
Abstract
The aim of the study was to evaluate the utility of the preprocedural platelet–lymphocyte ratio (PLR) for predicting no reflow in patients undergoing primary percutaneous intervention (PCI) for the treatment of ST-segment elevation myocardial infarction. The thrombolysis in myocardial infarction (TIMI) flow grades of 287 patients treated with primary PCI were assessed retrospectively. Patients were divided into 3 tertiles based upon preprocedural PLR. Pre- and postprocedural TIMI flow grades were evaluated. No reflow developed in 6, 14, and 43 patients in the lower, middle, and higher tertiles, respectively (P < .001). After multivariate analysis, PLR remained a significant predictor of no reflow together with neutrophil–lymphocyte ratio (NLR). A cutoff value of 160 for PLR and 5.9 for NLR predicted no reflow with sensitivities and specificities of 75% and 71% and 74% and 70%, respectively. In conclusion, high preprocedural PLR and NLR levels are significant and independent predictors of no reflow in patients undergoing primary PCI.
Keywords
Introduction
Rapid restoration of coronary blood flow to the jeopardized myocardium is the crux of therapy, after acute myocardial infarction. The invention and usage of stents have made percutaneous coronary intervention (PCI) a safe, effective, and preferred reperfusion modality for the treatment of ST-segment elevation myocardial infarction (STEMI). 1 Nevertheless, even after patency of an infarcted artery was successfully achieved via stent implantation, sufficient myocardial reperfusion was not observed in 2.3% to 29% of patients in the setting of acute myocardial infarction, which is often called the no-reflow phenomenon. 2 –5 Despite the mechanical opening of the infarct-related artery (IRA), early postinfarction complications, adverse left ventricular remodeling, and in-hospital and long-term morbidity and mortality are increased in patients who develop no reflow. 6 –9
Inflammation has a substantial role in the initiation and propagation of the atherosclerotic process. 10 The platelet–lymphocyte ratio (PLR) has been recently proposed to be a marker of thrombotic and inflammatory state, mainly in patients with malignancies. 11,12 However, little is known regarding the PLR and its association with adverse outcomes in patients with cardiovascular diseases. 13 Thus, we sought to assess the predictive value of preprocedural PLR in the development of no reflow in patients undergoing coronary stent implantation for the treatment of STEMI.
Methods
Study Population
We analyzed the clinical and angiographic data of 319 consecutive patients diagnosed with acute STEMI within 12 hours of symptom onset. Patients undergoing conservative therapy (n = 6), thrombolysis (n = 3), or coronary artery bypass grafting (CABG) as the primary reperfusion strategy (n = 8) and patients with stent thrombosis (n = 7), prior CABG (n = 3), cardiogenic shock (n = 3), active infections (n = 3), cancers (n = 2), and anemia (n = 5) were excluded from the study. Moreover, patients on oral anticoagulant therapy (n = 7) and treated with thrombus vacuum aspiration therapy (n = 16) were not included in the study. An STEMI was defined as the presence of chest pain lasting longer than 20 minutes and associated with ST-segment elevation ≥1 mm in at least 2 limb electrocardiographic leads or ≥2 mm in at least 2 contiguous precordial leads or the presence of new left bundle branch block. 1 The diagnosis was confirmed by the elevation in troponin levels. The local ethics committee approved the study.
Biochemical Measurements
Venous blood samples were drawn when the patient initially presented to the emergency department or the coronary care unit before coronary angiography. The total leukocyte count as well as the differential and routine biochemical tests was measured using commercially available methods and kits (Abbott Cell-Dyn 3700 and Architect C16000 auto-analyzer; Abbott Laboratory, Abbott Park, Illinois).
