
Abstract
A real-world US database analysis was conducted to evaluate the hospital resource utilization and costs of patients hospitalized for venous thromboembolism (VTE) treated with warfarin versus apixaban. Additionally, 1-month readmissions were evaluated. Of 28 612 patients with VTE identified from the Premier Hospital database (August 2014-May 2016), 91% (N = 26 088) received warfarin and 9% (N = 2524) received apixaban. Outcomes were assessed after controlling for key patient/hospital characteristics. For index hospitalizations, the average length of stay (LOS) was longer (3.8 vs 3.1 days, P < .001; difference: 0.7 days) and mean hospitalization cost higher (US$3224 vs US$2,740, P < .001; difference: US$484) for warfarin versus apixaban-treated patients. During the 1-month follow-up period, warfarin treatment was associated with a greater risk of all-cause readmission (odds ratio [OR]: 1.27; 95% confidence interval [CI]: 1.09-1.48, P = .003), major bleeding (MB)-related readmission (OR: 2.10; 95% CI: 1.03-4.27, P = .04), and any bleeding-related readmission (OR: 1.67; 95% CI: 1.09-2.56, P = .02) versus apixaban. The results of this real-world analysis show that compared to warfarin, apixaban treatment was associated with shorter index hospital stays, lower index hospitalization costs, and reduced risk of MB-related readmissions among hospitalized patients with VTE.
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common cardiovascular occurrence and a significant public health concern affecting up to 900 000 people in the United States every year. 1,2 In 2011, the total annual cost for VTE was estimated to range between US$13.5 and US$27.2 billion in the United States. 3 Patients experiencing VTE have a high risk of recurrence, with observational cohort studies reporting cumulative incidence of recurrence of 25% after 5 years and 30% after 10 years after initial VTE. 4,5 To prevent VTE recurrence, it is recommended to treat patients with anticoagulation therapy; however, anticoagulation therapy increases the risk of bleeding. 6
In the clinical trial, Apixaban for the Initial Management of Pulmonary Embolism and Deep-Vein Thrombosis as First-Line Therapy (AMPLIFY), apixaban treatment was compared to enoxaparin/warfarin. 7 The findings were that apixaban had a noninferior risk of recurrent VTE and a significantly lower risk of major bleeding (MB). 7 In a secondary analysis of patients in the AMPLIFY trial, apixaban versus enoxaparin/warfarin treatment was also shown to be associated with a signficantly lower likelihood for all-cause hospitalizations over 6 months and a shortened hospital stay after adjusting for differences in patient characteristics. 8
Some recent real-world studies have evaluated hospitalization outcomes among patients with VTE who were treated with rivaroxaban versus other anticoagulants 9 –12 ; however, no such comparisons with apixaban in the real-world setting have been published. Patients in clinical trials often differ in many respects from patients treated in the real-world setting and also bleeding rates are higher in routine clinical practice than reported in clinical trial settings. 7,13 Thus, studies investigating the clinical and economic burden of bleeding among patients with VTE treated with other oral anticoagulants versus apixaban in real-world settings are warranted. Additionally, many aspects of hospital readmissions are of concern in the United States, including how these relate to quality of care and financial penalties, especially with regard to readmissions occurring within 1 month of hospitalization. It is therefore important to better understand the clinical and economic burden of hospital readmissions among patients with VTE. To address these topics, we conducted a real-world US database analysis to evaluate the hospital resource utilization, measured by using length of stay (LOS), and associated costs of patients hospitalized for acute VTE and treated with warfarin versus apixaban. We also evaluated the rates of all-cause, MB-related, any bleeding-related, and VTE-related readmissions occurring within 1 month after hospital discharge; assessed the associated hospital resource utilization; and estimated the associated hospital costs.
Methods
Study Population
This study was a retrospective cohort analysis that used hospital records data from the Premier Hospital database between August 1, 2013, and June 30, 2016. The Premier Hospital database is the largest inpatient drug utilization database in the United States and contains complete billing and coding history for more than 45 million hospital inpatient discharges (approximately 15%-20% of all discharges annually in the United States). 14 Detailed hospital information contains billing information on a patient’s hospital stay, including a date-stamped log of all billed items (eg, medications, laboratory, diagnostic, and therapeutic services); primary and secondary diagnoses (admission and discharge) for each patient’s hospitalization; demographic; and payer information. The 600+ hospitals represented in the database are generally considered nationally representative with respect to bed size, geographical region, location (urban/rural), and teaching hospital status. 14
Patients (≥18 years of age) with a hospital or emergency department (ED) discharge International Classification of Diseases (ICD)-9 or ICD-10 code indicating a primary diagnosis of VTE (see appendix) were identified between August 1, 2014, and May 31, 2016. Patients who received warfarin or apixaban during any time of the hospitalization (from admission to discharge) were selected and grouped into 2 study cohorts based on the oral anticoagulant received. The first of such VTE hospitalizations with warfarin or apixaban treatment for a patient was defined as the index VTE hospitalization. The baseline period was defined as 12 months prior to the index admission date and was used to measure prior bleeding and VTE events. Other patient characteristics were measured using the discharge records of the index hospitalization. Patients were followed for a 1-month follow-up period after they were discharged from their index VTE hospitalization
Patients were excluded from the study population if they received both warfarin and apixaban during the index hospitalization to ensure both cohorts were mutually exclusive; received any other direct oral anticoagulant including rivaroxaban, dabigatran, or edoxaban during the index hospitalization; had any primary or secondary discharge diagnosis code for atrial fibrillation/atrial flutter, pregnancy, or records of inferior vena cava filter usage during the index hospitalizations or the baseline period; or had been transferred from other acute care facilities.
