calf (Kendall SCD Compression System; Medtronic, Minnesota, US) were used, in addition to pharmacological methods such as enoxaparin (40 mg every day), fondaparinux (2.5 mg every day), rivaroxaban (10 mg every day), dabigatran (220 mg every day), or apixaban (2.5 mg twice a day). Enoxaparin, fondaparinux, and rivaroxaban were initiated 6 hours after the end of the procedure, dabigatran was initiated after 4 hours, and apixaban after 12 hours (Table 1) and continued for 35 days postoperatively. The type of pharmacological agent was selected at the discretion of the surgeon.
Recommendations for Thromboprophylaxis in Major Orthopedic Surgery (Primary Hip Arthroplasty, Primary Knee Arthroplasty, and Hip Fracture) From the Institutional Guidelines for the Management of Thromboprophylaxis in Orthopedic Surgery.
For both groups, gender, age, body mass index (BMI), health status according to the American Society of Anesthesiologists (ASA) classification, comorbidities, surgical time, intraoperative bleeding, and use of mechanical and pharmacologic prophylaxis were assessed. Major bleeding events and the presence of thromboembolic events were assessed during hospitalization and at any time during the first 3 months after discharge. Outcomes were identified from both medical records and by a telephonic survey. If any of those was positive, the patient was classified as having an event.
Major bleeding was defined according to European Medicines Agency (Table 2). Thromboembolic disease was defined as the presence of symptomatic deep vein thrombosis (DVT) confirmed by Doppler ultrasound, pulmonary embolism (PE) confirmed by computed tomography angiography, or ventilation/perfusion scan or death caused by thromboembolism.
European Medicines Agency Criteria for Major Bleeding.

Statistical Analysis
Demographic characteristics and comorbidities are reported using means, ranges, standard deviations, and proportions. As intraoperative bleeding does not follow a normal distribution, it is reported as a median and its respective interquartile range (IQR) and compared between groups using the Mann-Whitney U test. Demographic and clinical variables were compared using Student t test or χ2 test as appropriate, in order to assure that study groups were comparable. The presence of thromboembolic disease or major bleeding events is presented as prevalence. These outcomes were compared between cohorts using a χ2 test. Values of P .05 or less were considered as statistically significant. Additionally, to test for type I error, a χ2 post hoc analysis was conducted; adjusted P values were obtained in order to further determine whether the differences between cohorts were statistically significant. Data were processed using the software IBM SPSS Statistics version 21 (IBM Corporation, Armonk, New York).
Study patient’s informed consent was not applicable according to local regulations. Institutional ethics committee approval was granted to this protocol before it was initiated.
Results
From the 209 hip revision and 558 primary hip procedures identified during the period of study, 185 and 370 patients, respectively, were included in the analysis (Figure 1). The main cause of revision was aseptic loosening (46.5%) and the main cause of primary hip arthroplasty was idiopathic osteoarthritis (40%).
