
Abstract
Total hip replacement (THR) and total knee arthroplasty (TKA) carry a high risk of postoperative venous thromboembolism (VTE); therefore, anticoagulation prophylaxis is recommended in these patients. Unfortunately, there are no guidelines about VTE prophylaxis in patients with hemophilia who underwent these high-risk surgeries. To determine whether these patients have high risk of VTE, we conducted a retrospective study on patients with hemophilia who underwent elective THR/TKA at our institute from 2004 to 2012. Postoperatively, we collected information on duration and method of factor VIII/IX infusion, VTE-prophylaxis, and complications. There were 23 patients with hemophilia, 18 (78%) with hemophilia A and 5 (22%) with hemophilia B, who underwent high-risk surgeries (39% THR and 61% TKA). The VTE prophylaxis included sequential compression device, 12 (52%), and prophylactic enoxaparin, 1 (4%). Ten (43%) patients did not receive VTE prophylaxis. At 1-year follow-up, we did not find any evidence of clinical VTE in our patients. Better risk stratification is needed to identify patients who would benefit from pharmacological prophylaxis.
Keywords
Introduction
The total hip replacement (THR) and total knee arthroplasty (TKA) carry with it a 45% to 84% risk of postoperative venous thromboembolic disease. 1 –6 About 2% to 7% of these patients may also develop pulmonary embolism, and 0.5% die from pulmonary embolism. 1 –6 The American College of Chest Physicians has strongly recommended anticoagulation prophylaxis with either low-molecular-weight heparin (LMWH), vitamin K antagonist with a target international normalized ratio of approximately 2 to 3, or fondaparinux in these patients. 7
Hemophilia, which is a group of inherited X-linked bleeding disorder, is secondary to a deficiency of factor VIII (FVIII; hemophilia A) or factor IX (FIX; hemophilia B). Severity of the disease presentation correlates with factor assay levels, with more disease manifestations in severe disease (defined as <1% factor activity). Internal bleeding can occur anywhere in patients with hemophilia, with joints being the most commonly involved site (80%), leading to severe pain, disfigurement, immobility, destruction, and development of debilitating arthritis. 8 Therefore, elective joint arthroplasty has emerged as a recent therapeutic option for management of hemophilic arthropathy with beneficial outcomes, such as restoring mobility and function, reducing joint pain, and reducing the frequency of recurrent joint bleeds. 8,9
Unfortunately, there are scarce data on the incidence of venous thromboembolism (VTE) in patients with hemophilia; therefore, the role of anticoagulation prophylaxis is being debated after high-risk surgeries in these patients. Orthopedic surgeons tend to avoid thromboprophylaxis on the assumption that the coagulation defect confers protection from VTE. Krause et al 10 have reported on the incidence of deep vein thrombosis (DVT) in hemophilia A after THR and TKA and found no documented cases of DVT in 32 patients with hemophilia A. In this study, patients did not receive any postoperative prophylaxis. 10 Other studies have also shown minimal occurrence of postoperative VTE with either no or mechanical thromboprophylaxis. 11 –18
Due to recent medical advances and more frequent use of recombinant factors, patients with hemophilia undergoing THR or TKA live longer with fewer complications. 2 –8 The number of hemophilic arthropathy has also been increasing for the last 10 years. 2 –8 In this study, we have reported our institution’s experience with patients having hemophilia who have undergone these high-risk surgeries and specifically evaluated whether these surgeries are associated with increased risk of thromboembolism in this population.
Methods
Institutional review board approval was obtained for a retrospective study that was conducted on consecutive patients with hemophilia from 2004 to 2012 who underwent elective TKA or THR for hemophilic arthropathy at our hemophilia treatment center, Ellis Fischel Cancer Center, University Hospital Missouri, Columbia. Orthopedic surgery was performed under general anesthetic by a senior surgeon. Standard antibiotic prophylaxis was given before surgery. Treatment protocol included initial bolus doses of FVIII or FIX at a dose of FVIII (international units) = weight (kg) × (desired percent increase) × 0.5 or FIX at a dose of weight (kg) × (desired percent increase) × F (F = 1.0 for coagulation FIX [Human]; F = 1.2 for coagulation FIX [recombinant]) in adults.
