
Abstract
Aim:
The aim of this study is to examine the relationship between initial magnesium (Mg) levels, electrocardiographic no-reflow, and long-term mortality in patients who underwent primary percutaneous coronary intervention (pPCI) due to ST-segment elevation myocardial infarction (STEMI).
Methods:
A total of 111 patients with pPCI participated in the study. Magnesium and high-sensitive C-reactive protein (hs-CRP) were measured. The sum of ST-segment elevation was measured immediately before and 60 minutes after the restoration of coronary flow. The difference between the 2 measurements was taken as the amount of ST-segment resolution and defined as sum of ST-segment resolution (∑STR). The ∑STR <50% was determined as electrocardiographic sign of no-reflow phenomenon. After the patients were discharged, they were followed up for major adverse cardiac events for up to 51 months after discharge.
Results:
Forty patients in the no-reflow group and 71 patients in the normal-flow group were included in the study. Magnesium value ≤1.87 mg/dL initially measured had 77% sensitivity and 59% specificity in predicting no-reflow on receiver operating characteristic curve analysis. In multivariate analyses, Mg (odds ratio [OR]: 0.01, <95% confidence interval [CI]: 0.01-0.12; P = .004), hs-CRP (OR: 1.06, <95% CI: 1.00-1.14; P = .05), left anterior descending artery lesion (OR: 6.66, <95% CI: 1.45-3.05; P = .01), and reperfusion time (OR: 1.01, <95% CI: 1.00-1.01; P = .03) were still independent predictors of electrocardiographic no-reflow, and only Mg (OR: 0.08, <95% CI: 0.01-1.03; P = .05) was still an independent predictor of long-term mortality.
Conclusion:
Serum Mg level is an independent predictor of electrocardiographic no-reflow and long-term mortality in patients with STEMI.
Keywords
Introduction
Primary percutaneous coronary intervention (pPCI) is the first choice of treatment in patients with ST-segment elevation myocardial infarction (STEMI). 1 It has been shown that adequate perfusion is not provided at the tissue level, although normal flow in epicardial coronary artery is provided in one-third of patients with STEMI. 2 This situation, in which myocardial perfusion cannot be achieved without a mechanical barrier such as coronary arterial obstruction blocking the flow after PCI, dissection, or spasm, is called as “no-reflow” phenomenon. 3 It has been demonstrated in various studies that this case, in which perfusion is inadequate in microvascular level, is associated with poor prognosis. 4,5 Thus, the aim of the treatment has changed to reflow on the microvascular level in patients with STEMI. Although the underlying causes related to no-reflow have not yet been fully understood, various mechanisms such as increased oxidative stress, inflammation, and increased platelet activation have been suggested for the pathogenesis of the no-reflow phenomenon. 6 –8 Even if it can be used in many ways, tissue-level reperfusion is the most commonly used method in electrocardiographic assessment due to its reliability, simplicity, and accessibility. 9,10
Magnesium (Mg) is a major intracellular cation that plays an important role in many chemical reactions including the transmission system and the regulation of blood sugar and pressure. 11,12 It has been also demonstrated that Mg has a key role in vasomotor tone via active transportation of calcium (Ca) and potassium in cell membrane and the regulation of heart rate. By blocking L-type Ca channels, it reduces Ca loading and energy requirements. 12 Additionally, it has been shown that Mg increases the endothelial-dependent vasodilation, regulates lipid metabolism, and reduces platelet aggregation. 13,14 Moreover, in the studies conducted, Mg deficiency has been found to be related to increased inflammatory response, increased cytokines production, and reactive oxygen species. 15,16 Additionally, prior studies showed that hypomagnesemia is frequent in patients with heart failure and/or coronary artery disease (CAD), and it is related to mortality from CAD and all causes of mortality. 13
Factors that help to predict no-reflow have not been fully understood yet. The effects of hypomagnesemia and pathogenesis of no-reflow may be similar. Our hypothesis was that decreased Mg might be related to the existence of electrocardiographic no-reflow. This hypothesis was tested in patients with STEMI who underwent a primary angioplasty.
Methods
Study Population
Our study involved 146 patients with STEMI who underwent cardiac catheterization with pPCI between September 2010 and February 2011. Of these patients, 17 were not included due to chronic renal failure, 6 patients were excluded due to the presence of new onset of complete left bundle branch block, 6 others were excluded due to left ventricular hypertrophy, and 6 further patients were excluded due to the presence of thrombolytic treatment administration before pPCI. Thus, a total of 111 patients with pPCI participated in the study (mean age 61.3 ± 12.3 and 81.1% male). All of the participants signed an informed consent before the procedure, and the study was approved by our hospital ethics committee.
Definitions
Reperfusion time was defined as the time from the onset of chest pain to the first balloon inflation. Diabetes mellitus (DM) was diagnosed based on the history of diabetes treated with or without drug treatment. Hypercholesterolemia was defined as total cholesterol of ≥200 mg/dL. Multivessel disease was characterized through a stenosis of >50% of 2 or more major epicardial coronary arteries.
Coronary Angiography and pPCI Procedure
With the adoption of a standard femoral approach that uses a 7F-guiding catheter, the pPCI procedure was performed. After 10 000 IU heparin, 300 mg acetylsalicylic acid, and 600 mg clopidogrel were given, target lesion was crossed through 0.014-in wires. According to the operators’ decision, tirofiban was given with the pPCI simultaneously. Nonionic low-osmolality contrast agent was used in all patients. After angioplasty, all patients were admitted to the coronary care unit. In addition, they were given 100 mg acetylsalicylic acid and 75 mg clopidogrel. Concomitant medical treatment with β-blockers, angiotensin-converting enzyme inhibitors, and statins was prescribed in accordance with the American College of Cardiology/American Heart Association guidelines.