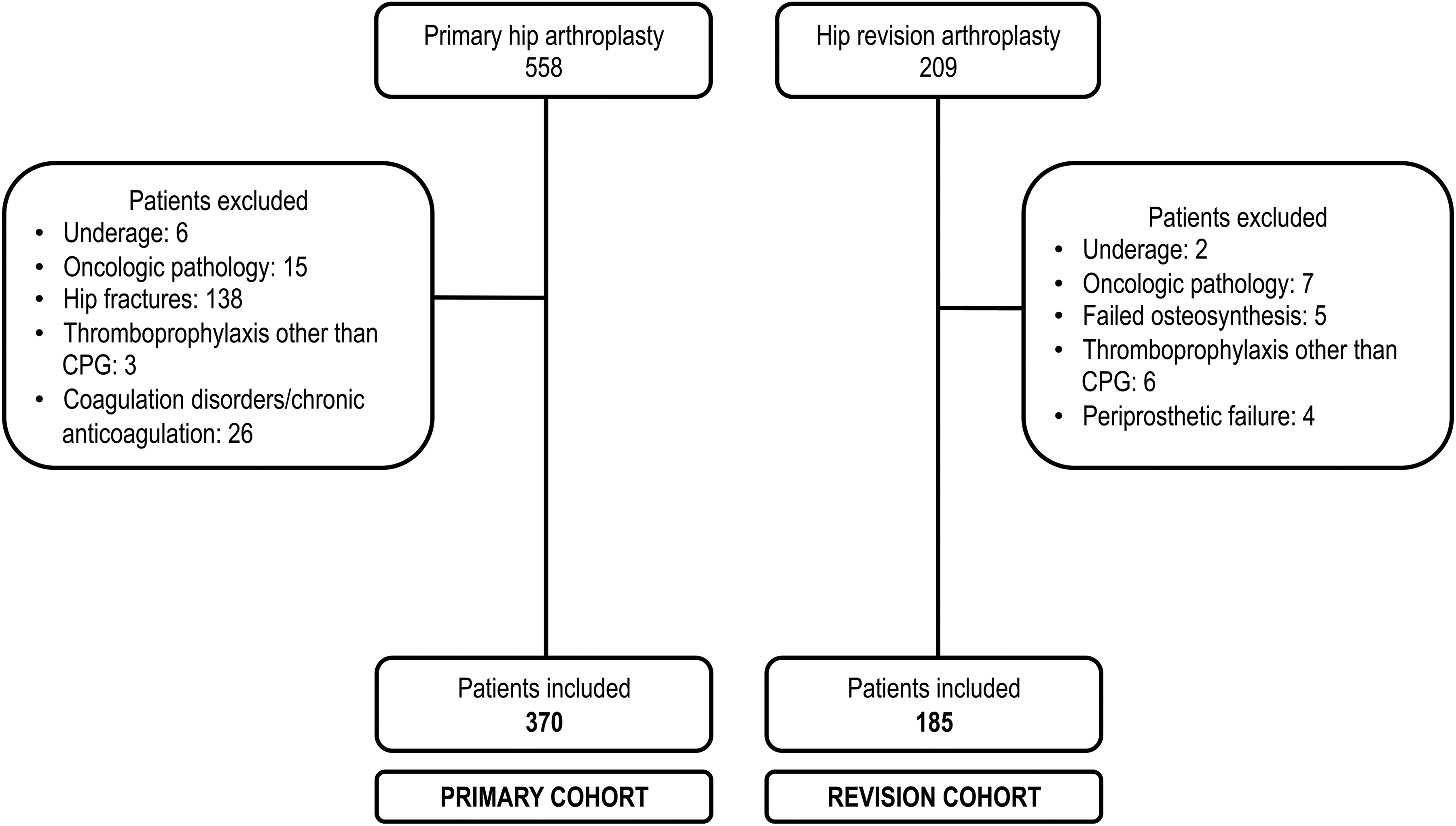
Patient selection flowchart.
Demographic characteristics were homogenous in the 2 cohorts. Mean age at the time of surgery for the revision cohort was 66.2 (range: 30-95) years and 66.1 (range: 29-92) years for the primary cohort. Females represented the 60.5% of patients in the revision cohort and the 70% in the primary cohort. Mean BMI in the revision cohort was 27.71 (19.3) kg/m2 and 25.96 (4.2) in the primary cohort. The 62.1% of patients in the revision cohort and 49.1% of patients in the primary cohort were classified as ASA II. The mean surgical time was 305 (93) minutes and 190 (43) minutes, respectively. Median intraoperative bleeding was 800 mL (IQR: 400-1500) for revisions and 400 mL (IQR: 300-600) for primary arthroplasty. Statistically significant differences between revision and primary hip arthroplasty cohorts were found in terms of ASA classification, surgical time, and intraoperative bleeding. These differences are expected since primary surgery and revision surgery are different procedures usually performed in slightly different populations. Other variables that might increase the risk of thromboembolic disease 16 were comparable within groups (Table 3).
Demographic and Clinical Characteristics of the Patients Included in the Study.
