
Abstract
We aimed to investigate the association between the neutrophil–lymphocyte ratio (NLR) and coronary artery ectasia (CAE). The study included 198 patients who had undergone coronary angiography for suspected coronary artery disease (CAD). The patients were divided into the following 4 groups: group 1, 44 patients with normal coronary arteries; group 2, 61 patients with CAD; group 3, 40 patients with isolated CAE; and group 4, 53 patients with CAE coexisting with CAD. Neutrophil–lymphocyte ratio was significantly lower in group 1 than the other groups and significantly higher in group 4. Patients in group 1 had significantly lower neutrophil counts and significantly higher lymphocyte counts than the patients in group 4. The isolated CAE and CAD groups were similar in terms of NLR, neutrophil count, and lymphocyte count. In addition, we found significant positive correlations between presence of ectasia, number of ectatic vessels, and NLR. Our findings provide additional evidence for the role of NLR in CAE.
Keywords
Introduction
Coronary artery ectasia (CAE), an aberration of the coronary anatomy, has been characterized as dilation of an arterial segment to a diameter at least 1.5 times that of the adjacent normal coronary artery (NCA). Coronary artery ectasia can be found in up to 5% of angiographic and in 0.22% to 1.4% of postmortem examinations. 1 –6 In majority of cases, the disease is found to coexist with coronary artery disease (CAD). As a consequence of the presence of immobile or turbulent blood flow in an aneurysmal segment, the repeated dissemination of microemboli to distal segments of the ectasia or a thrombotic occlusion of the dilated vessel (angina pectoris and myocardial infarction) has been seen in patients with CAE. 7 In patients with CAE, 10% to 20% of cases have been described in association with inflammatory or connective tissue diseases. 8 –12 Moreover, previous studies demonstrated that the neurohormonal process, inflammation, and cardiovascular risk factors are related to CAE. 13 The underlying mechanisms of ectasia formation are not yet entirely known; however, previous studies have demonstrated that CAE may be a form of atherosclerosis with more active inflammatory properties than normal vessels. 3 –6
The neutrophil–lymphocyte ratio (NLR), a marker of inflammation, is an independent predictor of cardiac mortality. 14 The NLR is a predictor of severe atherosclerosis that may be useful for cardiac risk stratification in patients with CAD. 15 Blood NLR reflects systemic inflammation well, as it is cost effective, easily available, and can be calculated quickly. 16 Although a lot of data have shown the association between inflammatory response and atherosclerosis, the role of inflammation in the etiopathogenesis of CAE is poor. 17 –19 The relationship between NLR and the presence of CAE with coexisting CAD has not been extensively studied. Thus, we sought to investigate the association between NLR and CAE.
Materials and Methods
Patient Selection
In this study, a total of 198 patients were consecutively selected among 2980 patients who underwent coronary angiography for suspected CAD in the catheterization laboratory of the Istanbul Mehmet Akif Ersoy Thoracic and Cardiovascular Surgery Training and Research Hospital between June 2011 and May 2012. The study groups were designed according to the presence of ectasia and proportion of coronary artery stenosis as follows: group 1, 44 patients with NCAs; group 2, 61 patients with newly diagnosed obstructive CAD without CAE; group 3, 40 patients with isolated CAE (ectasia without obstructive CAD); and group 4, 53 patients with CAE with coexisting obstructive CAD.
Age, gender, smoking, history of diabetes mellitus and hypertension, body mass index, localization of ectasia, and number of ectatic vessels were recorded. The exclusion criteria were history of acute coronary syndrome, heart failure, previous percutaneous coronary intervention, a history of coronary artery bypass grafting surgery, active infectious disease, inflammatory or immunological disease, hematological disorders, cirrhosis, peripheral arterial disease, chronic obstructive pulmonary disease, chronic kidney disease, malignancy, and current use of steroid or nonsteroid antiinflammatory drugs. This study was approved by the ethics committee and informed consent was obtained from each patient.
Biochemical Analysis
Venous blood samples were collected prior to coronary angiography after a fasting period of 12 hours. Glucose, creatinine level, and lipid profile were measured for all patients with a Cobas-C 501 biochemical analyzer (Roche Diagnostics, Mannheim, Germany) using Roche kits. Hematological indices were evaluated from complete blood count analysis performed using a Mindray device BC-5800 (Mindray Bio-Medical Electronics Co Ltd, Shenzhen, China) by the optical laser method. The NLR was calculated as the ratio of neutrophils to lymphocytes.