Angiographic Analysis
Coronary angiography and PCI were performed through the femoral artery using the Judkins technique, and the angiograms were recorded digitally for quantitative analysis. All patients received oral acetyl salicylic acid (300 mg), clopidogrel (loading dose of 600 mg), and intravenous unfractionated heparin (100 U/kg) before PCI. The usage of glycoprotein IIb/IIIa antagonists was left to the operator’s discretion. Two cardiologists who were blinded to patients’ clinical situation assessed the pre- and postprocedural thrombolysis in myocardial infarction (TIMI) grade flows of the IRA. Angiographic no reflow was defined as a postprocedural TIMI flow grade ≤2 in the absence of dissection, residual stenosis, or vasospasm, and angiographic success was defined as TIMI grade 3 flow. 14,15
Statistical Analysis
Data were analyzed with SPSS software version 16.0 for Windows (SPSS Inc, Chicago, Illinois). The Kolmogorov-Smirnov test was used to verify that continuous variables were normally distributed. Continuous variables are listed as mean ± standard deviation or mean (minimum–maximum); categorical variables are listed as percentages. The independent sample t test or the Mann-Whitney U test was used for continuous variables and the chi-square test for categorical variables. One-way analysis of variance followed by Scheffe test or Kruskal-Wallis test was performed for the comparison of multiple groups. The Pearson or Spearman test was used for correlation analysis. Statistical significance was defined as P < .05. Multivariate logistic regression analysis was performed to assess the independent predictors of no reflow. Variables with a P value of < .10 in univariate analysis were included in the logistic regression model and results are shown as an odds ratio (OR) with 95% confidence intervals (CIs). A receiver–operating characteristic (ROC) curve analysis was used to determine the optimum cutoff level for the PLR and neutrophil–lymphocyte ratio (NLR) values that best predicted no reflow.
Results
A total of 287 patients with a mean age of 60.8 ± 13.6 years were enrolled in the study. Patients were divided into 3 tertiles based upon preprocedural PLR. The baseline demographic, biochemical, hematological, and angiographic data of the patients according to the PLR tertiles are presented in Table1. The patients in tertile 3 were more likely to be older, have higher glucose levels, and platelet and neutrophil counts than those in tertiles 1 and 2. In contrast, lymphocyte counts and the incidence of smoking were lower in tertile 3. No reflow developed in 6, 14, and 43 patients in the lower, middle, and upper tertiles, respectively (P < .001; Figure 1). No significant differences in gender, lipid parameters, diabetes or hypertension, renal function, and distribution of target vessel were observed between the groups. The preprocedural PLR positively correlated with the NLR and age (r = .697, P < .001 and r = .191, P = .001; respectively). Higher preprocedural PLR and NLR values were found to be associated with no reflow by logistic regression analysis (Table 2). In the ROC analysis, PLR >160 had 75% sensitivity and 74% specificity (ROC area under curve: .798, 95% CI: 0.730-0.866, P < .001) and NLR >5.9 had 71% sensitivity and 70% specificity in predicting no reflow (ROC area under curve: .782, 95% CI: 0.710-0.853, P < .001; Figure 2).
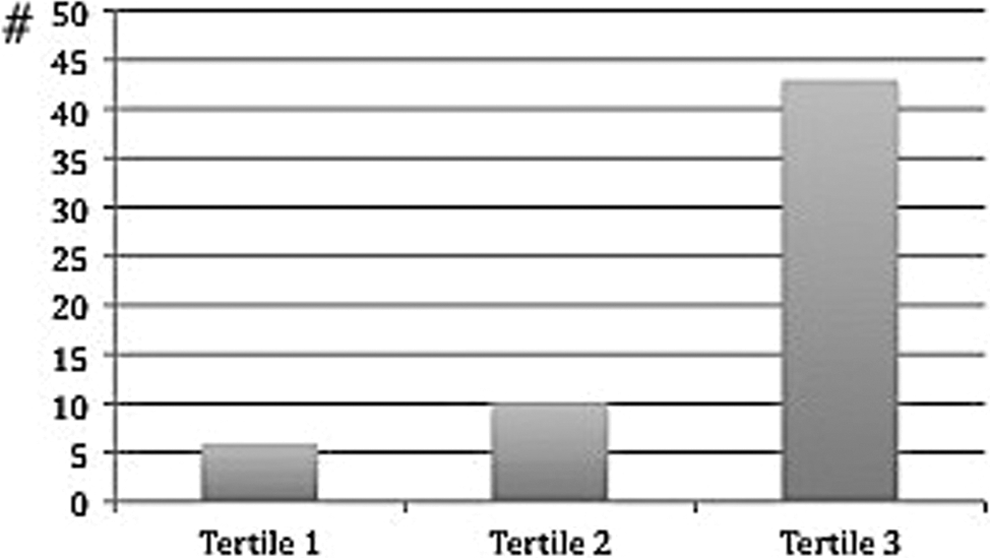
No reflow development according to platelet/lymphocyte tertiles.