Laboratory Analysis and Electrocardiography
Antecubital venous blood samples for the laboratory analysis were collected during the admission to the emergency department. Serum Mg concentration was evaluated by means of a Roche/Hitachi modular analyzer with a xylidyl blue reaction according to the manufacturer’s instructions. The Mg levels were explained in milligrams per deciliter. In the first electrocardiography (ECG), measurements were taken immediately before angioplasty. During the second ECG obtained 60 minutes after pPCI, ST-segment elevation in millimeters was measured 20 milliseconds after the J-point. The total of ST-segment elevations was measured in leads DI, aVL, and V1 via V6 for anterior infarctions and in leads II, III, aVF, V5, and V6 for inferior infarctions. 17 The difference in the sum of ST-segment elevations that were measured before and after pPCI was defined as the sum of ST-segment resolution (∑STR). The ∑STR was compared to the sum of ST-segment elevations, which were measured before and after pPCI, and the percentage of the ∑STRs was obtained. According to the classification of Schroder, 18 patients with ∑STR <50% were accepted as having the electrocardiographic no-reflow phenomenon (group 1). Patients with ∑STR ≥ 50% were viewed as having the electrocardiographic normal-reflow (group 2).
Clinical End Points
All patients were followed up for 51 months prospectively. In the 51st month, we contacted the patients either onsite or via phone. The main end points in this study were the major adverse cardiac events (MACEs) explained as cardiovascular mortality, repeated target vessel revascularization (TVR), and remyocardial infarction (re-MI). Cardiovascular mortality in patients was defined as death related to myocardial ischemia and infarction, heart failure, arrhythmia (ventricular fibrillation, ventricular tachycardia, or asystole), and cardiac arrest due to other or undetermined causes or cerebrovascular accident. Target vessel revascularization was expressed as the need of PCI or coronary surgery in the target vessel caused by clinical symptoms such as the restenosis or reocclusion of the infarct-related artery. The re-MI was explained as a reelevation in creatine kinase (CK) that was twice of the last value related to Creatine Kinase Isoenzyme MB (CKMB) ≥ 10% of the total CK and ST-segment reelevations. 19
Statistics
Continuous variables were expressed as mean (SD). Categorical variables were expressed as percentages. The Student t test was used in order to compare parametric continuous variables. To compare nonparametric continuous variables, the Mann-Whitney U was used. The χ2 test was used to compare categorical variables. By means of the Kaplan-Meier method, the cumulative survival curves for long-term mortality were evaluated. To investigate the differences between the Mg groups, log-rank testing was utilized. In patients with STEMI, the receiver operating characteristic (ROC) curve was used to demonstrate the sensitivity and features of Mg and its respective optimal cutoff value for predicting poor coronary flow after pPCI. Forward stepwise multiple logistic regression analysis was used to investigate whether the independent predictors of electrocardiographic no-reflow and long-term mortality existed. All variables showing significance values <0.1 on univariate analysis were included in the model. Spearman or Pearson correlation coefficients were used to characterize the relationship between the variables. Two-tailed P values <.05 were considered as significant, and confidence interval (CI) was 95%. The SPSS program (version 20.0; SPSS, Chicago, Illinois) was used for all statistical studies. The results of the statistical P value <.05 were viewed to be significant.
Results
Forty patients (mean age 62.6 ± 12.1 and 85.4% male) were present in group 1, whereas 71 patients (mean age 60.5 ± 12.4 and 78.6% male) were in group 2. Baseline characteristics are shown in Table 1. Except hypercholesterolemia, the groups were similar in terms of cardiovascular risk factors, age, and previous medications (9.8% vs 22.9%, P = .08). For baseline laboratory status, the high-sensitive C-reactive protein (hs-CRP; 28.1 ± 49.5 vs 8.0 ± 9.7, P < .001) was significantly higher, and Mg (1.83 ± 0.22 vs 2.09 ± 0.28, P < .001) and albumin (4.15 ± 0.67 vs 4.33 ± 0.37, P = .07) were significantly lower in group 1 at admission. In addition, there was a correlation with hs-CRP and Mg levels (r = .27, P = .006; Figure 1). No statistically significant difference existed in serum creatinine, admission CKMB, potassium, sodium, hemoglobin, platelet, and white blood cell (WBC) count between the groups. Additionally, multivessel disease and stent implantation percentage, stent length, and diameters were similar between the groups. The existence of left anterior descending artery (LAD) lesion (65.9% vs 44.3%, P = .02) and reperfusion time (11.6 ± 9.9 vs 6.9 ± 5.7, P = .03) was significantly higher in group 1. Tirofiban usage (43.9% vs 81.4%, P < .001) and postprocedural thrombolysis in myocardial infarction 3 flow rate (82.9% vs 95.7%, P = .02) were significantly lower in group 1.
