
Abstract
Inflammation has recently emerged in the pathogenesis of several cardiovascular disorders, including arrhythmias. The neutrophil–lymphocyte ratio (NLR) is a simple marker for the assessment of inflammatory status. Therefore, we aimed to investigate the relationship between the NLR and the ventricular premature contraction (VPC) existence. Patients aged between 18 and 40 years who were referred to the cardiology clinic were enrolled in the study. All patients’ complete blood counts and 24-hour Holter recordings were analyzed. The NLR was higher within the VPC group compared to the control group (P < .001). According to the NLR tertiles, VPCs were more common in the higher NLR tertile (P < .001). A cutoff point of 1.80 for the NLR had 71% sensitivity and 60% specificity in predicting VPC in apparently healthy individuals. After multivariate analysis, only the NLR remained significant predictor of presence of VPC. In conclusion, the NLR is independently and significantly associated with VPC existence.
Introduction
Ventricular premature contractions (VPCs) are commonly seen in daily practice. They are usually associated with no clinical significance in structurally normal hearts. The VPCs have an estimated prevalence of 1% to 4% in the general population. 1 The importance of VPCs is due to accumulating evidence showing VPCs as a possible cause of reversible cardiomyopathy. 2 –5 They may cause distressing and sometimes troubling symptoms such as palpitations, presyncope, syncope, chest pain, and heart failure. Over the past decade, there has been accumulating evidence implicating inflammation in the pathogenesis of some arrhythmic disorders such as atrial fibrillation. As the inflammatory states, such as myocarditis, pericarditis, and cardiac surgery, are frequently associated with VPCs, we suspect inflammation has a role in VPC development. The neutrophil-to-lymphocyte ratio (NLR) was found to be associated with severity and prognosis of several cardiovascular diseases in different studies. 6 –9 The role of the inflammatory status in apparently healthy individuals with VPCs is unknown, so in this particular study we investigated the association between the NLR and the VPC.
Methods
Study Population
We retrospectively collected patients aged between 18 and 40 years having ambulatory Holter electrocardiogram monitoring between 2011 and 2013. The study group included 104 patients with at least 1 VPC, whereas the control group consisted of 100 patients with no VPC. The study group was further categorized according to VPC frequency as rare, occasional, and frequent: a frequency of <5 PVCs/h was termed “rare,” 5 to 10 PVCs/h was considered “occasional,” and >10 PVCs/h was defined “frequent.” 10 The study and control groups had normal physical and echocardiographic examinations with no cardiovascular risk factors. Patients with arrhythmic disorders other than VPCs, thyroid disorders, active infection, anemia, and smoking were excluded from the study. The local ethics committee approved the study.
Biochemical Measurements
Venous blood samples were drawn at initial presentation from the “antecubital” vein. Total and differential leukocyte counts and routine biochemical tests, including C-reactive protein (CRP) levels, were performed.
Holter Monitoring
The 24-hour Holter recordings were independently analyzed by 2 cardiologists. Patients having sufficient recordings during at least 18 of the 24 hours were enrolled in the study. Recordings were scanned for frequency and the site of origin of VPCs. In the Holter recording, the lowest, mean, and highest heart rates were evaluated. The VPCs were expressed as number per 24 hours. Patients having ventricular tachycardia (3 consecutive wide QRS with a rate of
Statistical Analysis
Data were analyzed with the SPSS software version 16.0 for Windows (SPSS Inc, Chicago, Illinois). The Kolmogorov-Smirnov test was used to verify the normality of the distribution of continuous variables. Continuous variables were defined as mean ± standard deviation; categorical variables were given as percentages. The independent sample t test or the Mann-Whitney U test was used for continuous variables and the chi-square test for categorical variables. One-way ANOVA or Kruskal-Wallis test was performed for the comparison of multiple groups. Pearson or Spearman tests were used for correlation analysis. Statistical significance was defined as P < .05. Multivariate logistic regression analysis was performed to assess the independent predictors of VPC. All variables found significant in the univariate analysis were included in the logistic regression model, and the results are shown as odds ratio (OR) with 95% confidence intervals (CIs). Receiver–operating characteristic (ROC) curve analysis was used to determine the optimum cutoff levels of the NLR in association with VPC.