The preoperative target for FVIII or FIX levels was 100% factor assay activity. Continuous infusion (CI) dosing was calculated as follows: a bolus dose was delivered to bring the FVIII or FIX level to 100% assay activity (formula mentioned earlier), followed by CI at 4 IU kg/h. Factor assays were performed daily and the infusion rate for CI was adjusted to maintain the FVIII or FIX concentration at the desired level. All patients were negative for hemophilia inhibitor at the time of THR or TKA.
Our hospital system has a robust electronic health medical record system and a state-of-the-art orthopedic institute, which is specially designed for knee and hip replacement surgery. There is a policy in our institute that all patients with hamophilia A or B who need elective TKA and THR are first seen by hematologist in the clinic prior to surgery. All of these patients had a comprehensive history and physical examination, inhibitor screen, viral hepatitis profile, and HIV status checked. Patients were then admitted to the hospital for elective THR and TKA. All of these patients were retrospectively identified by International Classification of Diseases, ninth revision codes for hemophilia A, hemophilia B, TKA, and THR. Similar methodology and electronic record were used for patients seen by a hematologist first in the clinic. Fortunately, per institutional protocol, all patients were seen preoperatively by a designated hematologist; therefore, we were able to verify all patients with hemophilia who received these surgeries at our center.
We retrospectively collected information on demographics, body mass index (BMI), previous history of VTE, presence of inhibitor, HIV status (Western blot and viral load), hepatitis B status (hepatitis B surface antigen and hepatitis B core antibody), and hepatitis C status (enzyme linked immunosorbent assay [ELISA]), and if positive then confirmed by reverse transcriptase polymerase chain reaction to detect hepatitis C virus RNA. We also collected information on history of malignancy and family history of thrombophilia, which included antiphospholipid syndrome. Postoperatively, we extracted information on thromboprophylaxis received during hospitalization, duration of maintenance of factor infusion, and occurrence of clinically symptomatic VTE, bleeding, and other postoperative complications. This was done through a systematic retrospective chart review of the study patients looking 12 months out postoperatively for objectively documented evidence of VTE. No screening ultrasounds were done routinely to diagnose asymptomatic venous thrombosis postoperatively.
After THR or TKA, all patients underwent a standard rehabilitation program per institutional protocol, mobilizing the knee using a continuous passive motion machine and encouraging early full weight bearing as tolerated.
Results
There were 23 patients with hemophilia who underwent THR or TKA from 2004 to 2012. In all, 18 (78%) patients had hemophilia A and 5 (22%) patients had hemophilia B. Severe hemophilia defined as <1% factor activity was noted in 94% of patients with hemophilia A and 80% of patients with hemophilia B. Of the patients, 61% underwent TKA and 39% underwent THR.
All patients were noted to be negative for previous history of VTE and inhibitor screening. There were 2 (9%) patients with hemophilia A who had an underlying malignancy prior to surgery. One patient had rectal adenocarcinoma and the other patient had lung adenocarcinoma; however, both cancers were in complete remission prior to surgery. There were 14 (61%) patients with hepatitis C, 4 (17%) with hepatitis B, and 5 (22%) with HIV before surgery. Family history of thrombophilia was present in 2 (8%) patients. The median BMI was 24 (range 21-46). Two patients had BMI more than 35 (9%) and 1 of them had morbid obesity. Table 1 describes the preoperative characteristic features of the study patients with hemophilia A and B.
A Preoperative Characteristic Features of Patients With Hemophilia A and Hemophilia B.
