
Abstract
Purpose:
In this study, we aimed to investigate the relationship between saphenous vein graft disease (SVGD) and neutrophil-to-lympocyte ratio (NLR) with other possible confounding factors.
Methods:
A total of 120 patients were enrolled into the present study. Of all participants, 40 patients were with SVGD and 80 of them were with patent SVG.
Results:
The NLR, white blood cell (WBC) count, age of SVG, red cell distribution width (RDW), and mean platelet volume were significantly higher in the SVGD group. In regression analysis, NLR, WBC, RDW, and age of SVG remained as independent predictors of SVGD.
Conclusion:
To our knowledge, we showed for the first time that NLR is independently associated with SVGD. It can be easily used in this era, because it is easily available, widely used, and relatively cheap. Besides NLR, WBC count, SVG age, and RDW can also be used to predict SVGD.
Introduction
Ischemic heart disease is an important health problem with its morbidity and mortality. In this regard, coronary artery bypass grafting (CABG) is an available option to reduce the untoward consequences of coronary heart disease (CHD). Both arterial and venous conduits can be used in this procedure, but patency rates of saphenous vein grafts (SVGs) are lower compared to arterial conduits (especially for internal mammarian artery [IMA]). For the first year, there is significant stenosis in 15% of the SVGs, and at the 10th year of CABG surgery nearly half of the saphenous grafts will become occluded. 1 Most suggested mechanisms for SVG occlusion are thrombosis (first month), neointimal hyperplasia (1-12 month), and atherosclerosis (>12 months). 2
Role of inflammation in the atherosclerotic process has been well described previously. 3 White blood cells (WBCs) and its subtypes have been thought to be involved in this inflammatory disease. Neutrophils and lymphocytes are among the subtypes of WBCs, and the neutrophil-to-lymphocyte ratio (NLR) gives important clues about adverse outcomes. 4 Duffy et al showed that increased NLR predicts adverse outcomes in whom percutaneous coronary angioplasty was performed. 5 It has also been shown that elevated NLR is a marker of adverse prognosis in both stable angina and acute coronary syndromes. 6,7 In another study, it was shown that preoperative NLR was the strongest predictor of adverse outcomes in patients who underwent CABG. 8
In the light of these data, we aimed to investigate the relationship between NLR and other possible confounding factors with SVG disease (SVGD).
Methods
The study was performed at 2 education and research hospitals. Coronary angiography archives of these 2 centers were reviewed retrospectively between May 2011 and 2012, and patients with SVGs remained for further analysis. After evaluation for inclusion and exclusion criteria, 120 patients with SVG remained for final analysis. Afterward, we divided the patients into 2 groups according to the presence or absence of SVGD. Of all the participants, 40 patients were with SVGD and 80 of them were with patent SVG. The SVGD was accepted as presence of at least 50% stenosis in at least 1 SVG. Presence of at least 1 SVG for ≥1 year and a positive cardiovascular stress test and/or presence of stable angina as an indication for coronary angiography were accepted as inclusion criteria. Exclusion criteria were accepted as following: presence of acute coronary syndrome, significant valvular heart disease, decompensated heart failure, malignancy, renal or hepatic failure, acute or chronic infectious disease, autoimmune disease, anemia (definition of anemia according to the World Health Organization was a hemoglobin level of <12 g/dL in women or <13 g/dL in men), hematologic disease, and acute or chronic pulmonary disease.
Judkins technique was used for visualization of coronary arteries and coronary grafts. Each vessel was visualized in at least 2 different plane images. When it was indicated, visualization of aortic root was also performed by aortic root angiography. At least 2 cardiologist, who were blinded to patients’ characteristics, evaluated the coronary angiograms. Presence of ≥50% stenosis in at least 1 SVG was accepted as SVGD.
At both the centers, blood samples were collected after 12 hours of fasting between 8.00 and 10.00
Present study was approved by the local ethics committee.