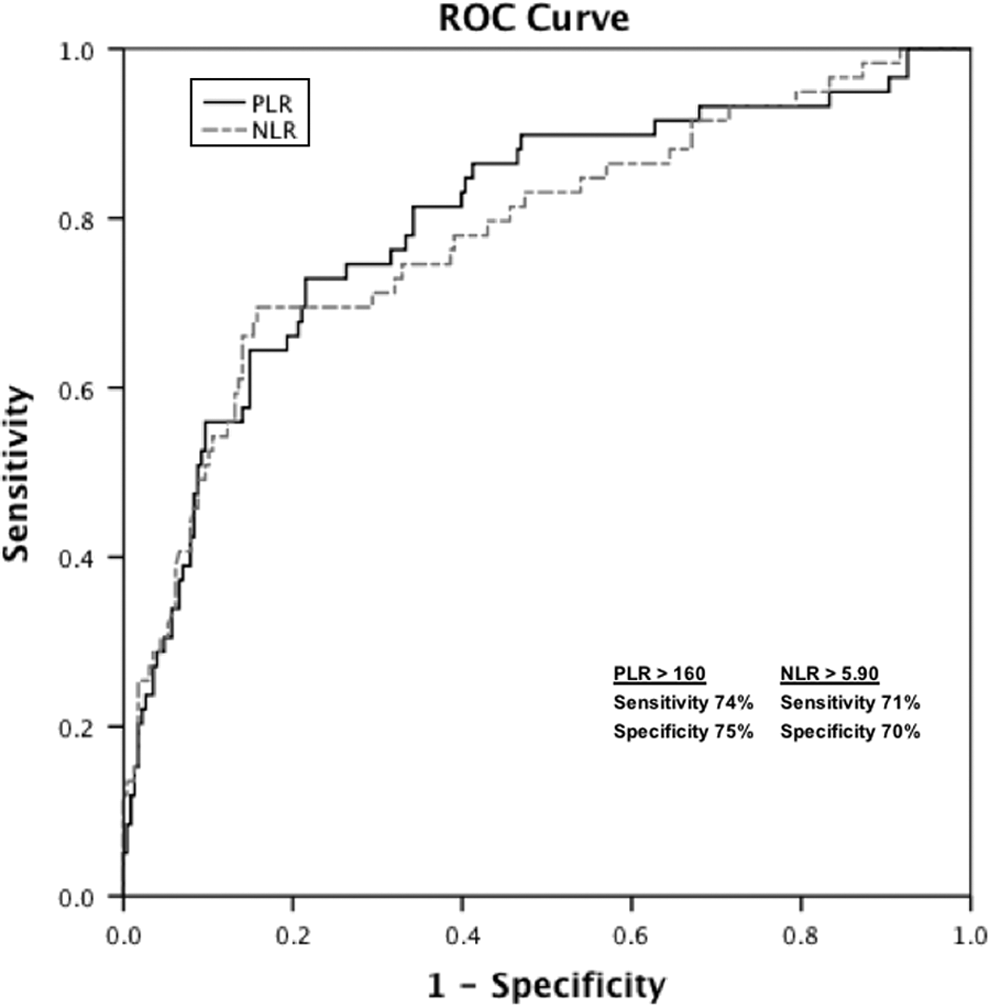
Receiver–operating characteristics curve of platelet–lymphocyte (PLR) and neutrophil–lymphocyte ratios (NLR) for predicting development of no reflow.
Baseline Characteristics, Hematological, and Angiographic Data of the Patients According to PLR Tertiles.