Baseline Characteristics.a
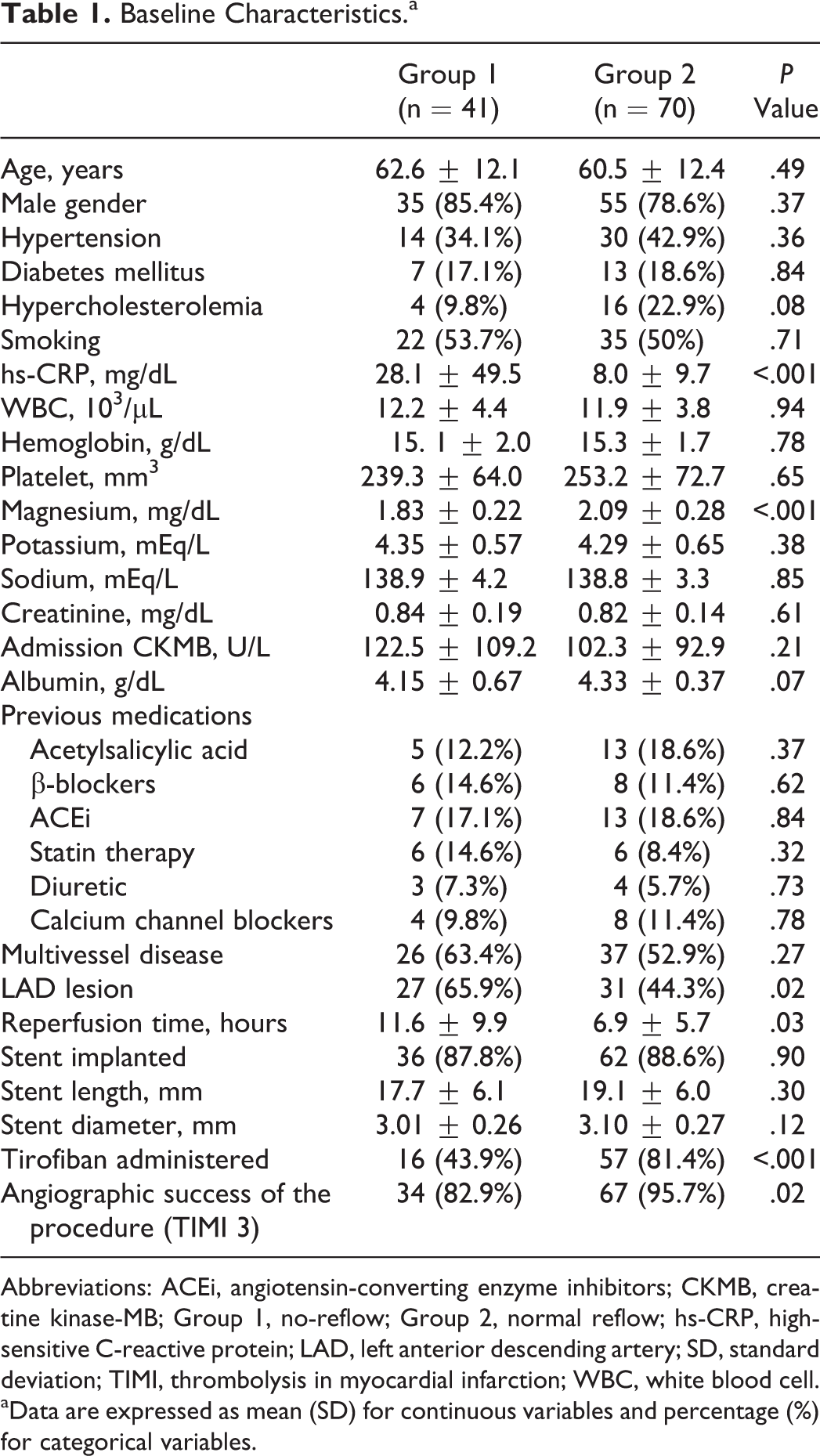
Abbreviations: ACEi, angiotensin-converting enzyme inhibitors; CKMB, creatine kinase-MB; Group 1, no-reflow; Group 2, normal reflow; hs-CRP, high-sensitive C-reactive protein; LAD, left anterior descending artery; SD, standard deviation; TIMI, thrombolysis in myocardial infarction; WBC, white blood cell.
aData are expressed as mean (SD) for continuous variables and percentage (%) for categorical variables.
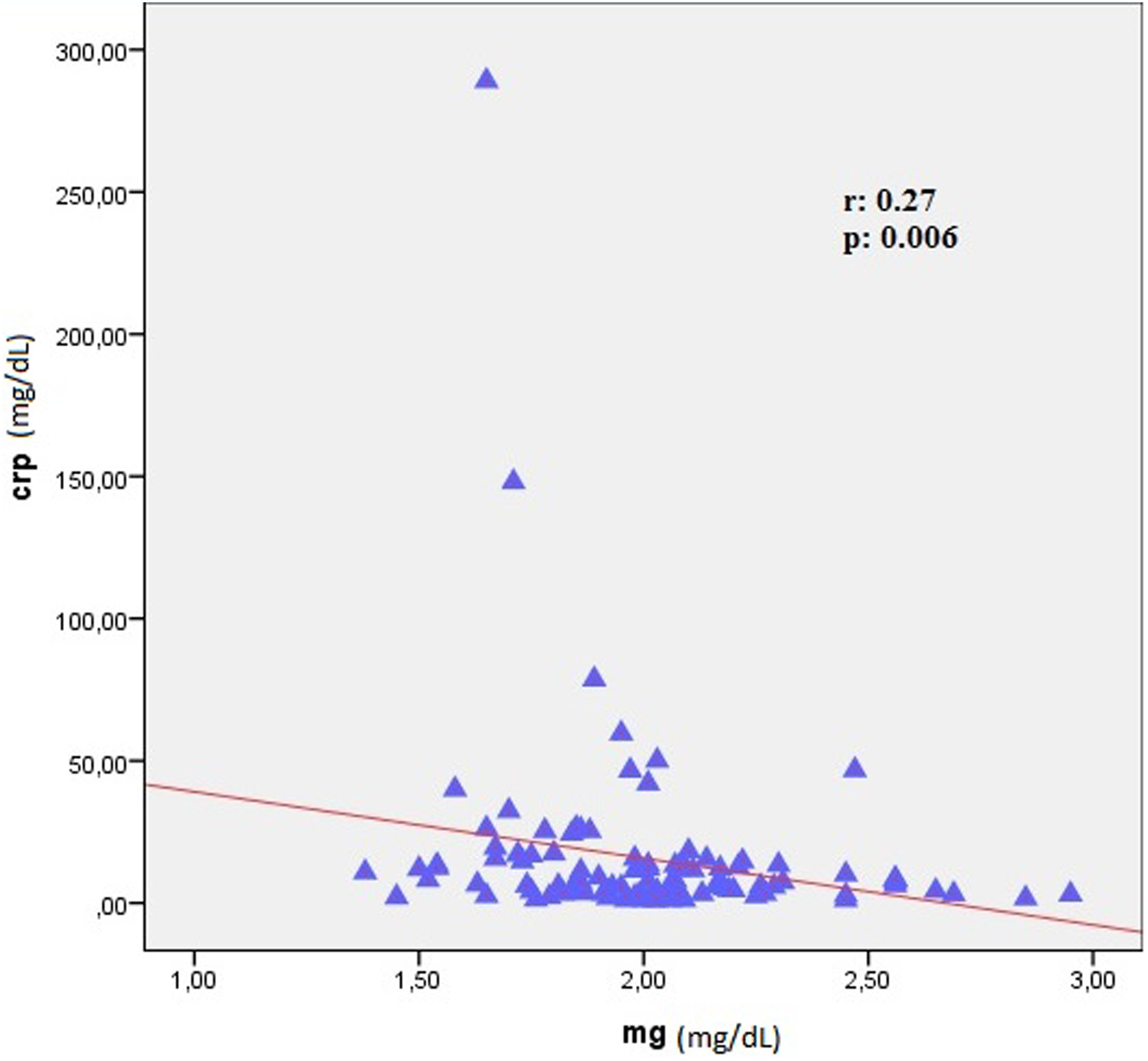
The correlation between high-sensitive C-reactive protein (hs-CRP) and magnesium (Mg) levels.
The variables for which the unadjusted P value was <.10 in univariate analysis were viewed as potential risk markers for the electrocardiographic no-reflow, and these variables were included