Statistical Analysis
The SPSS 16.0 for Windows (SPSS Inc, Chicago, Illinois) was used for all statistical analysis. Continuous variables were given as mean ± standard deviation, and categorical variables were given as percentages. Kolmogorov-Smirnov test was used to test normality of distribution. Categorical variables were compared with chi-square test, and continuous variables were compared with Student t test or Mann-Whitney U test, as appropriate. Receiver–operating characteristic (ROC) curve analysis was used to determine the optimum cutoff level of NLR to predict the patency rate of SVG. Logistic regression analysis was used to define the odds ratios (ORs) and 95% confidence intervals (CIs) of possible confounding factors in SVGD. Variables with a P value of <.1 in univariate logistic regression analysis were tested in multivariate analysis. A P value of <.05 was accepted as statistically significant.
Results
The study group was composed of 120 patients. Of all participants, 80 patients were with patent SVG and 40 patients were with SVGD. Basal characteristics of the groups were presented in Table 1. Mean age was 66.0 ± 8.2 years in SVGD group and 66.8 ± 10.6 years in patients with patent SVG (P = .686). Most of the study participants were male. Mean SVG age was older in SVGD group than in the patent SVG group (8.3 ± 4.4, 6.1 ± 3.5 years, respectively, P = .004).
Basal Characteristics of Groups.
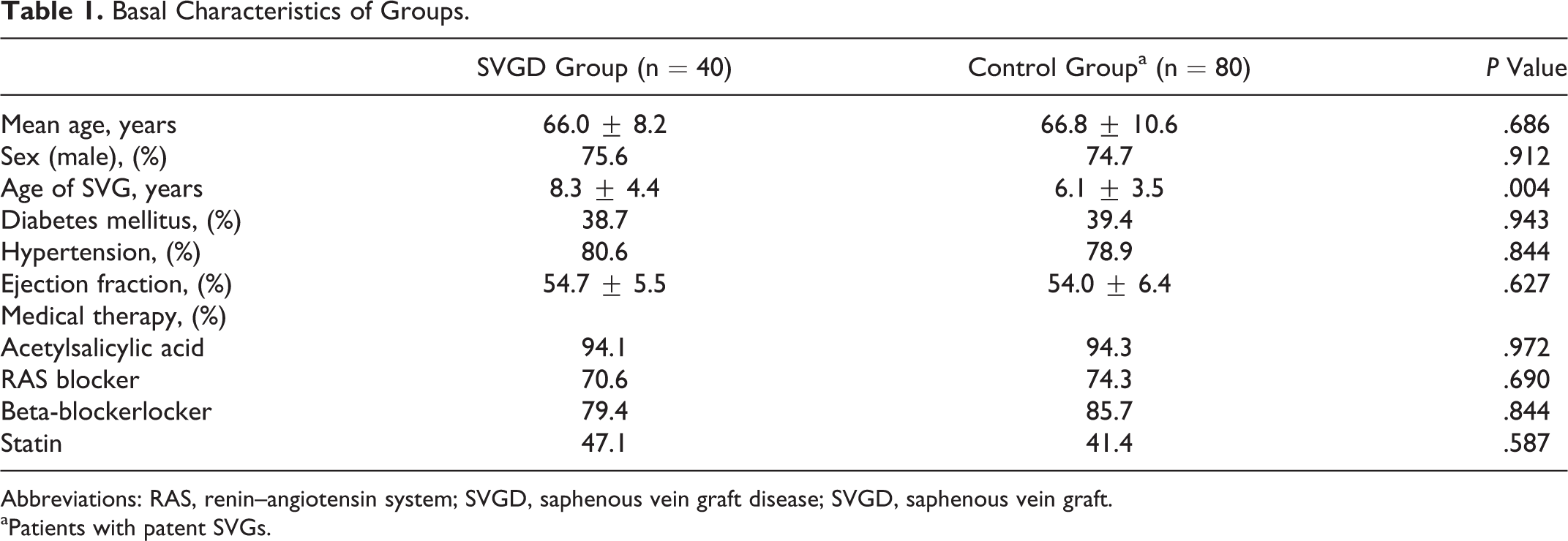
Abbreviations: RAS, renin–angiotensin system; SVGD, saphenous vein graft disease; SVGD, saphenous vein graft.
aPatients with patent SVGs.