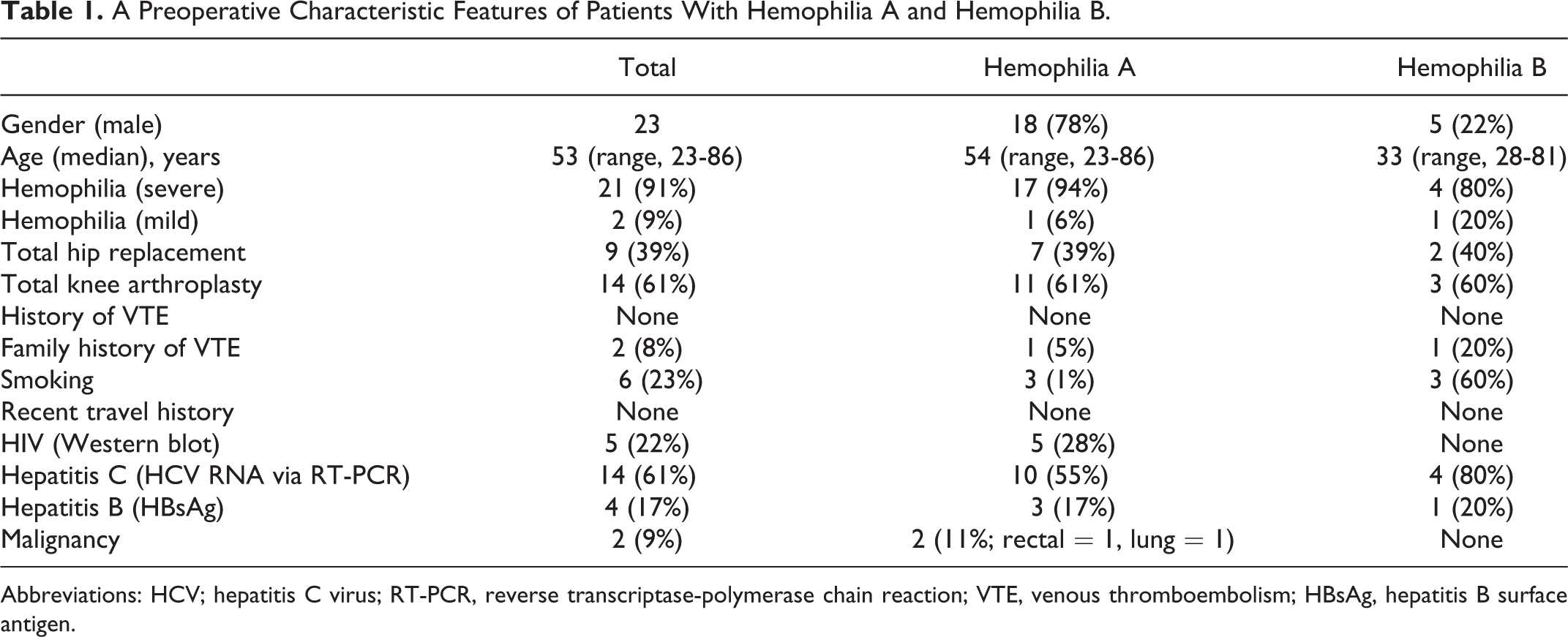
Abbreviations: HCV; hepatitis C virus; RT-PCR, reverse transcriptase-polymerase chain reaction; VTE, venous thromboembolism; HBsAg, hepatitis B surface antigen.
After THR or TKA, patients were treated with continuous factor infusion for at least 10 days (range 10-22). Median hospital stay for our study cohort was 14 days (range 10-27 days). The median peak FVIII and FIX levels were 153% (range 129%-244%) and 129% (range 77%-141%), respectively.
Of 23 patients, 12 (52%) patients had sequential compression device (SCD); 1 (4%) patient who had hemophilia A received LMWH (enoxaparin; 40mg subcutaneously daily); and 10 (43%) patients did not receive any VTE prophylaxis. One patient who had hemophilia B received prophylactic LMWH (enoxaparin) and had severe hemoptysis requiring intensive care monitoring due to rapid decline in FIX level up to 50%. The patient was switched to bolus infusion and after achieving target FIX level to 100% was again started on enoxaparin 40 mg subcutaneously for prophylaxis. The patient had a good outcome but required a hospital stay for 27 days. No other postoperative bleeding episodes were noticed in the other study patients. Four (17%) patients had postoperative pneumonia which was resolved with antibiotics. There was no evidence of symptomatic DVT or pulmonary embolism in any of the above-mentioned patients. Table 2 describes postoperative characteristics of patients with hemophilia in our study.
Postoperative Characteristics of Patients With Hemophilia.