in the full model. The presence of hyperlipidemia, LAD lesion, use of tirofiban, reperfusion time, Mg, albumin, and hs-CRP levels was analyzed with multivariate logistic regression model. In multivariate analyses, Mg (odds ratio [OR]: 0.01, <95% CI: 0.01-0.12; P = .004), hs-CRP (OR: 1.06, <95% CI: 1.00-1.14; P = .05), LAD lesion (OR: 6.66, <95% CI: 1.45-3.05; P = .01), and reperfusion time (OR: 1.01, <95% CI: 1.00-1.01; P = .03) were still independent predictors of electrocardiographic no-reflow (Table 2).
Effects of Multiple Variables on the No-Reflow in Univariate and Multivariate Logistic Regression Analyses.
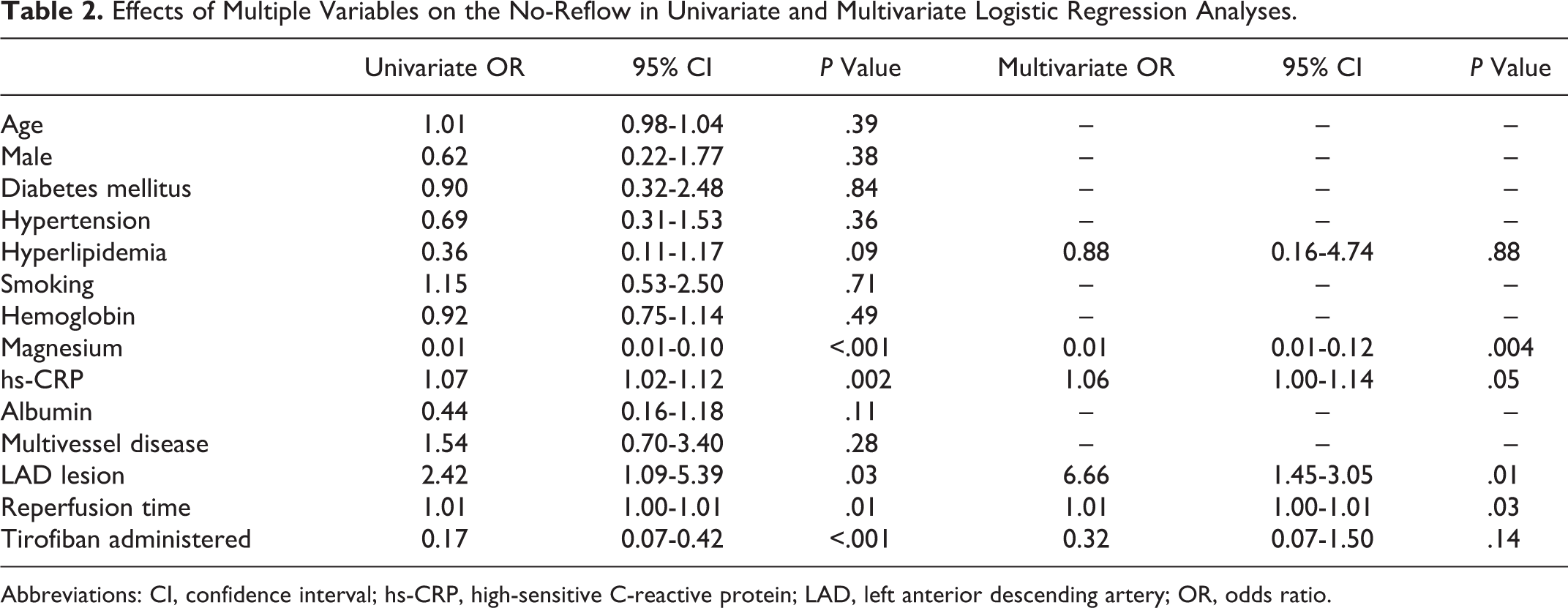
Abbreviations: CI, confidence interval; hs-CRP, high-sensitive C-reactive protein; LAD, left anterior descending artery; OR, odds ratio.