Patient Demographics, Clinical Characteristics, and Hospital Characteristics
Patient demographics, clinical characteristics, and hospital characteristics were evaluated during the index hospitalization and/or baseline period for each patient in the study cohorts.
Hospital Resource Use and Cost Measurements
The hospital LOS and associated cost for the index VTE hospitalization were evaluated for study cohorts.
Additionally, the proportions of patients with all-cause, MB-related, any bleeding-related, and VTE-related hospital readmissions (either inpatient hospital or ED readmission) occurring within 1 month postdischarge from the index hospitalization were evaluated. LOS and hospitalization costs associated with all readmission categories were also determined. MB- and VTE-related readmissions were defined as readmissions with a bleeding diagnosis and VTE diagnosis, respectively, at the primary position of the discharge ICD-9/ICD-10 diagnosis codes. Any bleeding-related readmission was defined as a bleeding diagnosis in either primary or secondary positions of the hospital discharge diagnosis codes. All hospitalization costs were inflation adjusted to 2016 US dollars using Consumer Price Index Medical Care component. 15
Statistical Analyses
We used descriptive statistics to describe demographics, clinical characteristics, hospital characteristics, hospital LOS, hospitalization costs, and readmission rates among patients with VTE cohorts treated with warfarin or apixaban. The t tests and χ2 tests were used to detect statistically significant differences in continuous and categorical variables, respectively.
We conducted multivariable logistic regression analyses to evaluate the association of warfarin versus apixaban treatment with the occurrence of hospital readmission (all-cause, MB-related, any bleeding-related, and VTE-related) within 1 month postdischarge while controlling for key patient and hospital characteristics.
We also conducted multivariable generalized linear models (GLM) to examine the association of warfarin versus apixaban index treatment with hospital LOS and costs of index hospitalizations and hospital LOS of readmissions while controlling for key patient and hospital characteristics. We used 2-part model regression analyses to evaluate the costs associated with hospital readmissions (all-cause, MB-related, any bleeding-related, and VTE-related) while controlling for key patient and hospital characteristics. In the GLM regressions, log transformation and gamma distribution were used for the analysis of the index hospital costs; negative binomial distribution was used for the analysis of index hospital LOS. Covariates in the regression analyses included age, gender, race, payer type, index Charlson Comorbidity Index score group, prior VTE, and bleeding diagnoses during baseline, baseline MB risk level (as described in the CHEST guidelines), 6 prior surgery within 3 months before index date, index hospitalization VTE type, and hospital characteristics (geographic region, rural/urban status, teaching status, admission type and source, and bed size). An α value of .05 was used to determine statistical significance. All statistical analyses were carried out using SAS 9.4.
We additionally conducted a sensitivity analysis for bridging warfarin patients, in which only patients treated with warfarin and other parenteral anticoagulant therapy (low-molecular-weight heparin, unfractionated heparin, or fondaparinux) during index hospitalizations were included in the warfarin cohort.
Results
Overall Study Population
Of the 28 612 patients included in the study, 91% (N = 26 088) received warfarin and 9% (N = 2524) received apixaban.
Patient Demographics, Clinical Characteristics, and Hospital Characteristics
Demographics and clinical characteristics of patients in the warfarin and apixaban cohorts are shown in Table 1. The mean age was lower for patients treated with warfarin versus apixaban (61.2 vs 63.1 years, P < .001); however, mean Charlson Comorbidity Index score was higher (1.7 vs 1.5, P = .008). A lower proportion of patients in the warfarin cohort compared to the apixaban cohort was white (70.5% vs 74.5%, P < .001), and fewer patients in the warfarin cohort had commercial (26.7% vs 30.4%, P < .001) or Medicare (50.4% vs 52.9%, P < .001) insurance coverage than the apixaban cohort. The distribution of the VTE event types requiring hospitalization did not significantly differ among the study cohorts (DVT: 33.5% vs 35.4%; PE: 36.6% vs 36.3%; DVT/PE: 30.0% vs 28.3%, P = .09).
Baseline Patient Demographics and Clinical Characteristics of Study Cohorts.