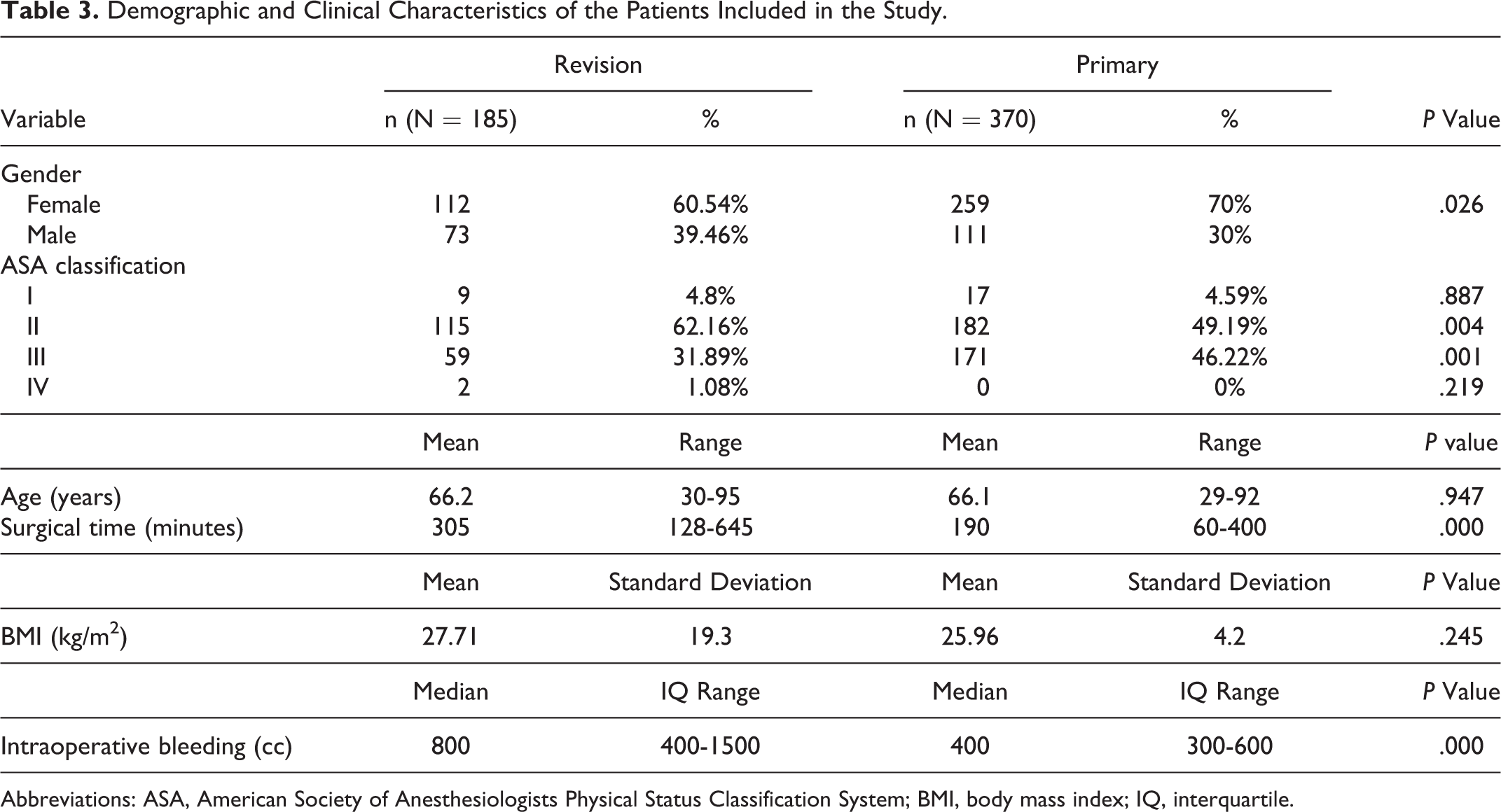
Abbreviations: ASA, American Society of Anesthesiologists Physical Status Classification System; BMI, body mass index; IQ, interquartile.
Regarding the presence of comorbidities, 55.9% of all patients had a history of cardiovascular disease, 7.03% had a history of cancer, 5% had a history of peripheral vascular disease, and 2.16% had renal comorbidities. The 47.8% of patients had 2 or more comorbidities. None of the hematological comorbidities reported in this study was related to coagulation disorders (see exclusion criteria). Table 4 describes the distribution of comorbidities in each cohort.