Results
According to the presence of VPC, the NLR was significantly higher in the VPC group compared to the control group (2.33 ± 0.84 vs 1.87 ± 0.68, P < .001). Patients were divided into 3 tertiles based on the NLR levels, 1.36 (1.31-1.40) in tertile 1, 1.92 (1.87-1.96) in tertile 2, and 2.96 (2.80-3.12) in tertile 3. According to the NLR tertiles, baseline demographic, hematological, and Holter parameters of the patients are shown in Table 1. There were no statistically significant differences between the groups with respect to age, gender, body mass index, CRP, hemoglobin, and mean, maximum, and minimum heart rates. The VPCs were significantly higher among patients in the upper NLR tertile than that of the middle and lower NLR tertile groups (23 [0-812] vs 10 [0-104] P < .001 and 23 [0-812] vs 0 [0-1] P = .001, respectively). There was no significant difference between the middle and lower NLR tertile groups in terms of VPCs (10 [0-104] vs 0 [0-1] P = .256). Table 2 shows the characteristics of the patients who were categorized according to VPC frequency as absent, rare, occasional, and frequent. When we dichotomized the frequency groups as “frequent VPC” and “no frequent VPC,” the CRP levels were significantly lower in the latter one (0.38 ± 0.21 vs 0.32 ± 0.17, P = .05). According to the Spearman test, a positive correlation was observed between the VPC number and the NLR and CRP (r = 0.386, P < .001 and r = 0.142, P = .043, respectively). On multivariate regression analysis, only the NLR remained a significant predictor of VPC existence (OR: 3.039, 95% CI: 1.343-6.876, P = .008). The ROC curves explored the relationship between the NLR and the presence of VPC. Using a cut point of 1.80, the NLR predicted the presence of VPC with a sensitivity of 71% and specificity of 60% (ROC area under curve: 0.683, 95% CI: 0.609-0.757, P < .001; Figure 1).
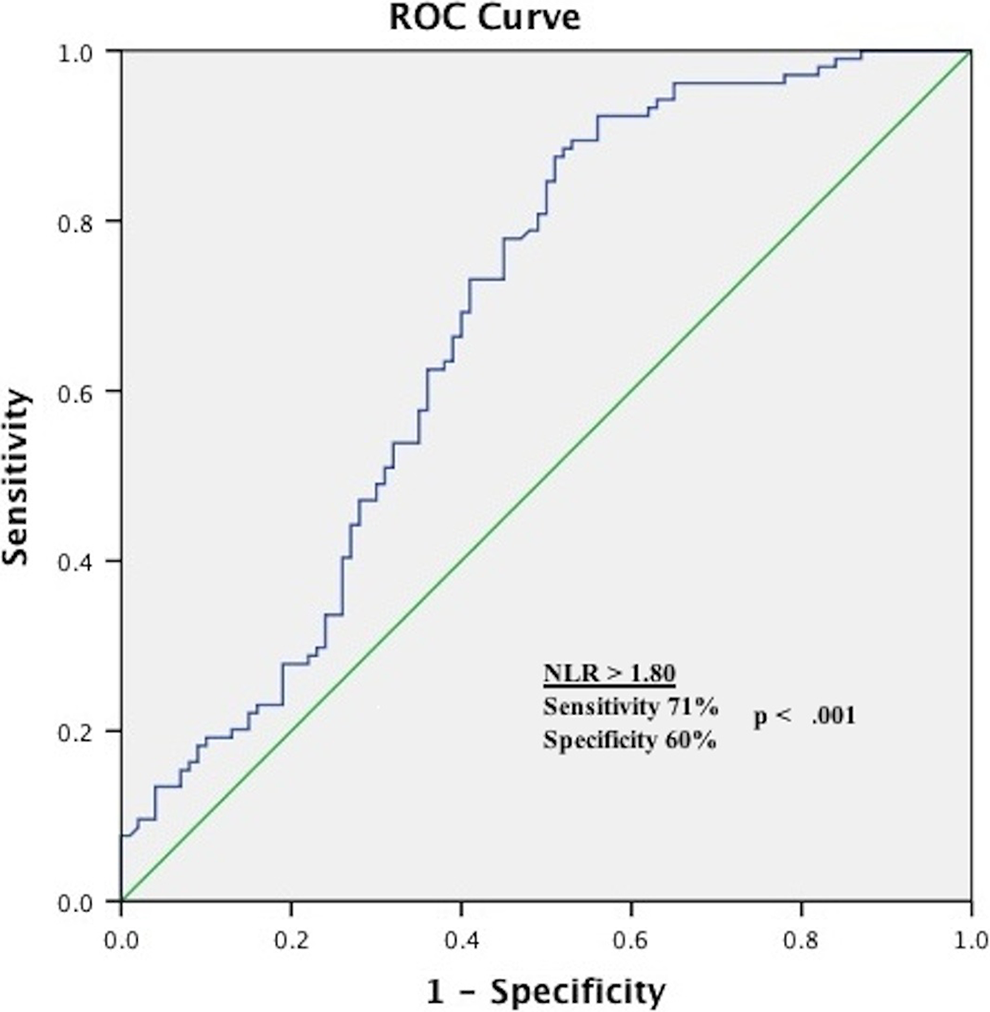
Receiver–operating characteristics curve of neutrophil-to-lymphocyte (NLR) for predicting the presence of ventricular premature contractions.