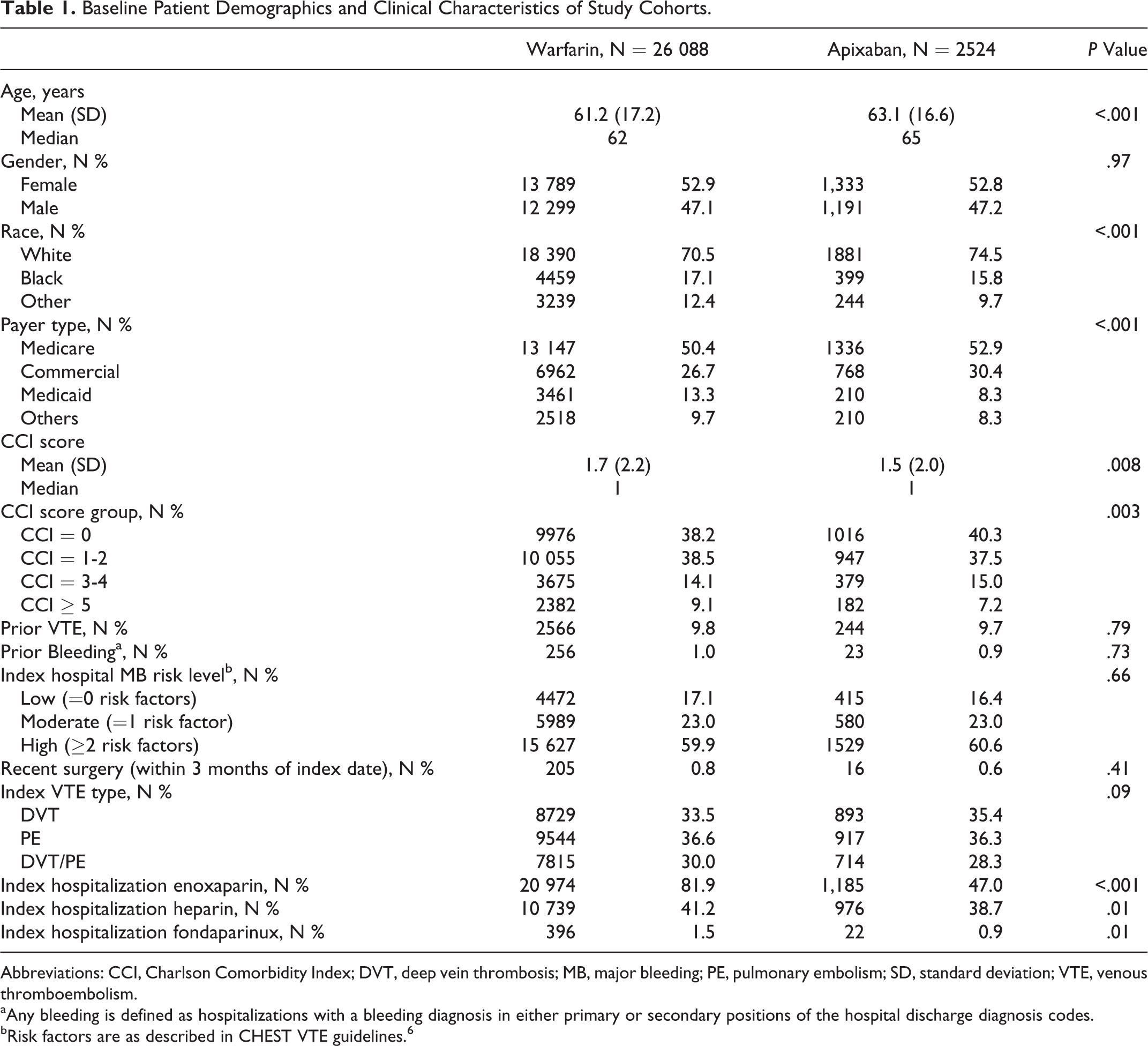
Abbreviations: CCI, Charlson Comorbidity Index; DVT, deep vein thrombosis; MB, major bleeding; PE, pulmonary embolism; SD, standard deviation; VTE, venous thromboembolism.
aAny bleeding is defined as hospitalizations with a bleeding diagnosis in either primary or secondary positions of the hospital discharge diagnosis codes.