Coronary Angiography and Transthoracic Echocardiography
Coronary angiography was performed using the Judkins technique through femoral artery access. Coronary angiograms were analyzed by 2 experienced interventional cardiologists without knowledge of the laboratory measurements or clinical status of the participant. Presence of CAD (significant coronary artery stenosis of at least 1 coronary artery) was defined as the existence of any stenosis with 50% or greater narrowing of the diameter in coronary arteries. Coronary artery ectasia was defined as the segmental or diffuse dilation of the coronary arteries to >1.5-fold the diameter of the adjacent segments of the same artery or of different arteries, as following Falsetti and Carroll. 8 Normal coronary artery was defined as coronary arteries without ectasia or stenosis on the basis of coronary angiography. The classification of CAE defined by Markis et al was graded as follows: type 1, diffuse ectasia of ≥2 coronary arteries; type 2, diffuse ectasia in 1 coronary artery and localized ectasia in another coronary artery; type 3, diffuse ectasia of 1 coronary artery; and type 4, localized or segmental (focal) ectasia of only 1 coronary artery. 2 According to Markis et al’s classification, types 1, 2, and 3 are classified as diffuse ectasia whereas type 4 is classified as focal ectasia.
Transthoracic echocardiography was performed on patients before discharge using a system V (Ving-med, GE, Horten, Norway) with a 2.5-MHz phased-array transducer. Recordings were taken from patients positioned in the left lateral decubitus position. The left ventricular ejection fraction (LVEF) was measured using the modified Simpson rule. 20
Statistical Analyses
All analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 18.0 for Windows (version 18.0, SPSS, Chicago, Illinois). The variables were investigated using visual (histograms and probability plots) and analytical methods (Kolmogorov-Smirnov test) to determine whether or not they were normally distributed. Descriptive analyses were presented as mean ± standard deviation and categorical variables were expressed as percentages. Groups were compared using the Mann-Whitney U, Kruskal-Wallis, 1-way analysis of variance, and the chi-square test. The Mann-Whitney U or Tukey test was performed to test the significance of pairwise differences using Bonferroni correction to adjust for multiple comparisons. Spearman correlation was used to evaluate the association between NLR and other variables. A 2-tailed P value <.05 was considered statistically significant.
Results
The study group consisted of 198 consecutive patients (132 [66.6%] men and 66 [33.3%] women) with an average age of 57 ± 10 years. The baseline characteristics of patients are summarized in Table 1. The prevalence of cardiovascular risk factors such as age, gender, hypertension or diabetes mellitus, smoking, metabolic syndrome, and a family history of CAD did not differ among the groups (for all, P > .05). In addition, the groups were similar in terms of hemoglobin, hematocrit, platelet count, monocytes, glucose, total cholesterol, triglycerides, and low-density lipoprotein cholesterol level. High-density lipoprotein cholesterol was significantly lower in patients with CAD (41 ± 9) and CAE with CAD (40 ± 10) than in patients with NCA (48 ± 10; P = .003 and P < .001, respectively).