Distribution of Comorbidities and Related Diagnoses of Patients Included in the Hip Revision Surgery Group and the Primary Arthroplasty Group.

All patients (100%) received pharmacological thromboprophylaxis and received mechanical prophylaxis with stockings and pneumatic compression devices. In the hip revision arthroplasty cohort, 24.32% received fondaparinux, 33.51% enoxaparin, 39.46% rivaroxaban, and 2.7% apixaban. In the primary hip arthroplasty cohort, 25.41% received fondaparinux, 16.49% enoxaparin, 52.97% rivaroxaban, 1.62% dabigatrán, and 3.51% apixaban (Figure 2).

Use of the different types of anticoagulant agents.
Of all patients included in the analysis, 38.4% from the revision cohort and 20.3% from the primary cohort presented major bleeding events, mainly defined by the requirement of transfusion of 2 or more units of red blood cells throughout the hospitalization (P < .05). The overall prevalence of thromboembolic events in hip revision arthroplasty and primary hip arthroplasty was 1.62% and 1.35%, respectively (P = .801). During hospitalization, none of the patients in the primary arthroplasty cohort (0%) and 2 patients in the revision arthroplasty cohort (0.27%) presented DVT (P = .479), diagnosed at the third day after surgery; one (0.54%) revision arthroplasty patient (diagnosed during the second day after surgery) and 2 (0.54%) primary arthroplasty patients had nonfatal PE (P = 1.000; diagnosed at the second and third postoperative day). At 3 months of follow-up after discharge, none (0%) of the patients in the revision arthroplasty cohort and 2 (0.54%) patients in the primary arthroplasty cohort presented DVT (P = .316; diagnosed 3 and 9 weeks after discharge); 2 patients in the revision arthroplasty cohort (1.08%; diagnosed 3 and 4 weeks after discharge) and 1 patient in the primary arthroplasty cohort (0.27%; diagnosed 8 weeks after discharge) presented with nonfatal PE (P = .219). The prevalence of thromboembolic events was not statistically significantly different between groups. Furthermore, after performing a χ2 post hoc test for type II error, adjusted P values obtained were not different either (Table 5).
Prevalence of Overall Thromboembolic Events in the Hip Revision Surgery Group and the Primary Arthroplasty Group and Prevalence at the Different Follow-Ups.

Discussion
Variability in hip revision surgery represents an additional challenge to mitigate the elevated risk of postoperative complications, in comparison to primary procedures, 6,12 which is in turn associated with increased costs of the procedure. 6,7 In a prospective study of national registries, the authors reported that patients undergoing revision surgery had a relative risk of 2.13 (95% CI: 1.05-4.32) of presenting deep venous thrombosis, as well as an increased risk of infection, major bleeding, transfusion, and postoperative death, compared to primary surgery. 12 This might be due to the fact that these patients are exposed to a longer surgical time, undergo greater soft tissue injury, have more restrictions of mobility, and their overall status of health is poorer. 6,11,12
Deirmengian et al 11 compared the rate of thromboembolic events with the use of warfarin and aspirin in a similar population and identified an increase in the risk of the occurrence of this complications in the group of patients who received warfarin (OR: 3.2; 95% CI: 1.03-16.3), and the authors conclude that the use of aspirin might be enough to prevent these events. However, in comparison with the results obtained in our cohort of hip revision surgery, in the aforementioned study, a lesser proportion of patients presented PE during hospitalization and a higher proportion of them presented general thromboembolic events. Therefore, it is possible that the use of aspirin and mechanical thromboprophylaxis might not be enough for the prevention of thromboembolic events. 15
Although some authors conclude that the use of more potent anticoagulants is not enough either, 17,18 in our cohort of hip revision arthroplasty patients, an overall prevalence of thromboembolic events of 1.62% was found. This prevalence is comparable with that reported in the literature for primary hip arthroplasty, in which a standardized scheme of thromboprophylaxis was used. 19,20
Regarding major bleeding events, 71 cases, defined by the requirement of transfusion of 2 or more units of red blood cells, were found. This prevalence is comparable to what has been reported by Mahadevan et al 21 and Schwartz et al. 12 However, it is not possible to attribute all these cases to the use of anticoagulants, due to the increased risk of bleeding inherent to the procedure, 6,12,21 given the statistically significant difference in the amount of intraoperative blood loss and surgical time in both cohorts, as well as the difference in the ASA classification.