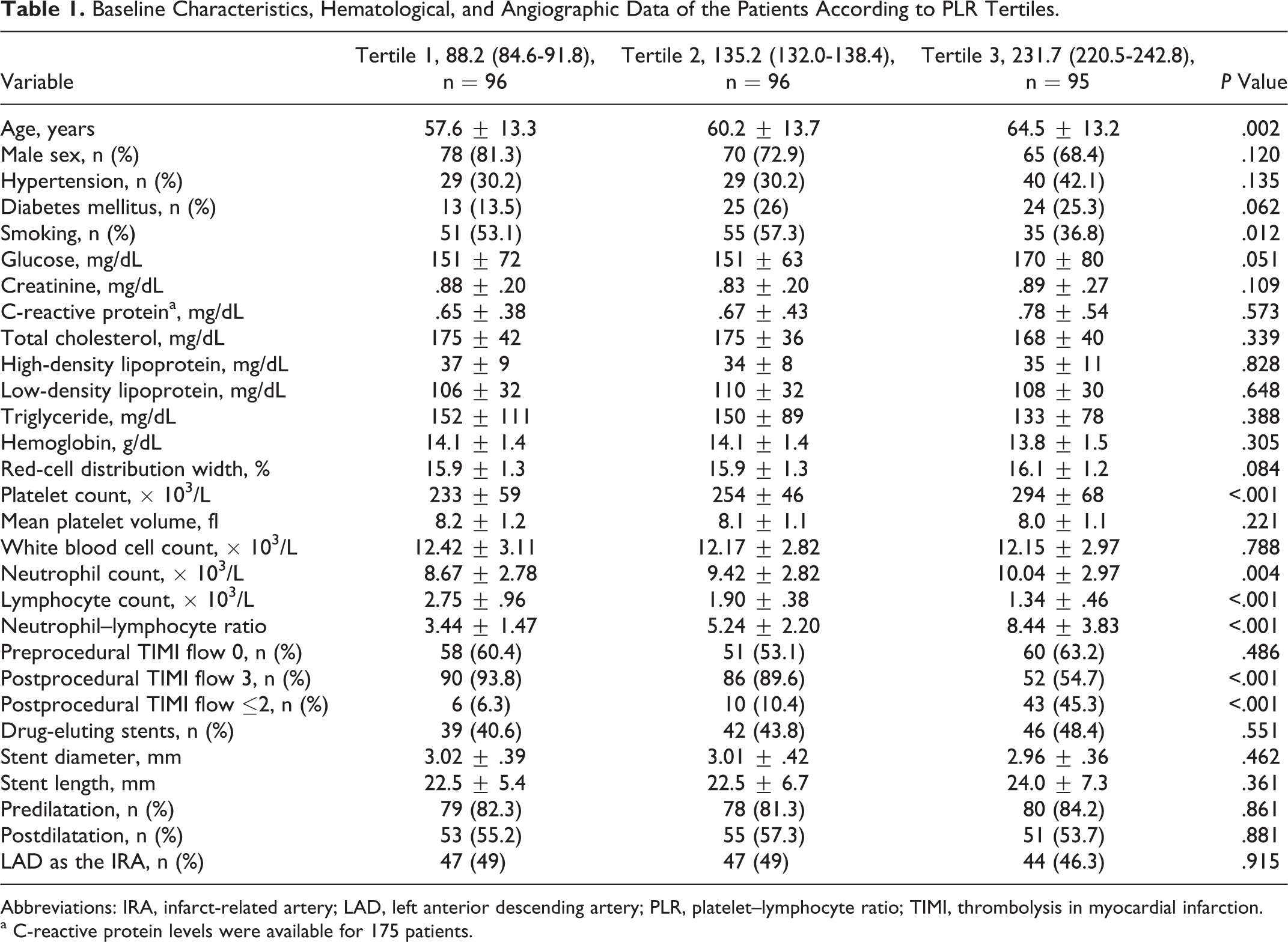
Abbreviations: IRA, infarct-related artery; LAD, left anterior descending artery; PLR, platelet–lymphocyte ratio; TIMI, thrombolysis in myocardial infarction.
a C-reactive protein levels were available for 175 patients.