Baseline Clinical and Laboratory Parameters in the Study Groups.a
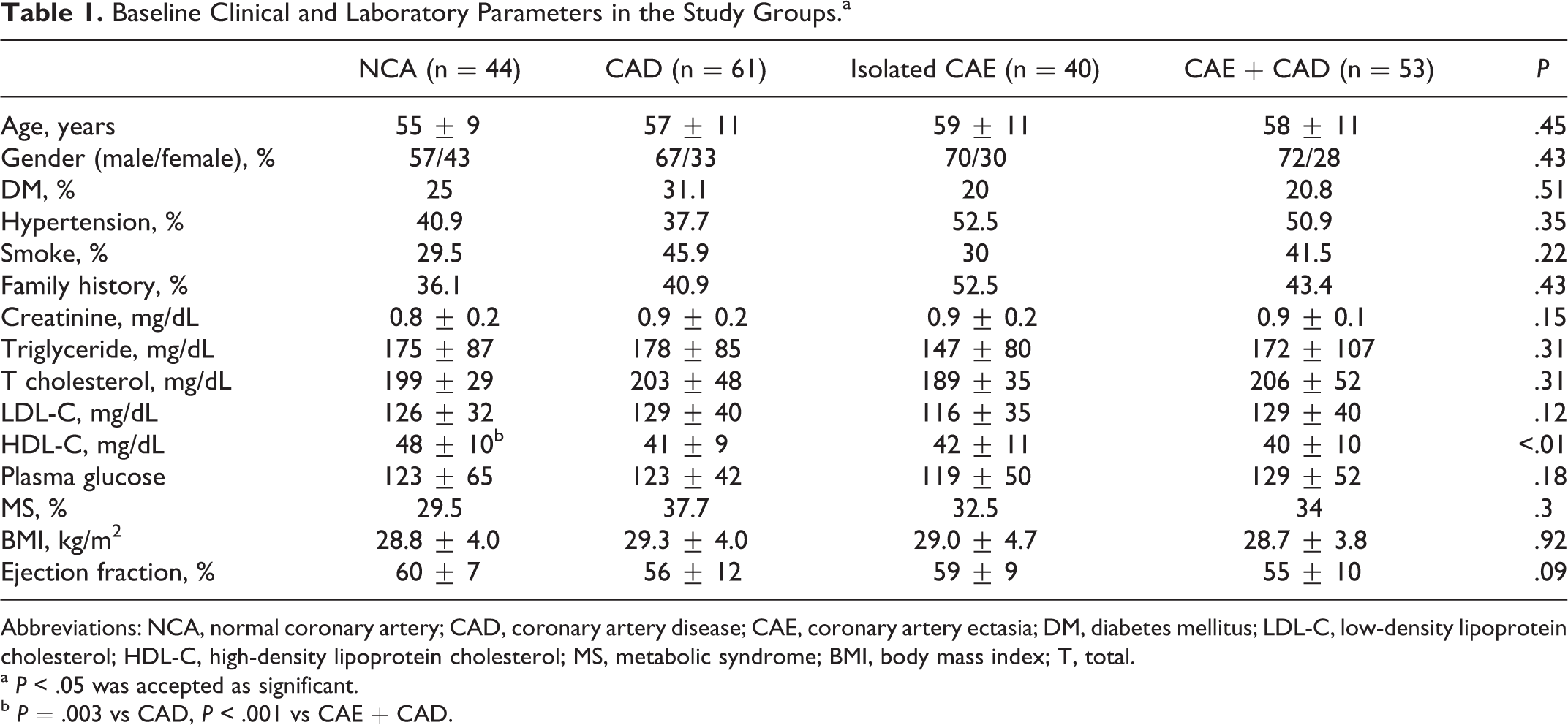
Abbreviations: NCA, normal coronary artery; CAD, coronary artery disease; CAE, coronary artery ectasia; DM, diabetes mellitus; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; MS, metabolic syndrome; BMI, body mass index; T, total.
a P < .05 was accepted as significant.
b P = .003 vs CAD, P < .001 vs CAE + CAD.
For patients with ectasia (group 3 and group 4), the number of ectatic vessels and classification of ectasia according to Markis et al are presented in Table 2. The most affected coronary artery was the right coronary artery (n = 59, 63.4%) and the distributions of coronary arteries affected by ectasia were found to be left main (n = 10, 10.8%), left anterior descending (n = 55, 59.1%), and circumflex (n = 54, 58.1%). Although the mean LVEF of the patients in the groups 2 and 3 was lower than those in groups 1 and 4, the difference was not statistically significant (P = .09; Table 1).
Distribution and Classification of Ectatic Vessels.