bRisk factors are as described in CHEST VTE guidelines. 6
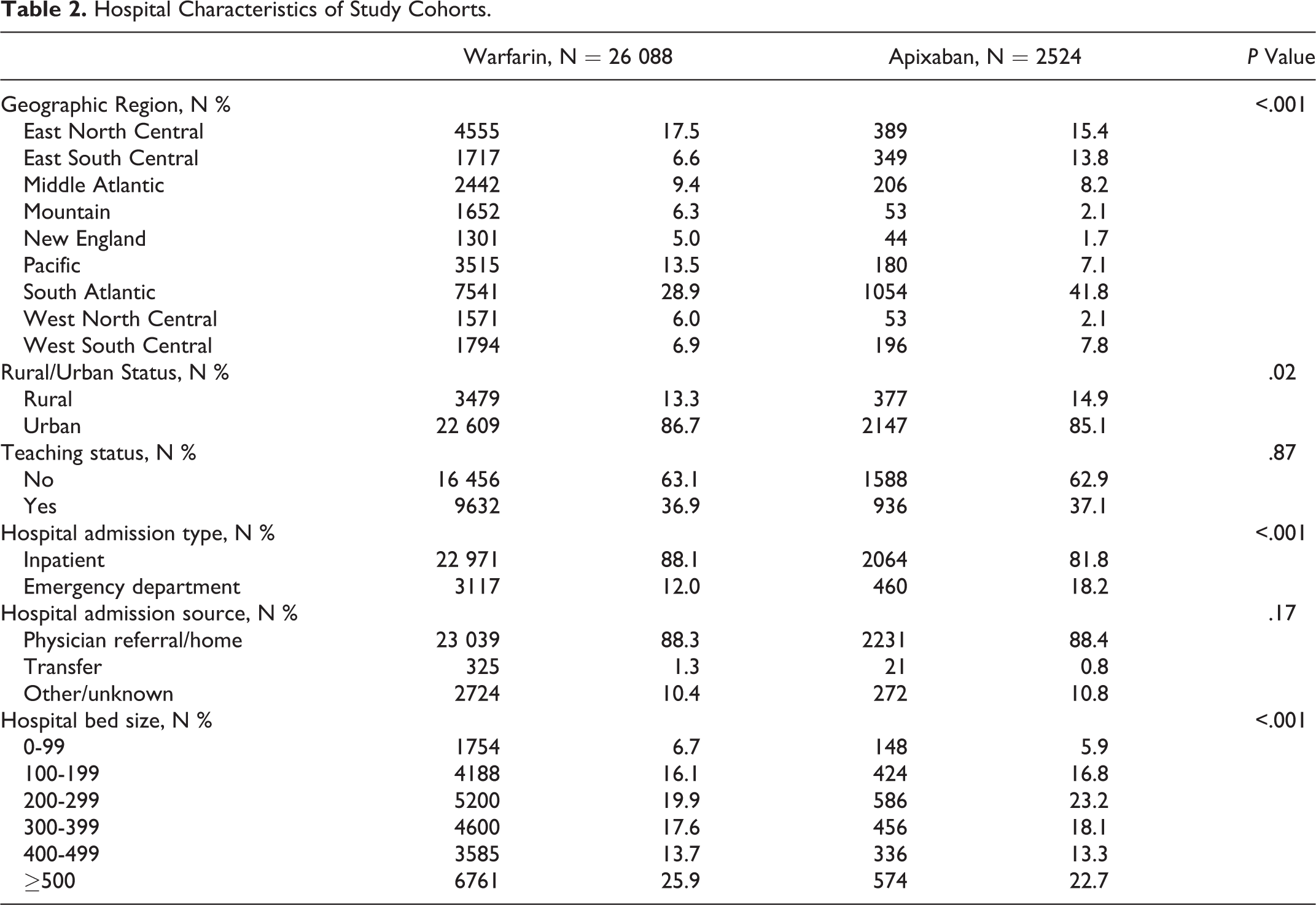
Hospital characteristics of the warfarin and apixaban cohorts are shown in Table 2. Compared to the apixaban cohort, slightly fewer patients treated with warfarin received care in rural hospitals (13.3% vs 14.9%, P = .02) and in hospitals with <300 beds (42.7% vs 45.9%, P < .001).
Hospital Characteristics of Study Cohorts.
Index Hospital Resource Utilization and Associated Cost
The unadjusted average LOS was longer per patient (4.3 vs 2.9, P < .001), and mean hospitalization cost was higher per patient (US$8167 vs US$6422, P < .001) for the index VTE hospitalization of patients treated with warfarin versus apixaban. After controlling for key patient and hospital characteristics, per patient, the average LOS for the index VTE hospitalization remained significantly longer (3.8 vs 3.1 days, P < .001; difference: 0.7 days; 95% confidence interval [CI]: 0.5-0.9), and the mean hospitalization