The ROC curves of Mg for predicting electrocardiographic no-reflow are shown in Figure 2. Magnesium <1.87 mg/dL measured on admission had 77% sensitivity and 59% specificity in predicting electrocardiographic no-reflow. When we divided the study population into 2 groups according to the 1.87 mg/dL Mg level cutoff value used in the ROC analysis, hs-CRP (25.4 ± 52.1 vs 10.7 ± 14.4, P = .003) and no-reflow (60.5% vs 24.7%, P < .001) were significantly higher in decreased Mg group. Although cardiovascular mortality, re-MI, and MACE were significantly more common in low Mg group, TVR rate was similar between the groups in the long-term follow-up (Table 3).
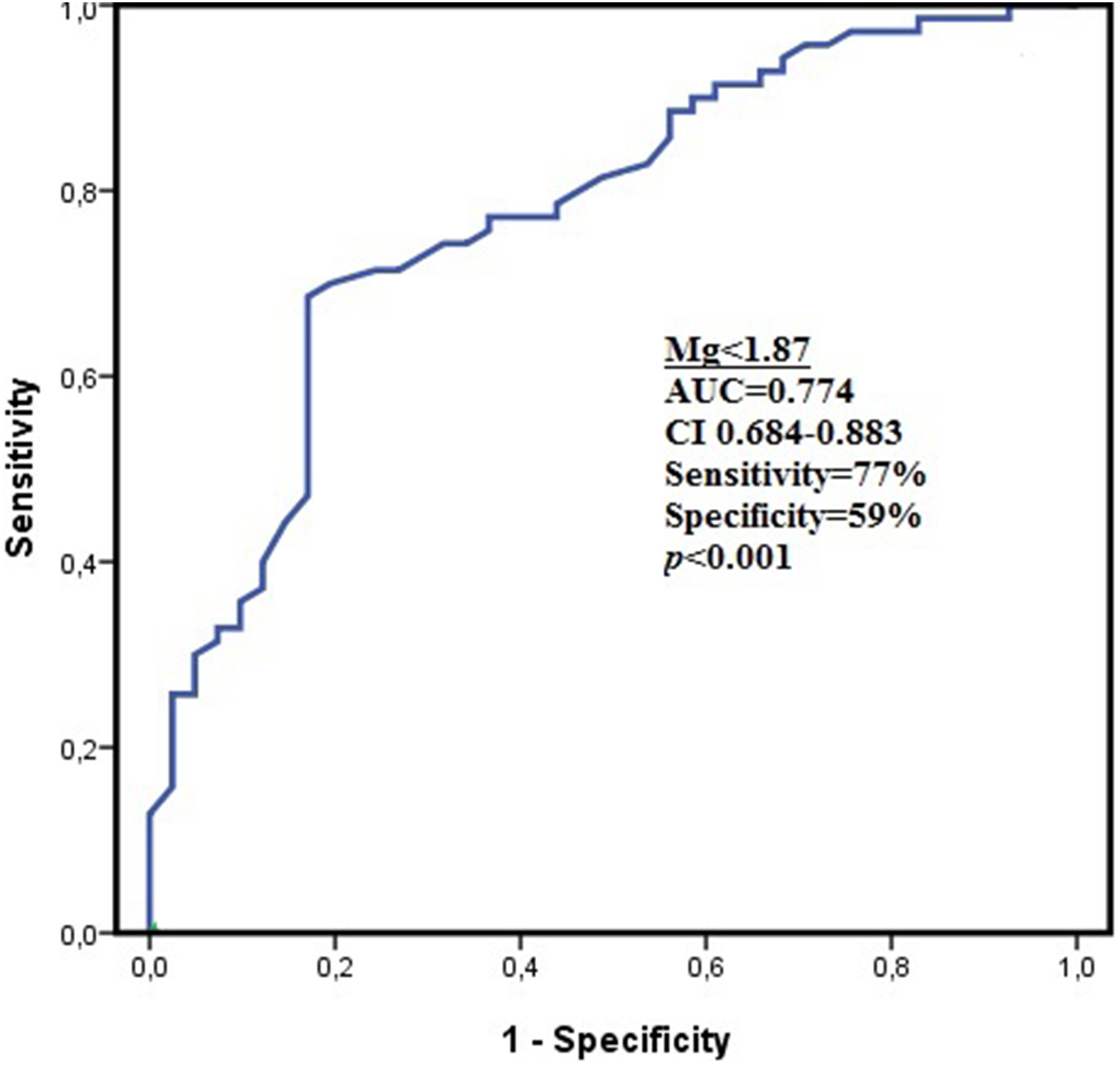
The receiver operating characteristic (ROC) curves of magnesium (Mg) for predicting electrocardiographic no-reflow.