To our knowledge, this is the first description in the literature of the prevalence of thromboembolic and bleeding events in patients undergoing hip revision surgery and receiving a standardized protocol of thromboprophylaxis recommended for primary procedures, which includes low-molecular-weight heparins, fondaparinux, and oral anticoagulants, 22 obtaining acceptable results in terms of efficacy and safety.
One of the main limitations of this study to determine the effect of the scheme of thromboprophylaxis is the low frequency of thromboembolic events and the sample size. After the χ2 post hoc analysis, adjusted P values showed nonsignificant differences (P > .05; Table 5). In the view of these results, it is possible that the power of this study might be insufficient to establish a statistically significant difference in the prevalence of these complications. In order to detect a difference of less than 1% between cohorts, at least 3302 patients would be required for each group. However, even if statistical significance could be demonstrated, this difference would only represent a clinical problem if the frequency of thromboembolic disease in revision surgery were 3 times higher than in primary surgery. Another potential limitation is that compliance to postoperative thromboprophylaxis was not assessed; however, due to a quality improvement program previously published by our group, 23 our current compliance is over 90%, and given the fact that both primary and revision patients received the same recommendations, a difference in the rate of compliance between groups is not expected. Lastly, due to an increase in the number of surgeons and patients operated during the study period, there is a higher proportion of patients who received rivaroxaban; furthermore, the primary group received more rivaroxaban, while the revision group received more enoxaparin, resulting in a slight difference in outcomes of both thromboembolic and bleeding events.
In addition, the design of the study and its temporal character does not allow to build causality relationships or to quantify the effectiveness of the treatment. By not including a control group, it is not possible to directly compare between the use of thromboprophylaxis and other strategies, or between drug types. However, its main strength is the comparability between the 2 cohorts of patients undergoing different surgical interventions but receiving the same thromboprophylaxis protocol, allowing the identification of a similar prevalence of the disease in both groups.
In conclusion, the implementation of thromboprophylaxis designed for primary hip arthroplasty in patients undergoing hip revision surgery results in a low rate of DVT and PE. However, in our study, the rate of major bleeding events was significantly higher in revision procedures. Whether this difference is due to the performance of a greater magnitude of surgery or the administration of anticoagulant medication is beyond the scope of this study. Therefore, the decision of thromboprophylaxis strategies for hip revision surgery must be the result of an individual risk–benefit analysis.
The use of the thromboprophylaxis strategies has been included in international clinical practice guidelines 15,24,25 and is universally available, which ensures the applicability of these results in other populations.
The use of a standardized protocol of thromboprophylaxis designed for primary hip arthroplasty produces similar results in a group of patients undergoing hip revision surgery, even with the high variability entailed in this procedure and the increased risk of developing deep venous thrombosis and pulmonary thromboembolism. The implementation of this scheme for the prevention of thromboembolic disease in patients who require hip revision arthroplasty is recommended.
Footnotes
Acknowledgment
The author would like to thank Alejandra Forero, MD, for her contributions in the editing, provision of comments, and assembling of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Maria Bautista has received royalties for research support from a company or supplier as a principal researcher from Grunenthal and DePuy Synthes (Orthopedics), and other financial support from Grunenthal and Abbott. Guillermo Bonilla has participated as paid speaker for Boehringer-Ingelheim, Pfizer, Sanofi, and DePuy Synthes (Orthopedics); has received other financial support from DePuy Synthes (Orthopedics); and has received research support from a company or supplier as a principal researcher for Grunenthal and DePuy Synthes (Orthopedics), outside this work. Adolfo Llinás has received royalties from Innomed, Novamed, and 3M; has participated as paid speaker for Zimmer, Shire, Novonordisk, Novartis, DePuy Synthes (Orthopedics), Medtronic, and Procaps; has participated as paid consultant for Zimmer and Medtronic, outside this work.