cost was higher (US$3224 vs US$2740, P < .001; difference: US$484; 95% CI: US$228-US$740) for those treated with warfarin versus apixaban (Figure 1).
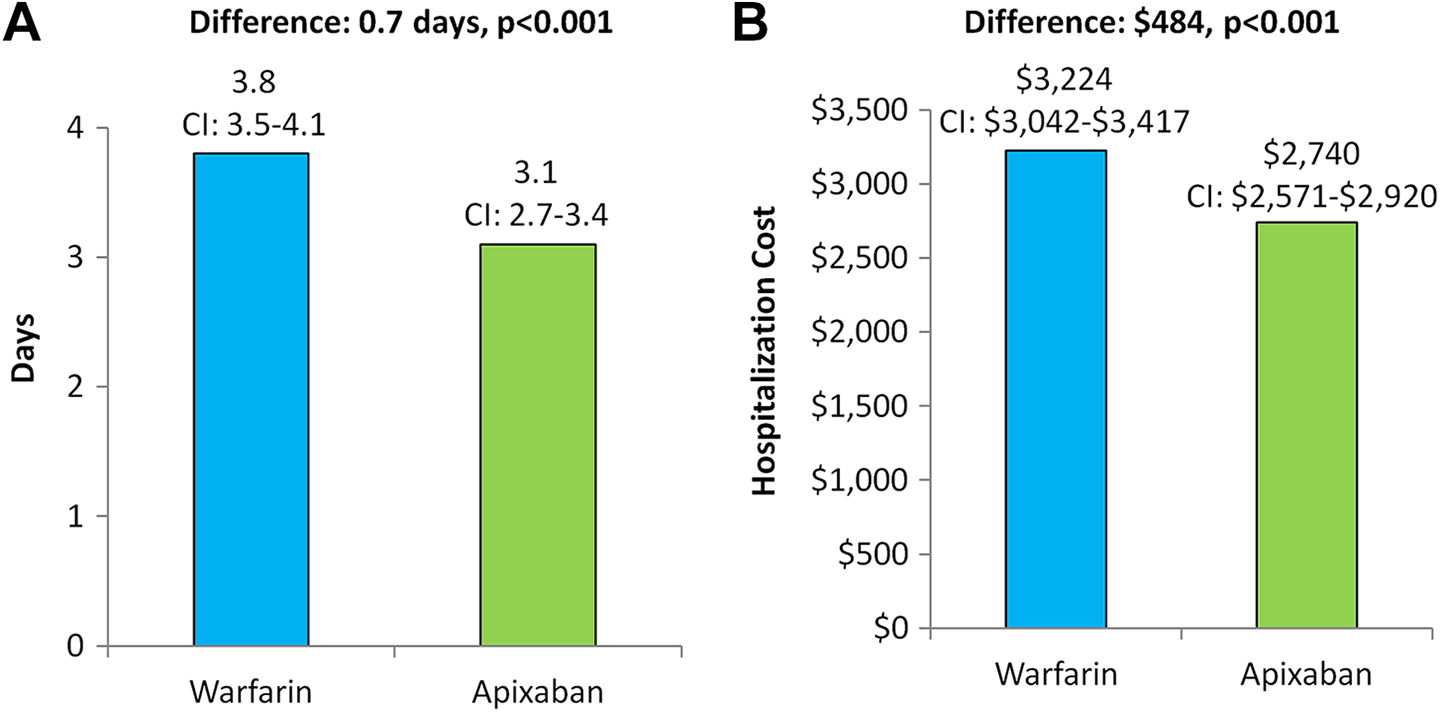
Regression-adjusted average hospital length of stay (LOS) (A) and mean hospitalization cost (B) for index VTE hospitalization per patient. VTE indicates venous thromboembolism.
Readmission Rates
The unadjusted readmission rates within 1 month of the index hospitalization were higher for all-cause (10.0% vs 7.7%, P < .001), MB-related (0.7% vs 0.3%, P = .02), and any bleeding-related (1.6% vs 0.9%, P = .006) readmissions for patients treated with warfarin versus apixaban (Figure 2A). Although numerically lower for apixaban, the rate of VTE-related readmission did not differ significantly between the study cohorts (4.3% vs 3.6%, P = .12; Figure 2A).
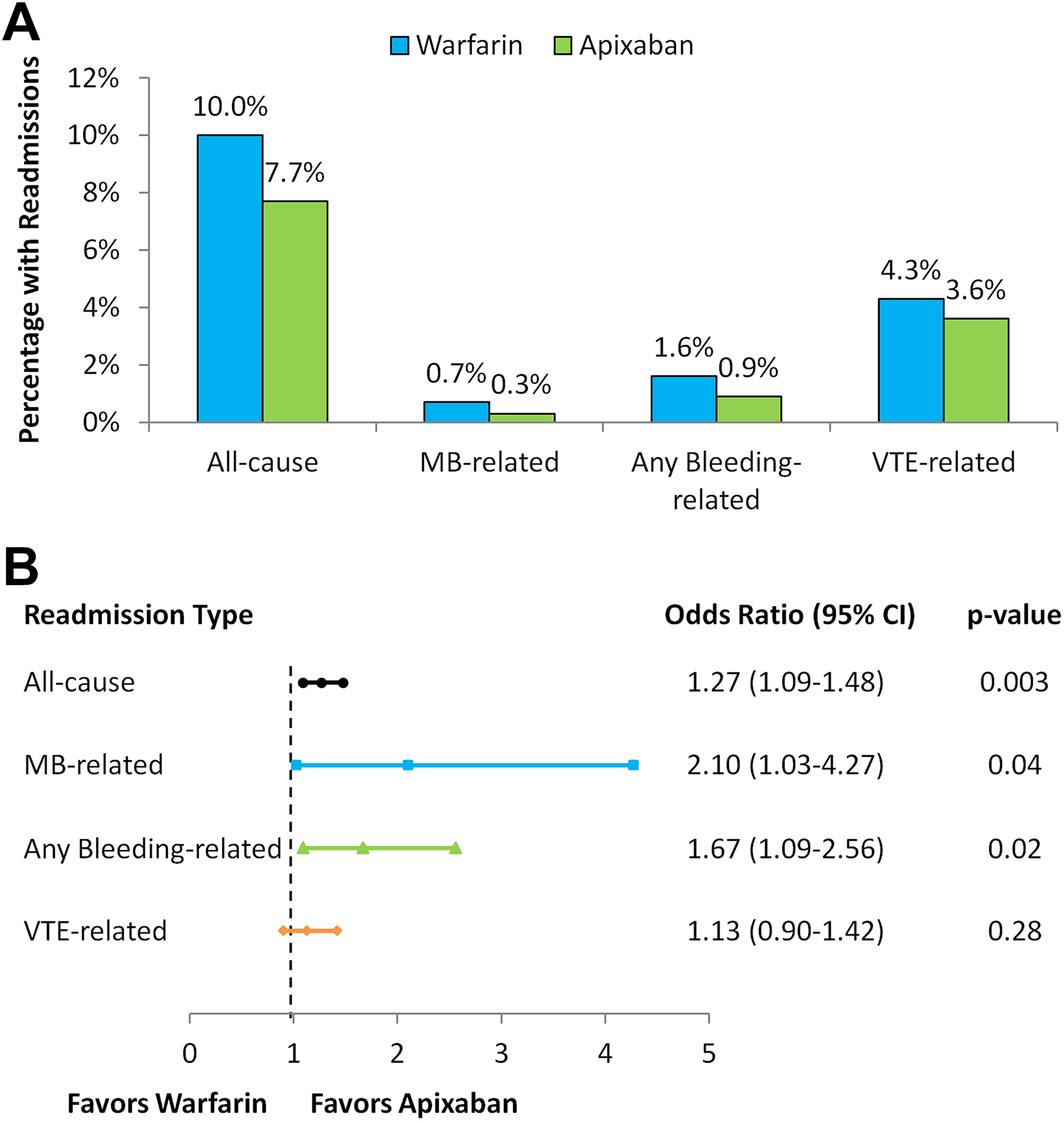
Unadjusted readmission rates (A) and adjusted risk for readmissions (B) for warfarin and apixaban cohorts.