Baseline Risk Factors Stratified by Magnesium Levels.a
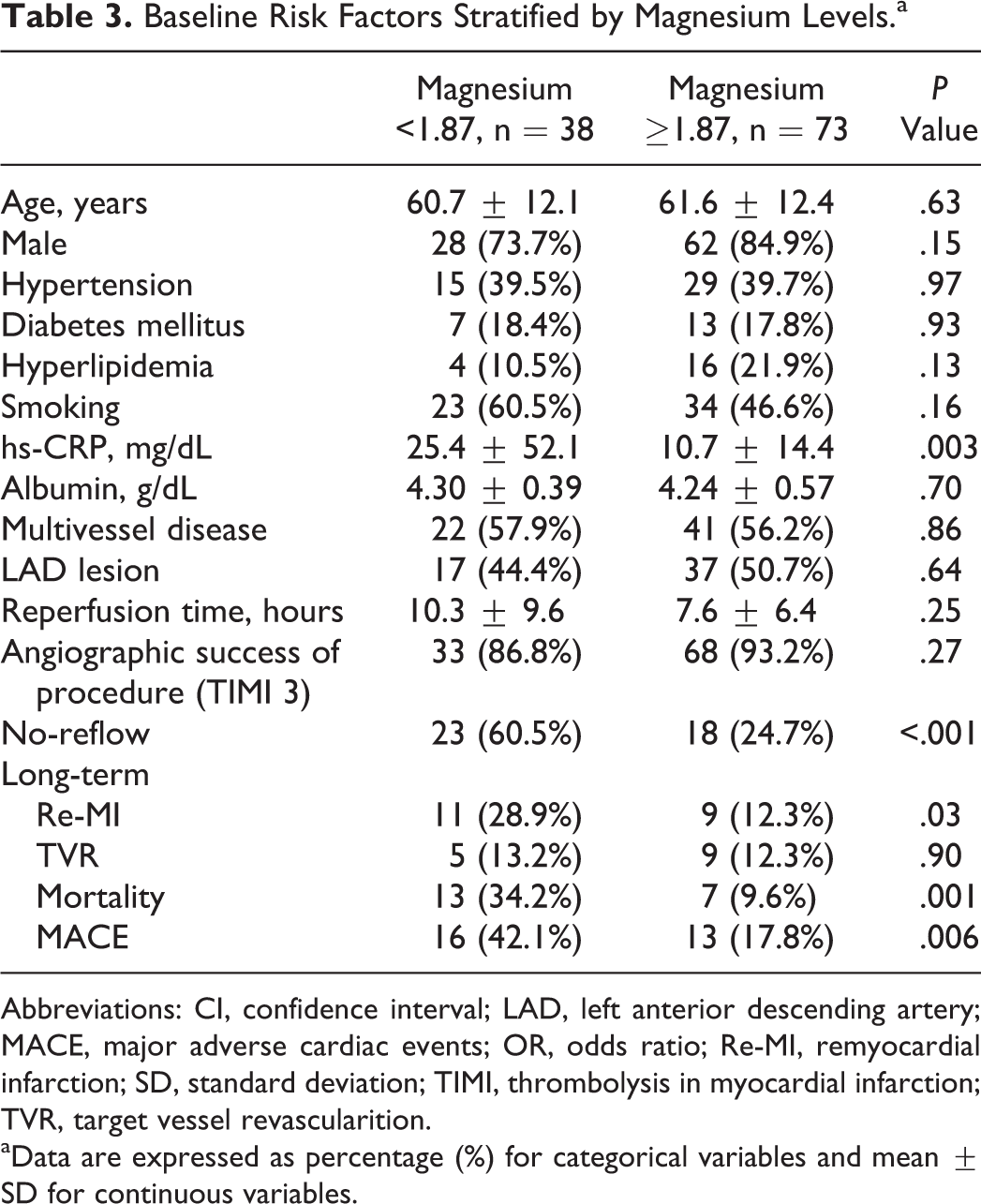
Abbreviations: CI, confidence interval; LAD, left anterior descending artery; MACE, major adverse cardiac events; OR, odds ratio; Re-MI, remyocardial infarction; SD, standard deviation; TIMI, thrombolysis in myocardial infarction; TVR, target vessel revascularition.
aData are expressed as percentage (%) for categorical variables and mean ± SD for continuous variables.
In the multivariate analyses for long-term mortality, age, gender status, DM, hemoglobin, Mg, presence of multivessel disease, LAD lesion, and no-reflow were investigated with multivariate logistic regression model. Only Mg (OR: 0.08, <95% CI: 0.01-1.03; P = .05) was still an independent predictor of long-term mortality (Table 4). Kaplan-Meier survival plots for cardiovascular mortality in Mg groups are presented in Figure 3.
Effects of Various Variables on Long-Term Mortality in Univariate and Multivariate Logistic Regression Analyses.