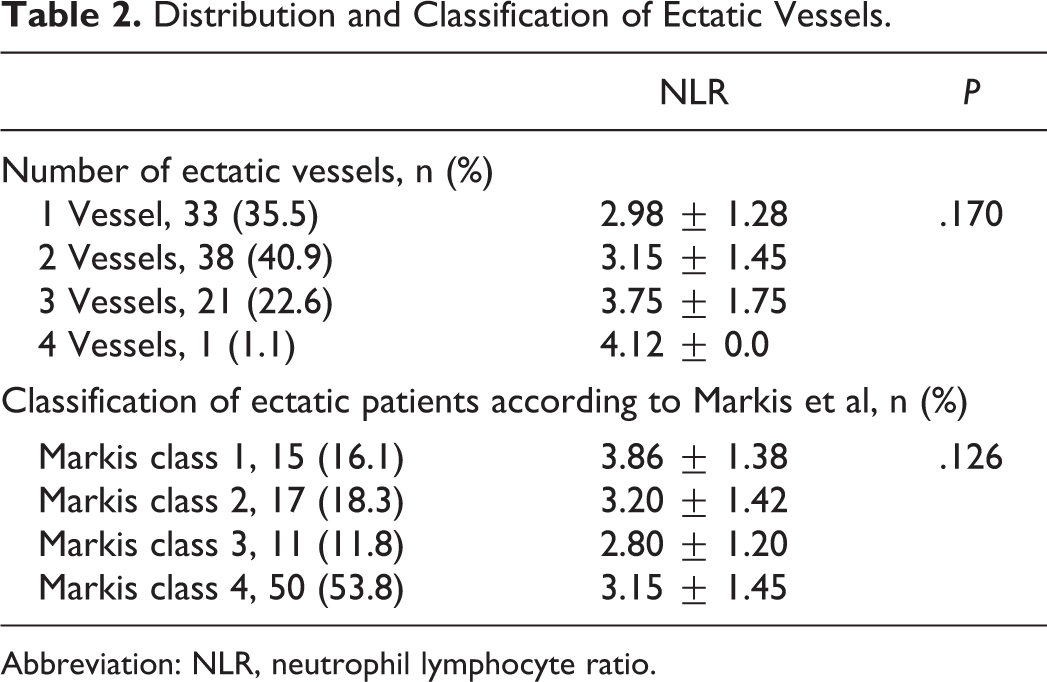
Abbreviation: NLR, neutrophil lymphocyte ratio.
The groups were compared with each other in terms of neutrophil count, lymphocyte count, NLR, and the other hematologic parameters (Table 3). In group 1 (NCA), the neutrophil count was found to be lower than in group 4 (CAE with CAD; P = .014), and the lymphocyte count was found to be significantly higher than in group 4 (CAE with CAD; P < .001). Moreover, NLR was significantly lower in group 1 (NCA) than in the other groups. Neutrophil–lymphocyte ratio was significantly higher in group 4 (CAE with CAD) than in the other groups. The NLR values of group 1 (NCA) and group 3 (isolated CAE) were 2.15 ± 1.27 and 2.92±1.56, respectively (P < .001). The NLR values of group 4 (CAE with CAD) and group 2 (CAD) were 3.46 ± 1.26 and 2.95 ± 1.56, respectively (P = .008). When group 2 (CAD) and group 3 (isolated CAE) were compared, the NLR did not differ between the groups (2.95 ± 1.56 vs 2.92 ± 1.56, P = .862; Table 3).
Comparison of the Hematological Parameters Among the Study Groups.a
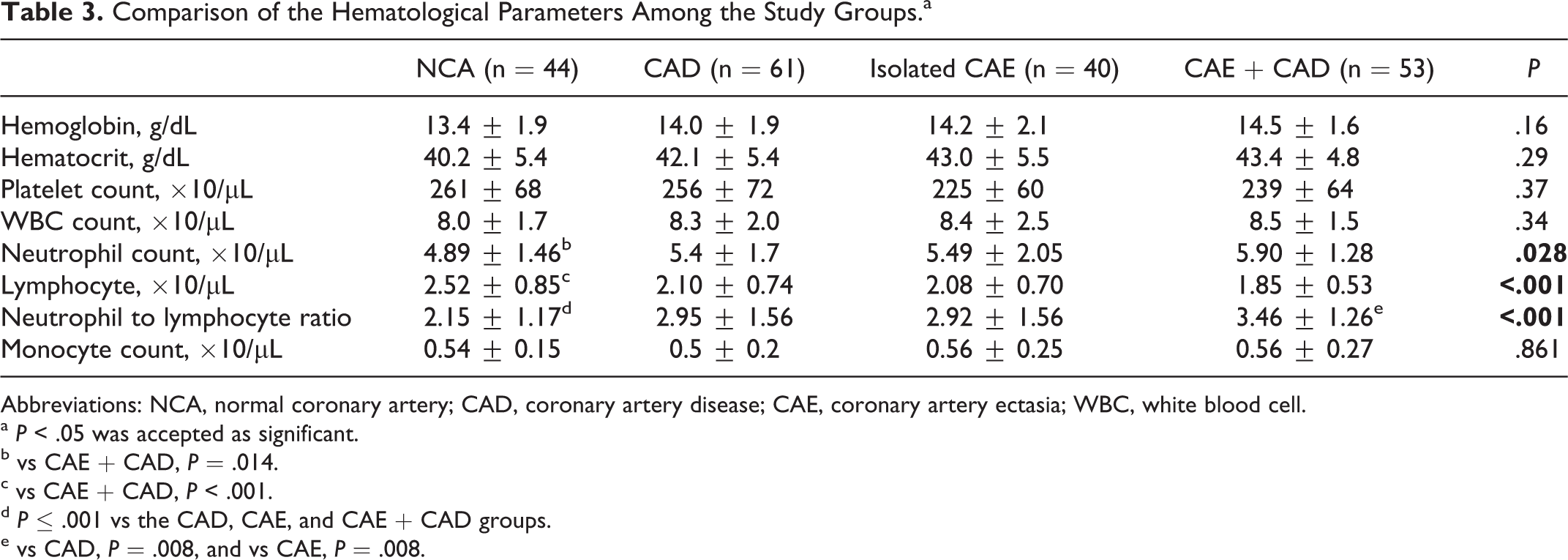
Abbreviations: NCA, normal coronary artery; CAD, coronary artery disease; CAE, coronary artery ectasia; WBC, white blood cell.
a P < .05 was accepted as significant.
b vs CAE + CAD, P = .014.
c vs CAE + CAD, P < .001.
d P ≤ .001 vs the CAD, CAE, and CAE + CAD groups.
e vs CAD, P = .008, and vs CAE, P = .008.