After adjusting for key patient and hospital characteristics via multivariable logistic regression analysis, compared to apixaban, warfarin treatment was associated with a greater risk of all-cause readmission (odds ratio [OR]: 1.27; 95% CI: 1.09-1.48, P = .003), MB-related readmission (OR: 2.10; 95% CI: 1.03-4.27, P = .04), and any bleeding-related readmission (OR: 1.67; 95% CI: 1.09-2.56, P = .02; Figure 2B). The risk for VTE-related readmission did not differ significantly between study cohorts (OR: 1.13; 95% CI: 0.90-1.42, P = .28; Figure 2B).
Hospital Readmission LOS and Associated Costs
Unadjusted hospital readmission LOS and costs are shown in Table 3. Two-part model regression analyses showed that, per patient, warfarin treatment was associated with a longer average hospital readmission LOS (0.12 days; 95% CI: 0.05-0.20, P = .001) and higher mean hospitalization cost (US$173; 95% CI: US$40-US$320, P = .02) versus apixaban for all-cause readmissions; a longer average hospital readmission LOS (0.03 days; 95% CI: 0.002-0.05, P = .03) and higher mean hospitalization cost (US$49; 95% CI: US$10-US$118, P < .001) for MB-related readmissions; and a longer average hospital readmission LOS (0.08 days; 95% CI: 0.02-0.14, P = .006) and higher mean hospitalization cost (US$75; 95% CI: US$26-US$147, P < .001) for any bleeding-related readmissions (Table 3). The average hospital readmission LOS and mean hospitalization cost for VTE-related readmissions did not significantly differ between study cohorts (Table 3).
Hospital Length of Stays and Associated Costs per Patient for Readmissions.a
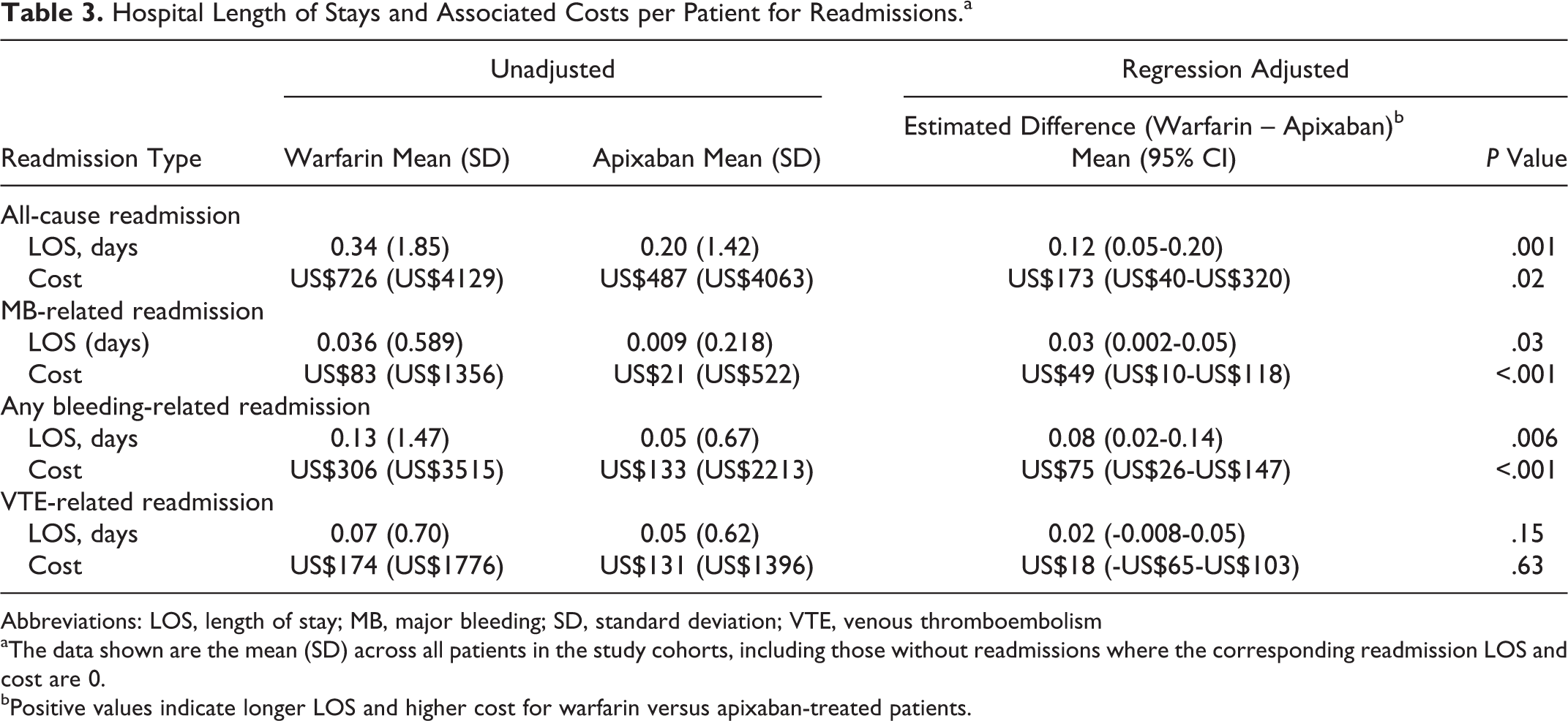
Abbreviations: LOS, length of stay; MB, major bleeding; SD, standard deviation; VTE, venous thromboembolism
aThe data shown are the mean (SD) across all patients in the study cohorts, including those without readmissions where the corresponding readmission LOS and cost are 0.
bPositive values indicate longer LOS and higher cost for warfarin versus apixaban-treated patients.
Sensitivity Analysis
We found among the study population that 98% (N = 25 619) of patients treated with warfarin during their index hospitalization received parenteral anticoagulation therapy (bridging therapy). The outcomes of this bridging warfarin cohort were also compared to the apixaban cohort (N = 2524). In this sensitivity analysis, per patient, the regression adjusted average LOS was longer (3.8 vs 3.1 days, P < .001; difference: 0.7 days) and mean hospitalization cost was higher (US$3236 vs US$2753, P < .001; difference: US$483) for index VTE hospitalizations of patients treated with warfarin versus apixaban. These results are similar to the findings in the primary analysis.
Regarding readmission risk, the findings from the sensitivity analysis were also consistent with the primary analysis results, with the regression analyses showing the risks of all-cause (OR: 1.27; 95% CI: 1.08-1.48, P = .003), MB-related (OR: 2.09; 95% CI: 1.02-4.26, P = .04), and any bleeding-related (OR: 1.66; 95% CI: 1.09-2.54, P = .02) readmission being greater for warfarin versus apixaban-treated patients. The risk for VTE-related readmission did not differ significantly between cohorts (OR: 1.12; 95% CI: 0.90-1.41, P = .30). The associated hospital readmission LOS and costs of readmissions for this sensitivity analysis of only including warfarin bridging patients in the warfarin cohort are shown in Supplemental Table 1.
Discussion