Effects of Variables on the No Reflow in Univariate and Multivariate Logistic Regression Analyses.
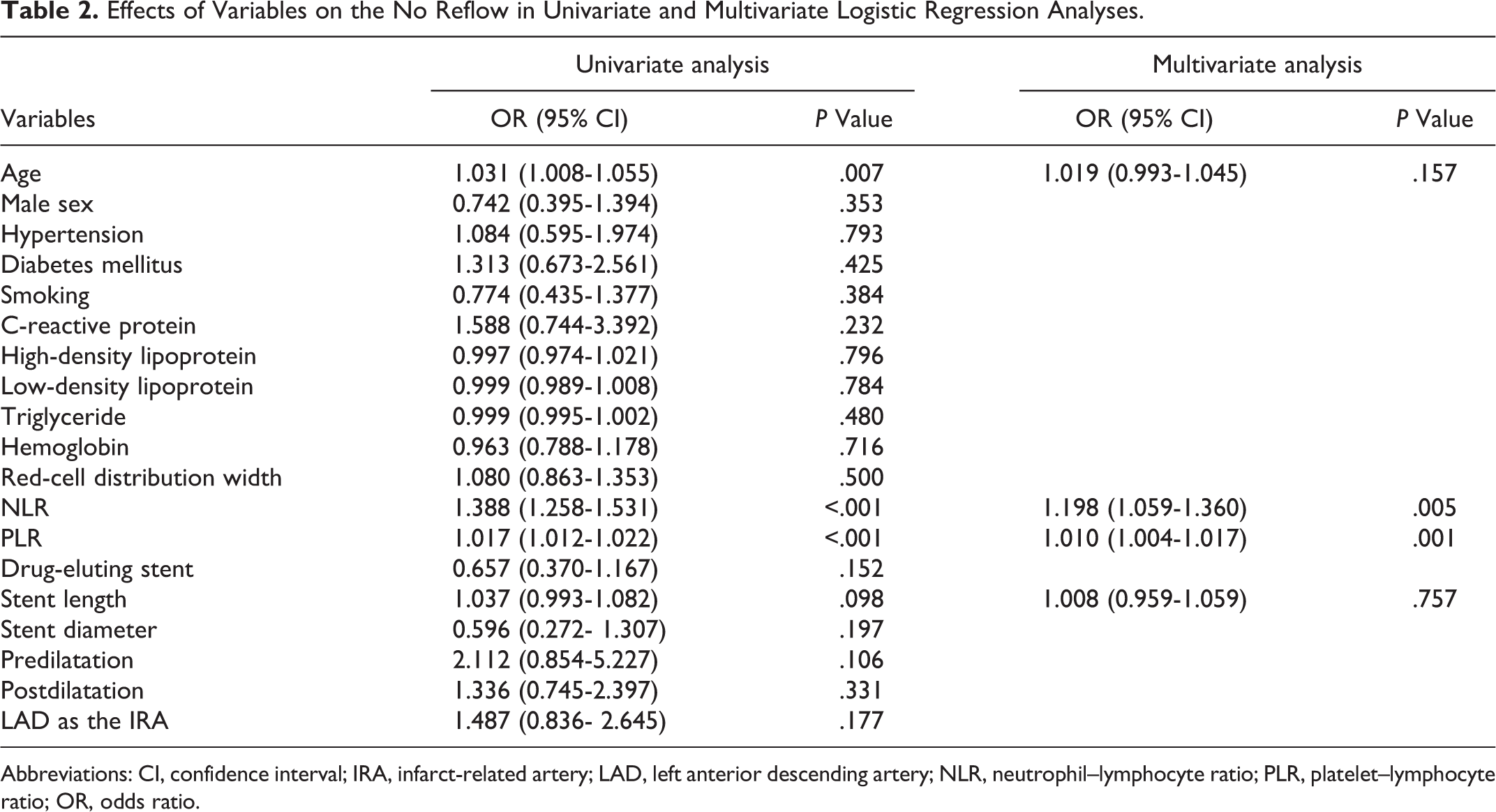
Abbreviations: CI, confidence interval; IRA, infarct-related artery; LAD, left anterior descending artery; NLR, neutrophil–lymphocyte ratio; PLR, platelet–lymphocyte ratio; OR, odds ratio.