After evaluating our study population, the mean NLR value of patients with ectasia (n = 93), including group 3 and group 4, was significantly higher than the mean NLR value of nonectatic patients (n = 105), including group 1 and group 2 (3.23 ± 1.42 vs 2.62 ± 1.49, respectively, P < .001). We found a significant positive correlation between NLR and presence of ectasia (P < .001, r = .289). After evaluating 93 patients with ectasia (group 3 and group 4), we found a weak positive correlation between NLR and the number of ectatic vessels (P = .047, r = .207); however, there was no statistically significant difference between NLR values, as shown in Table 2. There was no significant correlation between NLR and any Markis classification (P = .170, r = −.143) or focal (Markis class 4) or diffuse (Markis class 1, 2, 3) ectasia (P = .498, r = −.071; Table 2). The NLR values of patients with focal and diffuse ectasia were 3.15 ± 1.45 and 3.33 ± 1.39, respectively (P = .495).
Discussion
In practice, CAE frequently coexists with severe atherosclerosis. Some recent publications have looked at the relationship between isolated CAE and NLR. 21,22 However, the relationship between NLR and CAE with coexisting CAD has not been extensively studied. Here, we showed that patients with isolated CAE had significantly higher NLR values than patients with NCA. We also demonstrated that patients having CAE with CAD had higher NLR values than patients with NCA, CAD, and isolated CAE. Additionally, we showed that neutrophil counts were higher in the CAE + CAD group than in the NCA group. Elevated neutrophil counts and NLR values in CAD and CAE may mirror severity of inflammation in coronary arteries. Thus, this study provided strong evidence for the role of inflammation in coronary ectasia.