Clinical and Hematological Characteristics of Patients According to Neutrophil-to-Lymphocyte Ratio Tertiles.a
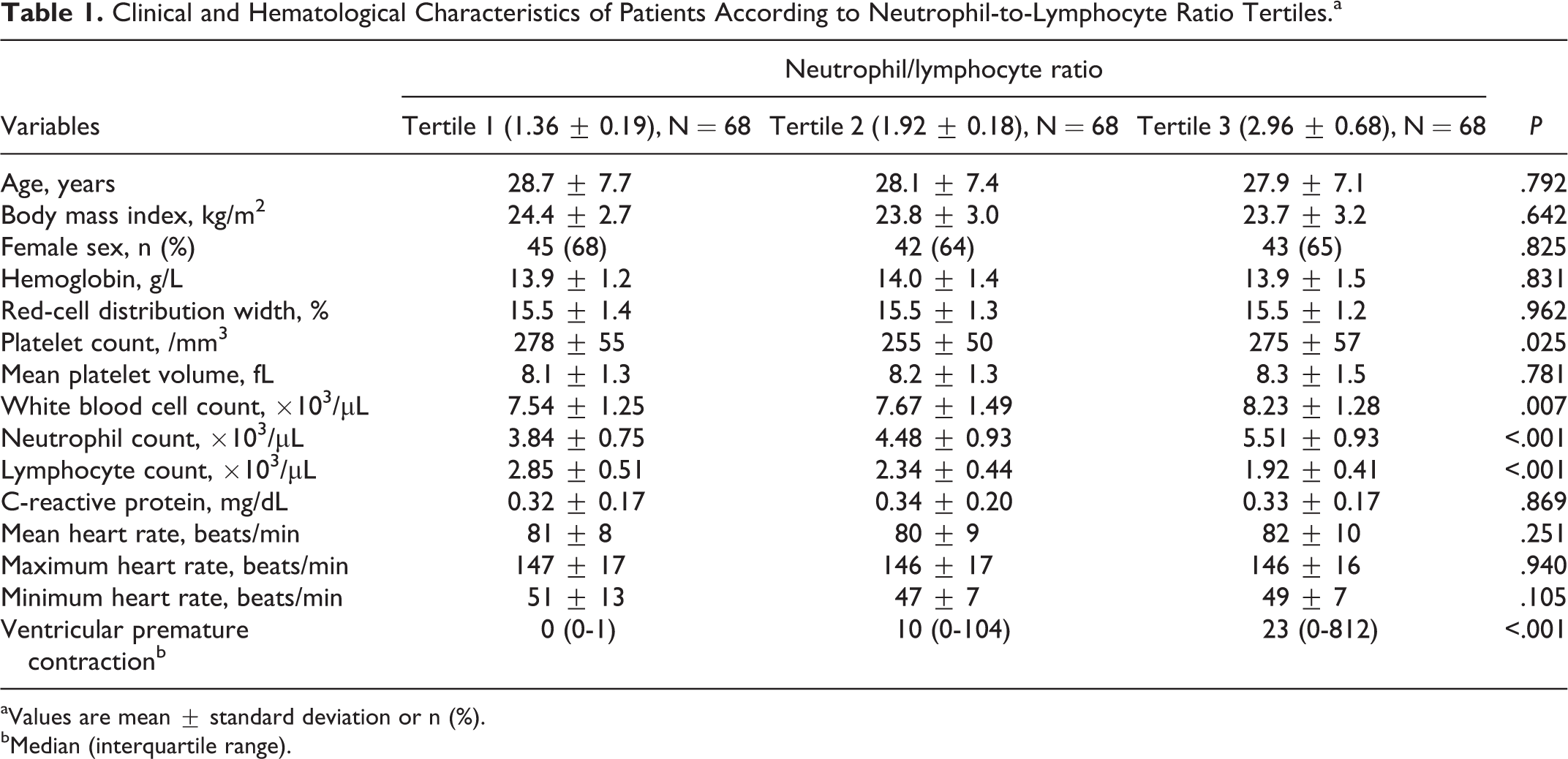
aValues are mean ± standard deviation or n (%).