Laboratory parameters of the patients were given in Table 2. The WBC count was significantly higher in the SVGD group (8.2 ± 1.3, 7.4 ± 1.6, P = .009). The NLR was higher in the SVGD group than the patent SVG (2.9 ± 1.4, 2.2 ± 0.8, P = .003; Figure 1). Another significant difference between the groups was red cell distribution width (RDW), and it was higher in the SVGD group (14.4 ± 1.5, 13.6 ± 1.1, P = .003). The mean platelet volume (MPV) values of patients with SVGD were higher than patients with patent SVG (8.7 ± 0.9, 8.3 ± 1.1, P = .039). Hemoglobin and creatinine levels, platelet count, and lipid parameters were similar between the 2 groups. Using a cutoff level of 2.5, NLR predicted patency for SVG with a sensitivity of 52% and specificity of 69% (ROC area under curve: 0.620, 95% CI: 0.509-0.731, P = .03; Figure 2).
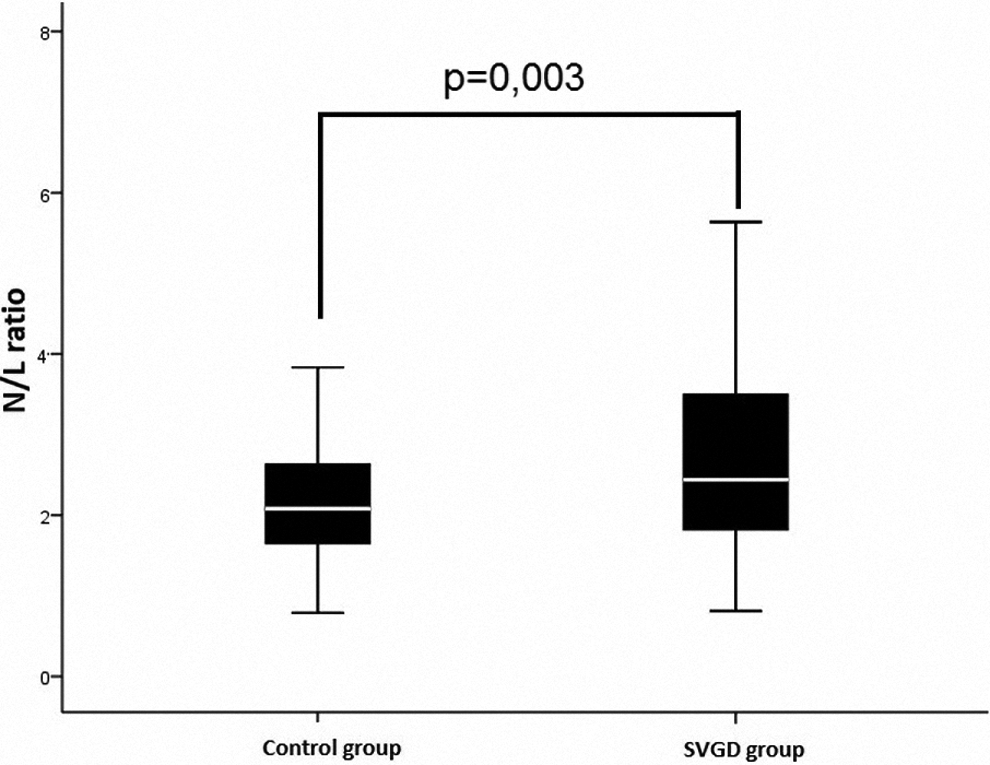
Comparison of neutrophil-to-lymphocyte ratios in saphenous vein graft disease and patent saphenous vein grafts. N/L indicates neutophil-to-lymphocyte ratio.