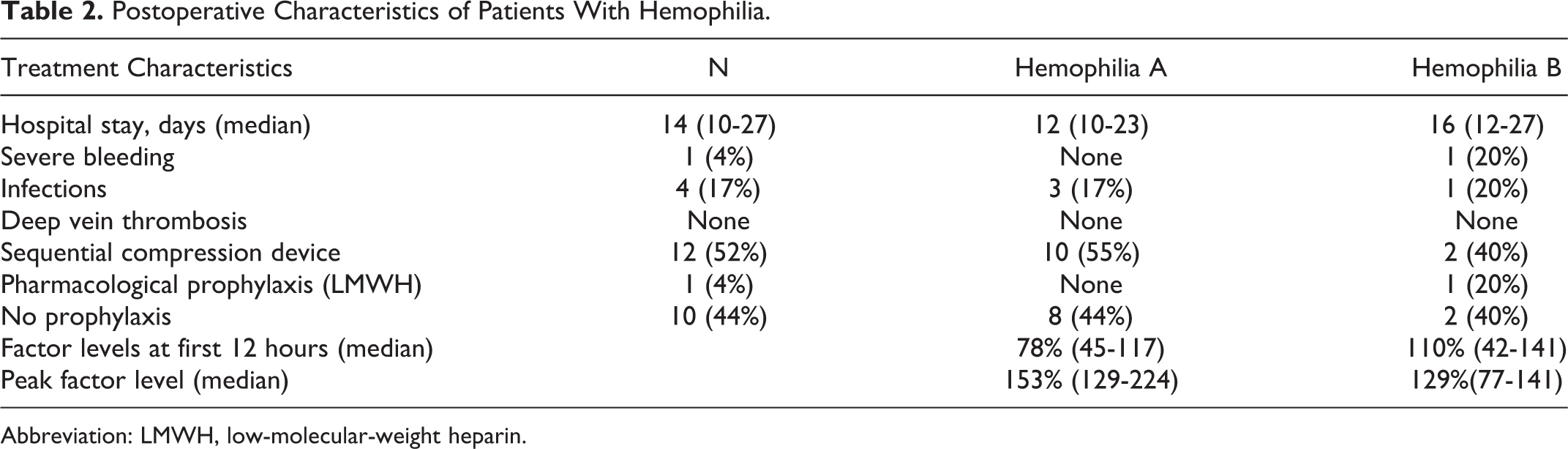
Abbreviation: LMWH, low-molecular-weight heparin.
Discussion
Patients with hemophilia are often considered to be at exceptionally low risk of postoperative thromboembolic complications. The low risk has been attributed to several factors including the young age and inherent protection offered by the bleeding disorder (variability between hemophilia A and B). In a normal individual, FVIII levels are known to increase nearly 2-fold postoperatively and stay elevated for several days or more, adding to an increased risk of DVT. 19 In patients with hemophilia A, however, the FVIII levels are only placed to 100% assay activity level and then drop as the factor replacement is cut down and discontinued. This may be one of the factors that tend to be protective against developing VTE. 19,20
A few studies have reported increased thrombotic risk associated with major joint replacement surgery due to decreased joint mobility, obesity, rapid correction of factor concentrates, elevated FVIII levels, and presence of congenital or acquired thrombophilia. 20,21 Patients with von Willebrand disease have been shown to have a much higher risk of VTE, especially after surgery. This is thought to be related to increased FVIII, due to replacement with factor concentrates containing FVIII in addition to von Willebrand factor and an increase in the half-life of endogenous FVIII. 22 Specifically, the co-occurrence of thrombophilic states such as factor V Leiden mutation, prothrombin gene mutation, protein C, and protein S deficiencies has been thought to reduce bleeding tendencies in patients with hemophilia. 23 This may suggest a potential increased risk of VTE as well. At this time, there are not large enough studies to support the recommendation for routine preoperative thrombophilia testing in patients with hemophilia prior to high-risk orthopedic surgery. 21 The presence of HIV infection has also been noted as an independent risk factor for VTE in patients with hemophilia. 24
There has been considerable disagreement about the optimal approach for thromboprophylaxis in these patients, given the complex considerations noted earlier. Thus far, it has been left up to the physician’s discretion to decide whether the patients with hemophilia will receive mechanical or pharmacological VTE prophylaxis or no prophylaxis. Pradhan and colleagues conducted a brief survey about the current attitudes in the practice of perioperative thromboprophylaxis in patients with hemophilia undergoing orthopedic surgery across 140 federally funded “Hemophilia Treatment Centers” in the United States. 20 According to the survey, 67% of physicians responded “yes” to anticoagulation prophylaxis in patients with hemophilia undergoing these high-risk surgeries; 25% of physicians did not agree with anticoagulation prophylaxis; and 78% of physicians who said yes to anticoagulant prophylaxis recommended prophylaxis if the factor level was above 100%. However, modality of prophylaxis also varied considerably. In all, 32% reported ordering compression stockings, 35% recommended SCDs, 24% reported using enoxaparin, 1% reported using fondaparinux, 3% reported using unfractionated heparin, 4% reported using warfarin, and 1% reported using aspirin. The survey results clearly demonstrate the wide variation in the practice of thromboprophylaxis in patients with hemophilia undergoing THR and TKA. In our study, 43% of patients did not receive any VTE prophylaxis due to the wide variety of practices without objective data. Therefore, there is a need for guidelines about VTE prophylaxis in the management of patients with hemophilia after these high-risk surgeries.