bMedian (interquartile range).
Characteristics of Patients According to the Frequency of Ventricular Premature Contractions.a
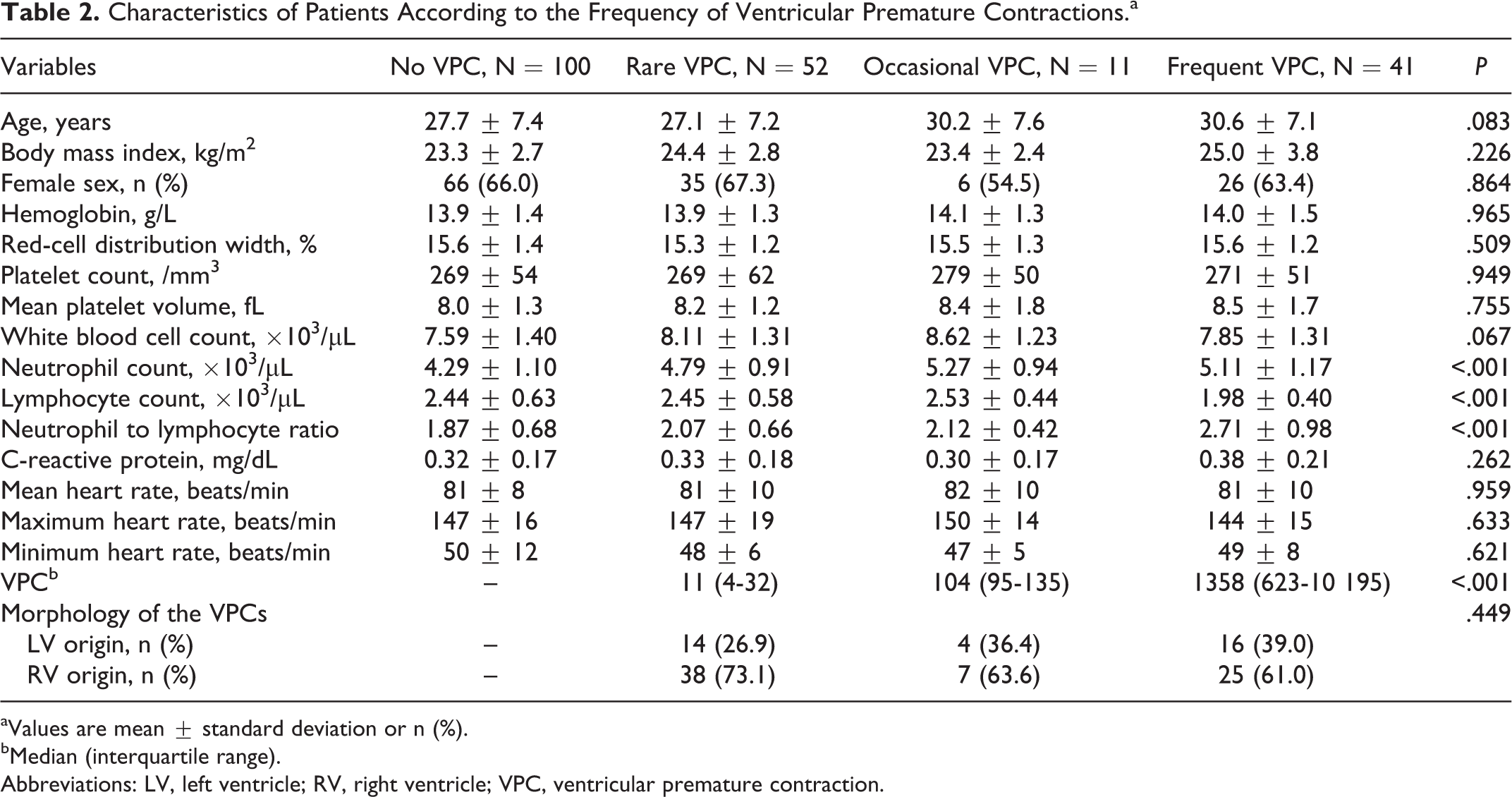
aValues are mean ± standard deviation or n (%).