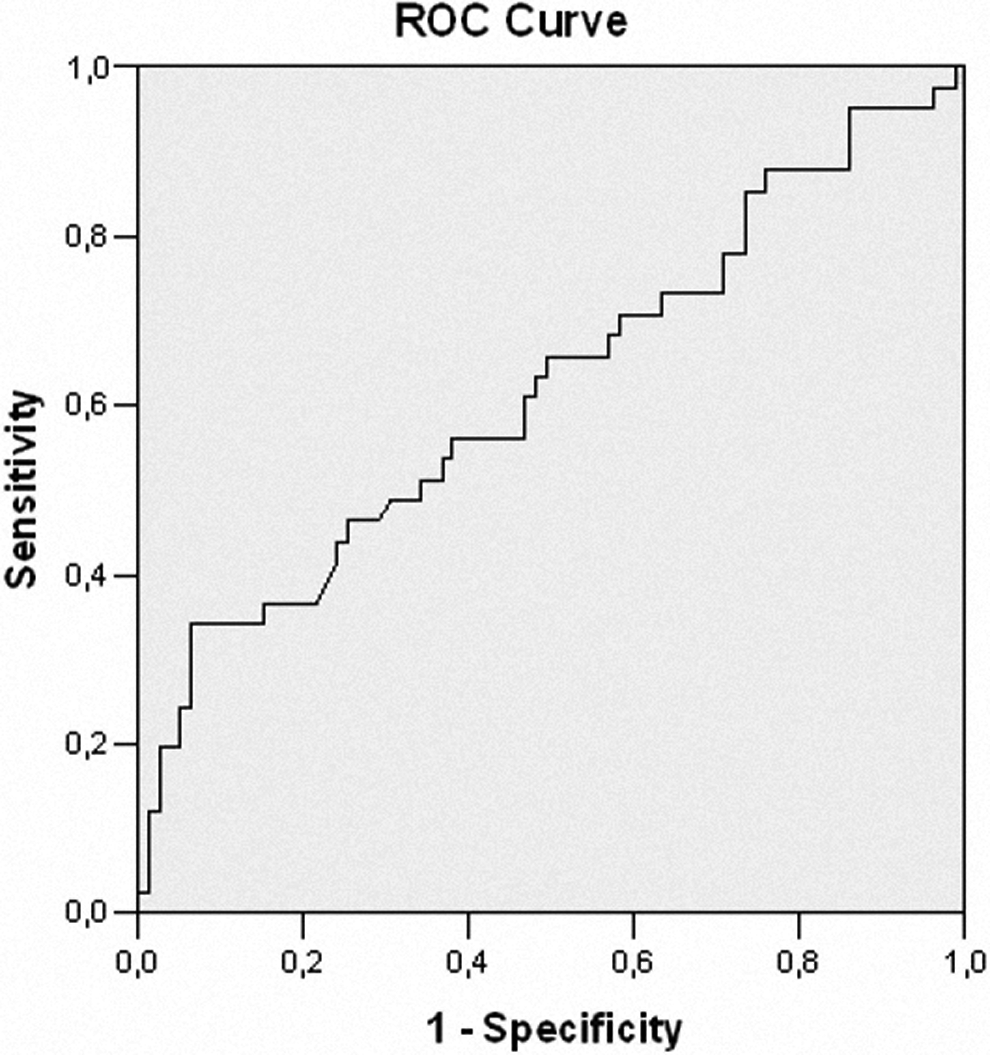
The receiver–operating characteristic (ROC) curve analysis of neutrophil-to-lymphocyte ratio for the prediction of saphenous vein graft disease.
Laboratory Parameters of Groups.