This study analyzed a population of more than 28 000 patients hospitalized for acute VTE in the United States between August 1, 2014, and May 31, 2016. After controlling for many differences in patient and hospital characteristics, patients who received warfarin were estimated to have an average hospital stay that was 0.7 days longer and a hospitalization cost that was on average US$484 higher for index hospitalizations compared to patients who received apixaban. Additionally, we found that warfarin treatment for VTE, compared to apixaban treatment, was associated with approximately a 27% greater risk of having a hospital readmission for any cause, twice the risk of having a MB-related readmission and a 67% greater risk for having any bleeding-related readmission during 1 month after the index VTE hospitalization. Furthermore, for patients treated with warfarin, the average LOS was longer and hospitalization cost higher for all-cause, MB-related, and any bleeding-related readmissions compared to patients treated with apixaban. The findings of the primary analysis were generally consistent with the sensitivity analysis, in which patients were only included in the warfarin cohort if they received warfarin bridging therapy during index hospitalization.
The longer hospital LOS and higher cost for index VTE hospitalizations associated with warfarin when compared to apixaban treatment may be attributed, in part, to the length in time required to obtain the optimal therapeutic range for warfarin—especially, when bridged from a parenteral anticoagulant—which can require days, and related bleeding complications, especially in those at higher risk of bleeding. 16 With apixaban, there is no need for monitoring or complicated dosage adjustments. 16 Also, apixaban begins to act immediately after treatment initiation, which could potentially allow for a shorter period of acute care. 16
In regard to the higher risk of MB- and any bleeding-related readmissions associated with warfarin versus apixaban treatment observed in this real-world study among patients hospitalized for VTE, the results support the findings of the AMPLIFY trial. In the AMPLIFY clinical trial, apixaban compared to enoxaparin/warfarin treatment was found to be associated with nearly a 70% reduction in the risk of MB and a 56% reduction in the risk for the combined outcome of MB and clinically relevant non-MB. 7 Additionally, our results supplement the secondary analysis of the AMPLIFY trial, which found that compared to enoxaparin/warfarin-treated patients, those treated with apixaban had an approximately 30% lower risk for all-cause hospitalization within the first 30 days of their index VTE hospitalization and readmissions were an average of 0.4 days shorter. 8
This study provides the first evidence on the comparison of bleeding rates among patients with VTE treated with warfarin versus apixaban in the real-world setting. Although no other comparative real-world data are currently published for apixaban in patients with VTE, our results are consistent with the several real-world studies of patients with atrial fibrillation, which have repeatedly found warfarin treatment to be associated with a greater likelihood for bleeding than apixaban treatment. 17 –23 As the occurrence of MB events among patients with VTE in the real-world setting in the United States has been reported to be relatively high (14% of patients within 1 year of initial VTE diagnosis) and the associated medical cost remarkably high (US$45 367 annually in 2013 USD), 13 newer anticoagulants with a lower risk of bleeding, such as apixaban, may provide an alternative treatment choice for hospitalized patients with VTE.