bMedian (interquartile range).
Abbreviations: LV, left ventricle; RV, right ventricle; VPC, ventricular premature contraction.
Discussion
In the present study, we found that an increased NLR, a reliable marker of inflammation, was statistically and independently associated with presence and frequency of VPCs. An NLR
The VPCs are commonly encountered arrhythmias in clinical practice. The vast majority of VPCs are clinically asymptomatic, but they can cause limiting symptoms in some patients. The clinical significance of VPCs is determined based on the presence of structural heart disease. In more than half of the patients, VPCs occur in the same mechanism as ventricular tachycardia in which catheter ablation is the curative treatment.
In patients without structural heart disease, as previously reported, VPCs more commonly originated from the right ventricle than the left, and the majority of these right-ventricular VPCs were from the right-ventricular outflow tract. 11 The arrhythmia mechanism is believed to be caused by triggered activity secondary to cyclic adenosine monophosphate-mediated delay after depolarizations. 12,13 Consistent with the literature, VPCs were 67.3% right sided and 32.7% left sided in our study population without a difference in the frequency groups.
Inflammation has been involved in the pathogenesis of several cardiovascular diseases, especially atherosclerosis. 14,15 Recent studies demonstrated the predictive and prognostic significance of the NLR in a wide range of cardiovascular diseases. 6 –9,14,15 There is now also strong evidence linking inflammation to the initiation and propagation of AF. 16,17 The role of inflammation in the initiation of AF was initially suspected by the observation that inflammatory states, such as myocarditis, pericarditis, and cardiac surgeries, are frequently associated with AF. 18 –20 Likewise, there has been a close relationship between VPC and myocardial inflammatory conditions. 21,22 In addition, circulating proinflammatory cytokines (interleukin 6 and tumor necrosis factor α) were found to be higher in the serum of young patients with ventricular arrhythmias and without structural heart disease compared to healthy participants. 23 In relation to the development of VPC, the inflammatory process may be involved in electrophysiological and structural ventricular remodeling.
The predictive capability of the NLR in identifying patients who will respond to cardiac resynchronization therapy was shown in patients with heart failure in which dyssynchrony is a substantial problem. 24 The ventricular dyssynchrony associated with VPCs causes dilatation of the left ventricle and impaired systolic function in a manner formerly defined for patients with permanent right ventricular pacing or left bundle branch block. 25 –27 It is not known why the majority of patients with frequent VPCs have a benign course, whereas up to one-third of them develop cardiomyopathy. Further large-scale cohorts are needed to clarify and confirm this association between the NLR and the VPCs, which might be promising in identifying patients who will develop cardiomyopathy.
The VPCs can be recorded in a wide range of clinical circumstances, from healthy persons to patients with severe structural heart disease. The prognostic importance differs depending on the underlying condition. In the absence of heart disease and frequent VPCs patients should be reassured, and no specific treatment should be required if they are relatively asymptomatic. In the presence of symptoms, treatment with a β-blocker or a nondihydropyridine calcium channel blocker may be the first choice. 28
The possible limitations of the study include that it was single-centered, retrospective, and included a relatively small number of patients. As we included a relatively young group of patients and excluded patients with triplets, the generalizabilty of the study was hindered. Usage of a single blood sample will not presume the persistence of the NLR over time and may not reflect the relations between VPC and NLR. This study is unable to provide a causal relationship between VPC and NLR.
In conclusion, the NLR is an inexpensive, readily available, and reliable marker of inflammation, which has an independent association with VPC presence and frequency. Further large-scale studies are needed to confirm this association between the NLR and the VPCs.
Footnotes
Acknowledgment
We are grateful to Dicle University DUBAP for their sponsorship about English editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.