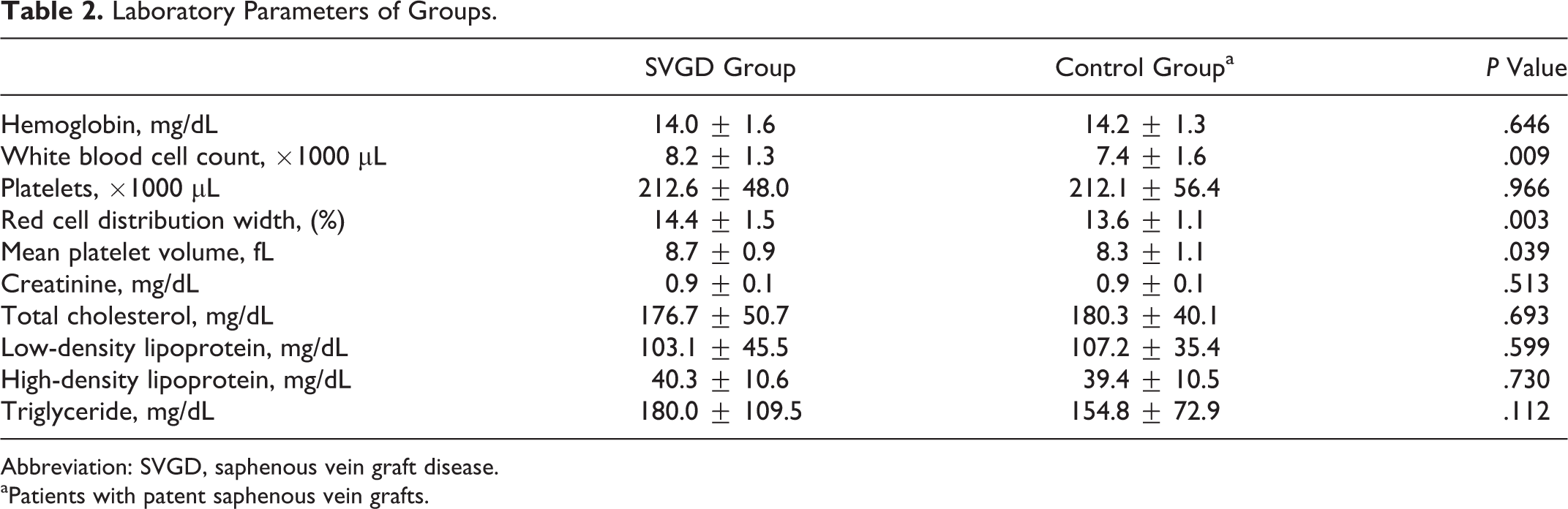
Abbreviation: SVGD, saphenous vein graft disease.
aPatients with patent saphenous vein grafts.
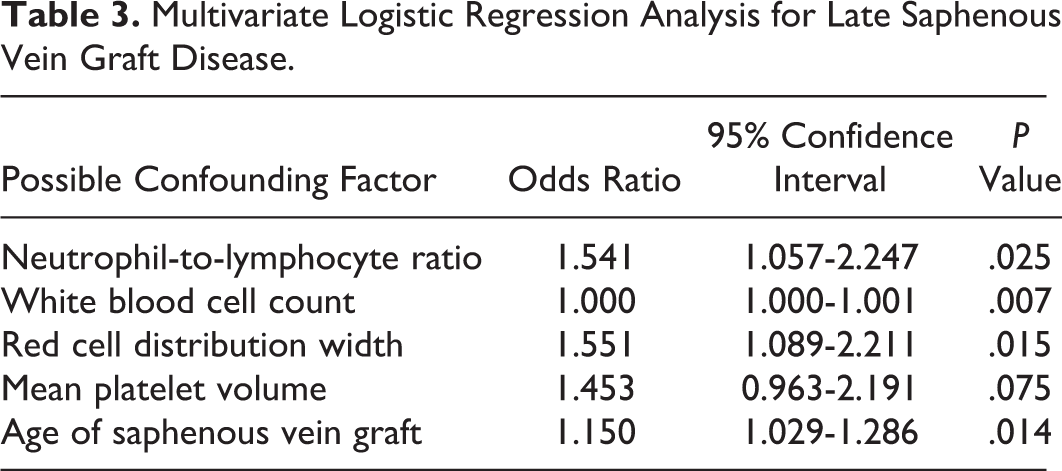
In univariate logistic regression analysis, NLR, WBC, RDW, MPV, and age of the SVG remained for multivariate analysis. In multivariate regression analysis NLR, WBC, RDW, and age of the SVG were shown to be independent predictors of SVGD (Table 3).
Multivariate Logistic Regression Analysis for Late Saphenous Vein Graft Disease.
Discussion
To our knowledge, for the first time by our study, NLR was evaluated in SVGD, and we found that NLR can be used as a predictor of SVGD together with the age of SVG, WBC count, and RDW.