Discussion
In the present study, we found that increased PLR and NLR levels were strongly and independently associated with the development of no reflow in the setting of acute STEMI. A preprocedural PLR >160 had 75% sensitivity and 74% specificity and NLR >5.9 had 71% sensitivity and 70% specificity for predicting no reflow in patients undergoing primary stent implantation.
Although several mechanisms have been proposed to explain the no reflow phenomenon, the pathophysiology of no reflow has not yet been completely understood. Some of the contributing factors in the occurrence of no reflow are distal atherothrombotic embolization, mechanical microvascular leukocytes and platelets plugs, in situ thrombosis, ischemic endothelial edema and damage, vasospasm, free oxygen radicals, and susceptibility of the coronary microcirculation to injury. 16 –18
The close interplay between inflammation, coagulation, and atherosclerosis progression has become a field of intensive research. White blood cell count and the differential, C-reactive protein and the NLR are some of the inflammatory markers that were demonstrated to have predictive and prognostic significance in a wide range of cardiovascular diseases. 9,19 –24 In our study, the NLR was independently associated with no reflow, thus confirming previous studies. 9 However, similar to Niccoli et al, we failed to find a relationship between serum levels of C-reactive protein measured within 24 to 72 hours of admission and the prevalence of no reflow. 25
In the setting of acute myocardial infarction, as a result of the stress response to myocardial ischemia, the leukocyte differential shifts toward a decreased lymphocyte and increased neutrophil count. 26 Lymphocytes represent a more appropriate immune response, while neutrophils cause an uncontrolled inflammatory reaction. 27 In several studies, the NLR has been found to be associated with worse prognosis in patients with atherosclerotic heart disease. 7,9,28,29 Likewise, we found an increased NLR in patients with impaired TIMI flow after primary PCI.
Megakaryocytic proliferation and relative thrombocytosis are consequences of an ongoing inflammatory response that results in a prothrombotic state. High platelet count, platelet activation, and plugging are proved to have a marked importance in the no reflow development because of the increased propensity to form platelet-rich thrombi and vasoconstriction due to the release of vasoactive mediators.
Prior studies have shown the association between major adverse cardiovascular outcomes and both higher platelet and lower lymphocyte counts. 27,30,31 Additionally, the diagnostic and prognostic utilities of a low lymphocyte count were demonstrated in patients with myocardial infarction and chronic coronary artery disease, respectively. 32,33 The advantage of the PLR is that it reflects both hyperactive coagulation and inflammatory pathways, and it may be superior to either the individual platelet or the lymphocyte counts in the prediction of impaired reperfusion.
The prognostic significance of the PLR has been demonstrated in patients with various cancers. 11,34 Some cardiovascular studies with PLR have also been performed. In a study by Azab et al, higher PLR values were associated with increased long-term mortality in patients with non-STEMI. 13 Sunbul et al found that the PLR was a significant predictor of nondipper status in patients with hypertension. 35 Recently, Acar et al demonstrated the independent relationship between the PLR and the coronary collateral development in patients with chronic total occlusions. 36
Our study has some limitations. Myocardial contrast echocardiography and magnetic resonance perfusion imaging, which are the gold standard methods to assess no reflow, could not be performed because of the retrospective design of the study. The study was single center and included a relatively small number of patients. The lack of postprocedural myocardial damage measurement (troponin and/or maximum creatine kinase MB) is another limitation. Despite these limitations, to our knowledge, this is one of the first studies evaluating the predictive value of preprocedural PLR on the development of no reflow in the setting of STEMI treated with primary PCI.
In conclusion, high preprocedural PLR is a significant and independent predictor of no reflow together with NLR in patients with acute STEMI undergoing primary PCI. Further large-scale, prospective and multicenter studies are needed to clarify and confirm the association between the PLR, NLR, and no reflow, which might be promising in identifying patients who need prophylactic treatment.
Footnotes
Acknowledgment
We are grateful to Dicle University DUBAP for their sponsorship about English editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.