In the secondary analysis of the AMPLIFY trial, compared to patients treated with apixaban, a greater number of patients treated with enoxaparin/warfarin were readmitted to the hospital for recurrent VTE (37 vs 48 over 6 months). 8 In our study, we also found a higher percentage of patients in the warfarin cohort (4.3%) were readmitted to the hospital for recurrent VTE within 1-month postdischarge than in the apixaban cohort (3.6%). However, this difference was not statistically significant. These results may be related, in part, to the fact that patients were only followed for 1-month postdischarge, and further study with a longer follow-up period may be needed. Furthermore, the sample size of the apixaban-treated cohort was relatively low, since this study is among the earliest to evaluate real-world VTE treatment with apixaban.
Strengths and Limitations
In this first real-world analysis of patients hospitalized for acute VTE who were treated with warfarin versus apixaban, we used the Premier Hospital database—the largest hospital database in the United States—to examine differences in hospitalization LOS, costs, and readmission rates, including bleeding-related readmissions between study cohorts. There are several limitations of this study. First, the database does not contain information on outpatient health-care utilization; therefore, patients with DVT who were treated in the outpatient setting were not captured in the study population. Future studies with larger apixaban-treated populations and potentially longer follow-up periods may be helpful to further compare the VTE rate differences in patients treated with warfarin and apixaban in real-world settings. Second, while the Premier Hospital database contains information from a large number of hospitals across the United States, it is possible that it may not be representative of the entire US population of hospitalized patients with VTE. Third, only readmissions to the same hospital or hospital system within the Premier network can be identified in the database. This limitation may have led to an underestimate of actual readmission rates. Fourth, administrative hospital records data are collected for purposes other than research and may contain coding errors and missing data. Fifth, as this is an observational study, patients were not randomized, and despite statistical adjustments, unobserved confounders may still potentially exist for which the analysis did not control. Finally, no causal relationship between treatments and outcomes could be established based on this retrospective hospital records analysis.
Conclusions
This study of patients hospitalized for acute VTE in a real-world setting in the United States suggests that treatment with apixaban was associated with shorter hospital stays and less costly index hospitalizations for acute VTE versus warfarin. Apixaban treatment was also associated with a reduced risk for all-cause, MB-related, and any bleeding-related readmissions within 1 month after discharge from index VTE hospitalization, as well as shorter hospital stays and lower costs for corresponding readmissions compared to warfarin. These results supplement findings from the AMPLIFY trial and its secondary analyses of trial participants, by providing information on healthcare resources and corresponding costs associated with apixaban compared to warfarin in the real-world hospital setting.
Supplemental Material
Supplemental Material, VTE_Warf_Apix_Index_Hosp_Readmission_Manuscript_v12_Submitted_Suppl_Table - Hospital Resource Utilization and Costs Associated With Warfarin Versus Apixaban Treatment Among Patients Hospitalized for Venous Thromboembolism in the United States
Supplemental Material, VTE_Warf_Apix_Index_Hosp_Readmission_Manuscript_v12_Submitted_Suppl_Table for Hospital Resource Utilization and Costs Associated With Warfarin Versus Apixaban Treatment Among Patients Hospitalized for Venous Thromboembolism in the United States by Steven Deitelzweig, Jennifer D. Guo, Patrick Hlavacek, Jay Lin, Gail Wygant, Lisa Rosenblatt, Anu Gupta, Xianying Pan, Jack Mardekian, Melissa Lingohr-Smith, Brandy Menges, Alexander Marshall, and Anagha Nadkarni in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Steven Deitelzweig is a consultant for Bristol-Myers Squibb and Pfizer. Jennifer D Guo, Gail Wygant, Lisa Rosenblatt, Xianying Pan, and Anagha Nadkarni are employees of Bristol-Myers Squibb and own stock in the company. Alexander Marshall is a fellow with Rutgers University and Bristol-Myers Squibb. Patrick Hlavacek, Anu Gupta, and Jack Mardekian are employees of Pfizer. Jay Lin, Melissa Lingohr-Smith, and Brandy Menges are employees of Novosys Health, which has received research funds from Bristol-Myers Squibb and Pfizer in connection with conducting this study and development of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Bristol-Myers Squibb and Pfizer.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.