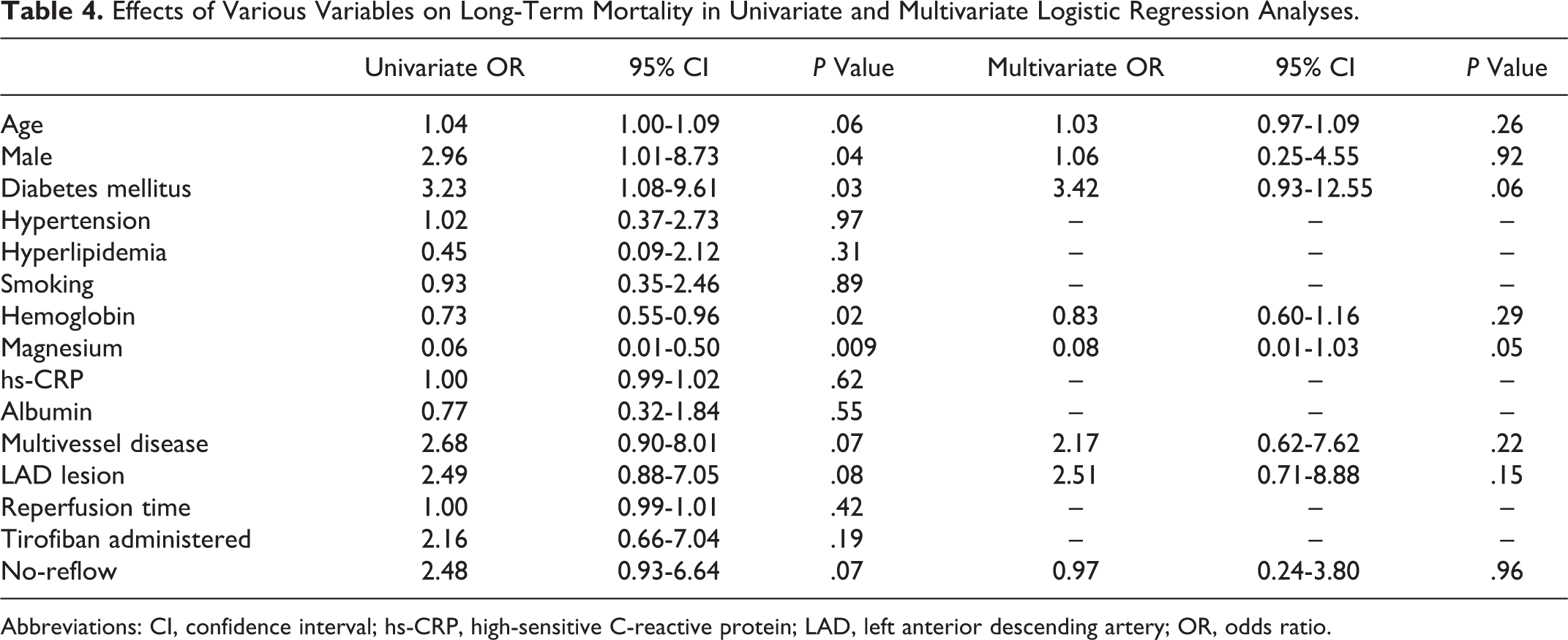
Abbreviations: CI, confidence interval; hs-CRP, high-sensitive C-reactive protein; LAD, left anterior descending artery; OR, odds ratio.
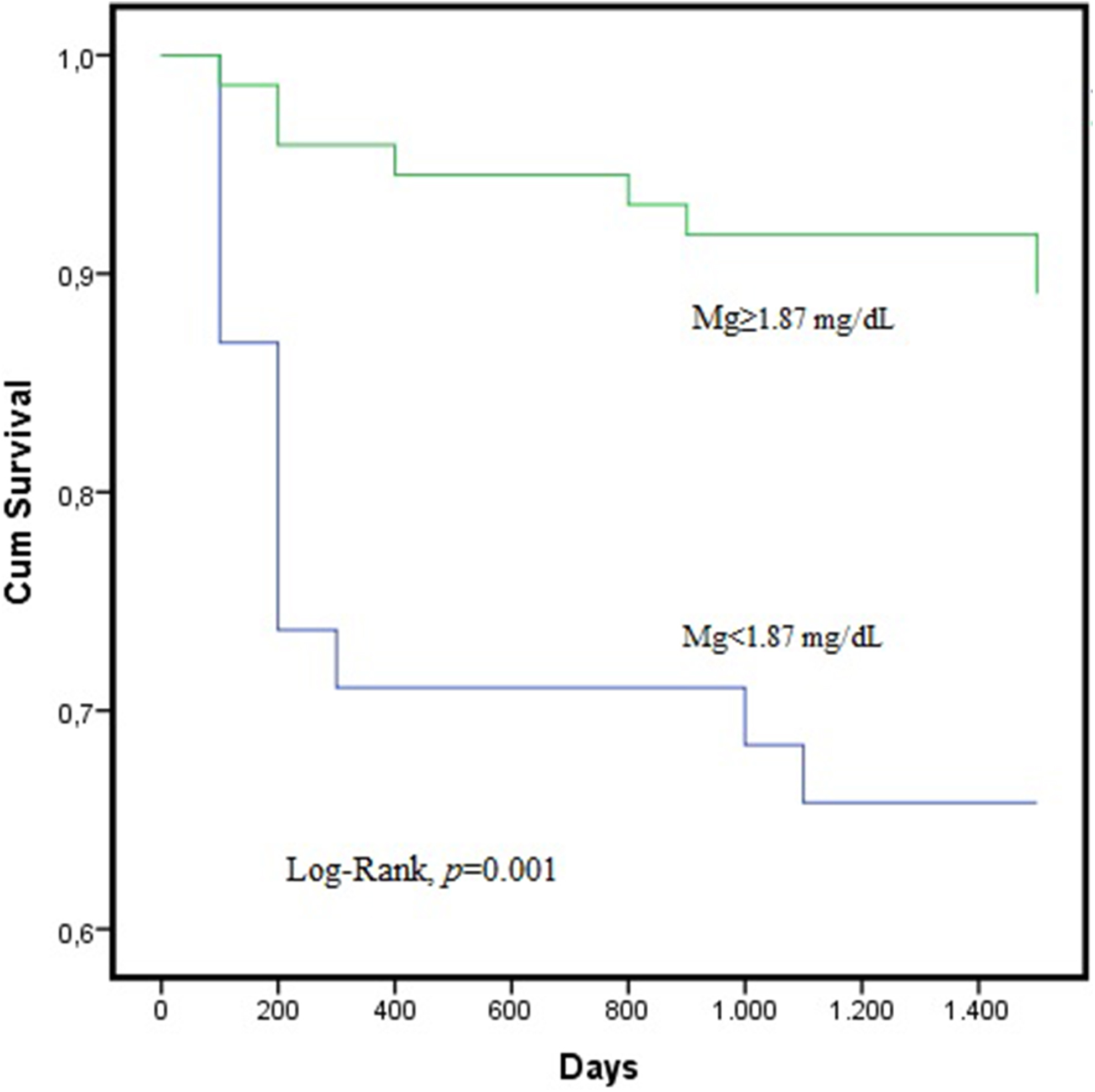
Kaplan-Meier survival plots for cardiovascular mortality in magnesium (Mg) groups.