Coronary artery bypass surgery, when indicated, is a good option for the treatment of CHD. With appropriate indications and appropriate surgery, CABG gives significant mortality and morbidity benefits to the patients with CHD. Both arterial and venous conduits are available, and they have been frequently used in this surgical procedure. Although patency rates for left IMA is excellent, it cannot be used for all stenotic vessels. For this reason, SVGs are frequently preferred counduits in the CABG surgery. Besides its benefits on revascularization, higher rates of graft occlusion remain to be a challenging issue. It is known that there is approximately 50% occlusion rates for saphenous grafts after 10 years of CABG surgery. 1
At this point, possible causative and risk factors for graft occlusion have been investigated. For example, Tavil et al found that MPV, LDL, and age of SVG were significant predictors of SVGD. 9 Iwama and colleagues showed that plasma homocysteine levels might be associated with SVGD. In another study, it was shown that location of the saphenous graft and the diameter of vessel after anastomosis were affecting SVG patency rates. 10 Classical CHD risk factors, graft age, diameter of native vessel, and severity of bypassed proximal coronary lesion were also suggested as predisposing factors of SVGD. 11 Recently in another study, it was found that RDW was an independent predictor of SVGD. 12
The NLR is significantly related to long-term prognosis in various conditions. For example, Azab et al showed in their 4-year follow-up study that NLR was closely related to MACEs in patients with diabetes mellitus. 13 In another follow-up study, it was shown that NLR is an independent marker of cardiovascular mortality. 14 Tamhane et al showed in their study that NLR is a useful marker in risk stratification, and it is also useful for the prediction of prognosis after acute coronary syndromes. 15
The predictor power of NLR for adverse cardiovascular events and poor prognosis is also valid for atherosclerotic diseases. Because WBCs and its subtypes are closely related to atherosclerotic heart disease, it was shown that they can also be used in the prediction of future cardiovascular events in atherosclerotic disease processes. 16 In a study, it was shown that elevated preprocedural WBC count is closely related to long-term mortality after percutaneous coronary intervention. 17 Turak and colleagues proposed that NLR is a useful marker in the prediction of bare metal stent restenosis. 18 The possible relationship between NLR and severity of CHD was studied in another study, and in this study, it was shown that high level of NLR was an independent predictor of severe atherosclerosis. 19
In light of these data, it can be thought that there is a close relationship between atherosclerotic diseases with NLR. Because atheroclerosis is the most significant pathologic insult in late SVGD and because SVGD is associated with worse prognosis, we hypothesized that higher levels of NLR might be a marker of SVGD. According to the findings of present study, we showed for the first time that NLR is an independent predictor of SVGD. Besides NLR, age of the SVG, RDW, and WBC are significantly and independently related to SVGD. Although MPV values were significantly higher in patients with SVGD, it did not remain as an independent predictor of SVGD in logistic regression analysis. Our findings suggest that although WBC count is important for SVGD, its subtypes also have significant role in this pathologic state. Because neutrophils and lymphocytes act in different manner by their cytokines and receptors, they may have different roles in different inflammatory situations. In this regard, neutrophils may be more responsible for the development and progression of atherosclerosis when compared to lymphocytes. According to our findings, it can also be interpreted that neutrophils might have a dominant role in the development of SVGD, which is also an atherosclerotic process. Pathophysiology underlying these findings is not clear for now, but it should be sought by further studies. Because increased time interval after CABG surgery leads to the degeneration of grafts, increased SVG age is also useful for the prediction of SVGD. Another CBC parameter, RDW, can also be used as a marker of SVGD. Increased RDW levels show poor prognosis; and according to our findings, its levels are closely related to SVGD.
Conclusions
The present study is the first report about the association of NLR with SVGD in patients with coronary bypass. The results may have clinical significance, because NLR is easily available, widely used, and relatively cheap compared to most other laboratory markers. Besides NLR, WBC count, SVG age, and RDW can also be used as a predictor of SVGD.
Limitations
The main limitation of this study is the limited number of study participants. Another limitation of this study is that it provides no information regarding the cause or effect relationship between NLR and atherosclerosis. Being a retrospective study, spot laboratory parameters rather than follow-up values are also among limitations of our study. But with its findings, our study gives novel findings in SVGD, and it can be helpful in designing of further studies in SVGD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.