Despite advances in cardiology, the specific causative mechanisms of abnormal luminal dilation in CAE remain unclear. However, some inflammatory markers such as C-reactive protein (CRP), interleukin 6, tumor necrosis factor α, matrix metalloproteinase, and some atherosclerotic risk factors such as advanced age, diabetes, and smoking may be associated with the presence of CAE. 3 –5 Coronary artery ectasia exists in 1.5% to 5% of patients included in coronary angiographic studies. 23 Angina pectoris can be seen in patients with CAE without CAD. In addition, some studies have shown that the frequency of acute coronary events via vasospasm, dissection, or thrombus is higher in patients with isolated CAE than in patients with normal coronary angiograms. Moreover, studies have reported that 29% to 39% of patients with isolated ectasia have a history of previous myocardial infarction or angina pectoris, and patients with CAE have an increased risk of mortality equivalent to patients with CAD. 2,24
Previous epidemiological and clinical studies have shown a clear association between peripheral leukocyte counts and the risk of adverse cardiovascular events in both patients with established CAD and individuals free of disease at baseline. 25,26 Thus, the role of inflammation in the initiation and progression of coronary atherosclerosis is well described. 27,28 The NLR ratio, a marker of inflammation, was an independent predictor of cardiac mortality. 14 Neutrophil–lymphocyte ratio is a predictor of severe atherosclerosis that may be useful for cardiac risk stratification in patients with CAD. 15
In this study, NLR was significantly lower in patients with NCA as well as significantly higher in patients with CAE coexisting with CAD. On the other hand, the isolated CAE and CAD groups were similar in terms of NLR. Having evaluated 93 patients with ectasia (group 3 and group 4), we found a weak positive correlation between NLR and number of ectatic vessels (P = .047, r = .207); however, the difference in NLR values between the groups did not achieve statistical significance. If we had a larger study group, the results might be different.
The histopathological characteristics of CAE are similar to those of coronary atherosclerosis. In more than half of the patients with CAE, the condition is related to coronary atherosclerosis. The histology of ectatic segments demonstrated extensive atherosclerotic changes and destruction of the media of the vessel wall. 6 This coexistence supports the idea that CAE may be a variant of CAD. Antoniadis et al reported that in the media layer of ectatic segments, there was an infiltration of inflammatory cells. 29
In this study, we observed that the lymphocyte level was decreased in isolated CAE and CAE with the CAD groups. The probable causes of this finding were decreased production of lymphocytes as a result of increased steroid level due to a CAE-induced stressed condition and increased apoptosis of lymphocytes triggered by increased inflammation. 30,31 In addition, several previous studies have reported decreased lymphocyte levels in acute cardiovascular events, and there is a negative correlation between cardiovascular prognosis and lymphocyte level. 32,25
Sarli et al showed that NLR was higher in patients with isolated CAE and in patients with CAD than in patients with NCA. In addition, it was demonstrated in the same study that NLR was associated with severity of coronary ectasia according to Markis classification. 21 Moreover, in 3 recent studies investigating the relationship between NLR and isolated CAE, it was shown that patients with isolated CAE had significantly elevated NLR levels. 22,33,34 Balta et al investigated the role of NLR in 181 patients that were divided into 3 groups; they found that NLR was significantly higher in both CAE and CAD groups compared to the NCA group. 34 Isık et al indicated that an NLR level ≥2.37 measured on admission had 77% sensitivity and 63% specificity in predicting isolated CAE. 33
In contrast to these studies, we evaluated patients with CAD with concomitant CAE and compared with CAD alone. We found that NLR was higher in patients having CAD with CAE than in patients with CAD alone as well as higher in patients with isolated CAE than in those with NCA. In our study, we also investigated the presence of associations between NLR and severity of ectasia (according to Markis classification), focal (Markis class 4), or diffuse (Markis class 1, 2, and 3) ectasia, distribution of ectatic coronary arteries, and number of ectatic coronary arteries. We found no association between NLR and either the Markis classification or having focal or diffuse ectasia. However, we did find significant positive correlations between NLR and both the presence of ectasia and number of ectatic vessels.
The role of inflammation in the development of coronary atherosclerosis is well known. This study showed that neutrophil counts and NLR were higher in patients with CAD, isolated CAE, and CAD with CAE compared to patients with NCAs. This may be related to chronic inflammation occurring in CAE.
Limitations
The first limitation in our study is the small sample size; further studies with larger sample sizes are needed to confirm that NLR may be used as an indicator for CAE. Second, we did not analyze other markers of inflammation such as inflammatory cytokines or high-sensitivity CRP. These measurements could provide important, comprehensive information.
Conclusions
Our findings provided additional evidence for the role of NLR in CAE. Neutrophil–lymphocyte ratio, which can be determined by a simple, easily available, and inexpensive complete blood count test, seems to be useful in predicting the presence of CAE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.