Discussion
In this study, it was discovered for the first time, to our knowledge, that initial serum Mg level is an independent predictor for electrocardiographic no-reflow in patients with STEMI who underwent pPCI. In addition, it was demonstrated that initial Mg level is an independent predictor for long-term mortality in patients with STEMI who underwent pPCI.
Magnesium is commonly performed and measured in patients taken to general intensive care units. Also, it is commonly used in cardiopulmonary bypass surgery due to its cardioprotective effects during ischemia–reperfusion. 20 The routine use of Mg in acute myocardial infarction (AMI) is controversial. 21 Li et al published that early mortality was reduced in patients not treated with thrombolysis and in those treated with <75 mmol of Mg compared with the placebo groups. 22 Magnesium in Coronaries Trial study showed early administration of Mg in high-risk patients with STEMI has no effect on 30-day mortality. 23 Hypomagnesemia is a condition commonly associated with acute and chronic heart disease. Rasmussen et al showed that hypomagnesemia encountered during AMI is a result of Mg migration to the intracellular space from the extracellular space. 24 Studies show that low Mg is directly related to enable endothelial dysfunction by creating a proinflammatory, prothrombotic, and proatherogenic environment, which may lead to the pathogenesis of cardiovascular diseases. 25 It was identified that Mg prevents platelet activation by inhibiting platelet-stimulating factors such as thromboxane A2 (TXA2) or activating platelet inhibitory factors such as prostaglandin I2. 26,27
By reducing Ca mobilization in platelets, Mg shows its platelet inhibitory effect. Additionally, it limits fibrinogen interaction with platelets by competitive inhibition of Ca at the Ca-binding sites of the glycoprotein IIb/IIIa complex. 28 On the other hand, hypomagnesaemia is related to increased inflammation. The lack of Mg induces an inflammatory syndrome in animal models, shown by macrophage and WBC activation, release of proinflammatory cytokines, activation of an acute-phase response, and production of oxygen-free radicals more than necessary. 29,30 In our study, it was shown that Mg is correlated with hs-CRP. In addition, hs-CRP was statistically significant in patients having low-Mg level. It was demonstrated in the studies that hypomagnesemia is correlated with prognostic in acute cardiac events and chronic heart disease. 13,31 Cicek et al stated that hypomagnesemia is a predictor for stent thrombosis after pPCI. 31 Muir demonstrated that Mg has a neuroprotective effect in acute ischemic stroke. 32 In our study, we showed that hypomagnesemia is a predictor for long-term mortality.
No-reflow is an important complication common among patients with STEMI undergoing pPCI. It was found in studies that 5% to 50% of the patients undergoing pPCI due to STEMI developed no-reflow. 33 In our study, this rate is 36.9%, which is similar to the studies in the literature. Even if the responsible mechanism of no-reflow is not fully known, the most probable mechanisms are endothelial dysfunction, increased oxidative stress, and endothelial gap and bleb formation occurring due to increased reactivity of platelets with increased inflammation, platelet/leukocyte capillary plugging, and embolization of thrombus and/or plaque material spontaneously or during coronary intervention. 8 There are several studies indicating the relationship between no-reflow and increased inflammation and platelet reactivity. Abdi et al identified WBC count and thrombus grade as independent factors for no-flow after pPCI. Similar to our study, the correlation between no-reflow and duration of pain and hs-CRP levels was found. 7 Additionally, Hong et al showed that hs-CRP was an independent predictor of no-reflow in AMI. 34 To predict no-reflow incidence, Niccoli et al tried to evaluate the role of plasma levels of TXA2 while being admitted. It is clear TXA2 has an important mediator of platelet activation and aggregation and also a significant mediator of platelet-induced coronary vasoconstriction. 35 There are several studies examining the relationship between no-reflow and cardiovascular events. The correlation between no-reflow and long-term prognosis is still unclear. However, in the early period, the prognostic significance of no-reflow increases. 36 In our study, it was found that no-reflow was not an independent indicator of long-term mortality contrary to Mg. In addition, hypomagnesemia may not only increase mortality by triggering no-reflow but also contribute to mortality increase related to deteriorated regulation due to hypomagnesemia.
This study has some limitations. First, only a small number of patients participated in the study. On the other hand, the study population was homogeneous random patients with STEMI submitted to pPCI similar to real-world situations. Second, for finding myocardial perfusion, ∑STR was utilized. Using quantitative myocardial contrast echocardiography, more information on tissue perfusion can be obtained. Additionally, as optimal cineangiographic frame count setting (12.5 frames/second) did not exist, myocardial blush grade could not be evaluated. Through a blinded manual in a usual way, ∑STR measurements were provided. However, measurements through a digital ECG system with a high-resolution screen may yield more reliable results. Third, in this study, only hs-CRP in inflammatory parameters was investigated, whereas increased oxidative stress and platelet reactivity were not evaluated. Many studies indicating relationship between no-reflow and increased oxidative and thrombogenicity are present. 8,35
Conclusion
As a result, we believe that Mg levels in blood should be investigated in patients with STEMI admitted to the emergency services. Since no-reflow and long-term mortality rates are high in patients with STEMI having hypomagnesemia, more aggressive preventive methods could be adopted to block the development of no-reflow. This suggestion should be carefully supported and investigated with wider range prospective studies.
Footnotes
Authors’ Note
M.Y. and T.I. participated in its design and drafted the article. E.A., M.E.H., S.T., S.D., E.A., and S.S. participated in data collection. I.H.T. performed the statistical analysis. All authors approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.