In the present study, we did not find any evidence of symptomatic VTE in the population with hemophilia after high-risk orthopedic surgeries. However, it is unknown which patients would benefit from only mechanical prophylaxis or pharmacological prophylaxis or both versus no prophylaxis. We believe patients who have multiple high-risk features should be evaluated individually for anticoagulant prophylaxis unless incidence of VTE in hemophilia is more clearly defined in randomized trials.
Mannucci et al 25 recommended LMWH 6 to 12 hours after orthopedic surgery, along with factor replacement in the absence of inhibitors or mechanical prophylaxis alone in the presence of inhibitors versus early ambulation. However, these recommendations are based on expert opinion, and due to lack of randomized trials, rarity of clinical VTE events, and difficulty of conducting clinical trials in patients with hemophilia undergoing these surgeries, a consultation from experienced hematologists within an hemophilia center regarding VTE prophylaxis is warranted in these patients. The data on the use of intravenous heparin in hemophilia are also very limited, as most patients in the past did not have these high-risk surgeries or cardiac interventions. Recently, isolated case reports have shown the safety of heparin use in patients who underwent cardiac catheterization or who received a therapeutic heparin dose in patients with VTE provided their factor levels are above 100%. 21,23
The use of global markers of hemostasis such as thrombin generation assays, endogenous thrombin potential, as well as the use of thromboelastography, could potentially serve as an overall risk marker for bleeding, risk of VTE as well as to fine-tune factor replacement. Further studies in this area to develop validated protocols could be quite useful.
Conclusion
Life expectancy of patients with hemophilia is now approaching that of the general population. More patients with hemophilia are undergoing hip and knee replacement surgeries; therefore, better risk stratification for pharmacological and/or mechanical prophylaxis is required for these high-risk surgeries. In the present study, we did not find any VTE events; however, our data have limited numbers and should be interpreted with caution. At the present time, there are no randomized prospective clinical trials on VTE prophylaxis in patients with hemophilia, and it is highly unlikely that these trials will ever be accomplished in this population. Therefore, our findings are important for clinicians for the management of VTE prophylaxis in patients with hemophilia. Overall incidence of VTE in patients with hemophilia undergoing high-risk orthopedic surgeries is noted to be quite low in the small observational studies. The reports of VTE through anecdotal case reports have been predominant in patients with multiple additional thrombotic risk factors. Appropriate factor replacement protocols and monitoring to optimize the balance between bleeding and thrombotic risk could be quite helpful as well. Until prevalence of VTE is known and there have been a few anecdotal case reports of VTE, anticoagulation prophylaxis should only be considered in patients with hemophilia with multiple high risk factors for thromboembolism.
Footnotes
Acknowledgments
We would like to thank Theresa Murphy for reviewing and editing the manuscript.
Authors’ Note
This study received a travel award and was presented on August 8, 2013, at 23rd Mayo Clinic Annual Hematology Oncology Review in Amelia Island, Florida.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.