
Abstract
Non-ST-segment elevation acute myocardial infarction (NSTEMI) is a life-threatening clinical emergency with a poor prognosis. However, there are no individualized nomogram models to identify patients at high risk of NSTEMI who may undergo death. The aim of this study was to develop a nomogram for in-hospital mortality in patients with NSTEMI to facilitate rapid risk stratification of patients. A total of 774 non-diabetic patients with NSTEMI were included in this study. Least Absolute Shrinkage and Selection Operator regression was used to initially screen potential predictors. Univariate and multivariate logistic regression (backward stepwise selection) analyses were performed to identify the optimal predictors for the prediction model. The corresponding nomogram was constructed based on those predictors. The receiver operating characteristic curve, GiViTI calibration plot, and decision curve analysis (DCA) were used to evaluate the performance of the nomogram. The nomogram model consisting of six predictors: age (OR = 1.10; 95% CI: 1.05-1.15), blood urea nitrogen (OR = 1.06; 95% CI: 1.00-1.12), albumin (OR = 0.93; 95% CI: 0.87-1.00), triglyceride (OR = 1.41; 95% CI: 1.09-2.00), D-dimer (OR = 1.39; 95% CI: 1.06-1.80), and aspirin (OR = 0.16; 95% CI: 0.06-0.42). The nomogram had good discrimination (area under the curve (AUC) = 0.89, 95% CI: 0.84-0.94), calibration, and clinical usefulness. In this study, we developed a nomogram model to predict in-hospital mortality in patients with NSTEMI based on common clinical indicators. The proposed nomogram has good performance, allowing rapid risk stratification of patients with NSTEMI.
Keywords
Introduction
Cardiovascular deaths have long been the leading cause of death globally. in 2021, cardiovascular diseases were responsible for an estimated 19.91 million deaths globally. 1 Non-ST-segment elevation acute myocardial infarction (NSTEMI) is one of the leading causes of hospitalization in patients with ischemic heart disease and is associated with a high mortality rate. 2 Data from the Beijing region of China showed that the hospitalization rate for NSTEMI per 100,000 population almost tripled from 2007 to 2012 (from 8.1% to 33.5%), with in-hospital mortality rates decreasing from 6.4 to 5.3% for men and from 11.6 to 8.7% for women. 3 A recent study showed that the 30-day mortality rate for NSTEMI in China was reported to be 4.7%, with the highest proportion of in-hospital deaths. 4 Treatment of NSTEMI consists mainly of pharmacologic and invasive therapies. 5 Antiplatelet drug therapy is usually performed in all patients, and the main drugs include aspirin and clopidogrel. Percutaneous coronary intervention is an effective treatment for NSTEMI in patients with ineffective pharmacologic therapy or at high risk for NSTEMI (eg, intractable angina, heart failure, ventricular tachycardia or ventricular fibrillation, and new onset of ST-segment depression). 5
Improving the prognosis of patients with NSTEMI and especially reducing in-hospital mortality is a long-term challenge for emergency physicians and cardiologists. Adherence to risk stratification of the disease and individualization of treatment are key to addressing this issue. The Thrombolysis in Myocardial Infarction and Global Registry of Acute Coronary Events risk scores were developed primarily in patients of Caucasian origin and are often used to assess adverse events and prognosis in NSTEMI.6,7 However, they have been reported to have limited applicability in non-White ethnicity.8,9 Yang et al first proposed a risk prediction model for in-hospital mortality in Chinese NSTEMI patients in 2018, which showed good predictive results, but systematic model validation was lacking, and it has not been widely studied since then. 10 Individualized risk assessment of patients to determine treatment regimens and overall management approaches is expected to result in lower mortality rates and better short- and long-term clinical outcomes. In recent years, the nomogram models have been widely used in disease diagnosis and risk stratification due to their visualization and simplicity. A well-performing nomogram can positively influence clinical decision-making and patient prognosis to a certain extent. Here we present a nomogram prediction model for hazard stratification of the risk of in-hospital death in patients with NSTEMI to help clinicians improve the prognosis of NSTEMI.
Methods
Data Source
Data for this retrospective study were obtained from a publicly available dataset (data available at https://peerj.com/articles/14346/), which was shared by Yao et al. 11 All authors have waived their copyright to the original research data. For scientific research purposes, we used these data for secondary analysis.
Study Population
A total of 774 non-diabetic patients diagnosed with NSTEMI were included in this study, including 734 patients who survived to discharge and 40 who died during their hospitalization. The Ethics Committee of Zhongda Hospital affiliated to Southeast University (2020ZDSYLL164-P01) approved the original study.
Data Collection
We included a set of variables based on literature review and their availability in the original dataset. These variables include age, sex, hypertension, chronic kidney disease (CKD), smoking, alcohol, systolic blood pressure (SBP), diastolic blood pressure (DBP), Pulse, white blood cells (WBC), neutrophils, lymphocytes, monocytes, platelet (PLT), hemoglobin (Hb), D-dimer, alanine aminotransferase (ALT), aspartate aminotransferase (AST); albumin (ALB), lactate dehydrogenase (LDH), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol, triglyceride (TG), total cholesterol (TC), blood urea nitrogen (BUN), uric acid (UA), creatinine, cardiac troponin I (cTnI), left ventricular ejected fraction (LVEF), antihypertensive drug, lipid-lowering drug, aspirin, diuretics and β-blockers.
Statistical Analyses
The distributions of all quantitative variables were analyzed using the Shapiro-Wilk test. Normally distributed continuous data were presented as the mean ± standard deviation and were compared between the two groups using the independent samples t-test. Non-normally distributed continuous data were presented as median (interquartile range) and compared using the Mann-Whitney test. Categorical variables were presented as counts and percentages, and differences between two groups were compared by the chi-squared test or the Fisher exact test.
Figure 1 illustrated the flowchart of this study. All the 774 patients were analyzed for variable selection to develop the risk prediction model. Least Absolute Shrinkage and Selection Operator (LASSO) regression was applied to select the potential predictors from 34 candidate variables. Univariate logistic regression and multivariate backward stepwise logistic regression were performed to identify the predictors for in-hospital mortality in patients with NSTEMI, and the Akaike Information Criterion (AIC) was used to construct the best prediction model. A nomogram was developed based on the results of the best prediction model, which was validated internally using the bootstrap method. The receiver operating characteristic (ROC) curve, GiViTI calibration plot, and decision curve analysis (DCA) were used to evaluate the performance of the nomogram. All of the statistical analyses were performed using R software (4.2.2). A P-value < .05 (two-tailed) or the 95% confidence interval (CI) of the odds ratio excluding the value one was considered statistically significant.
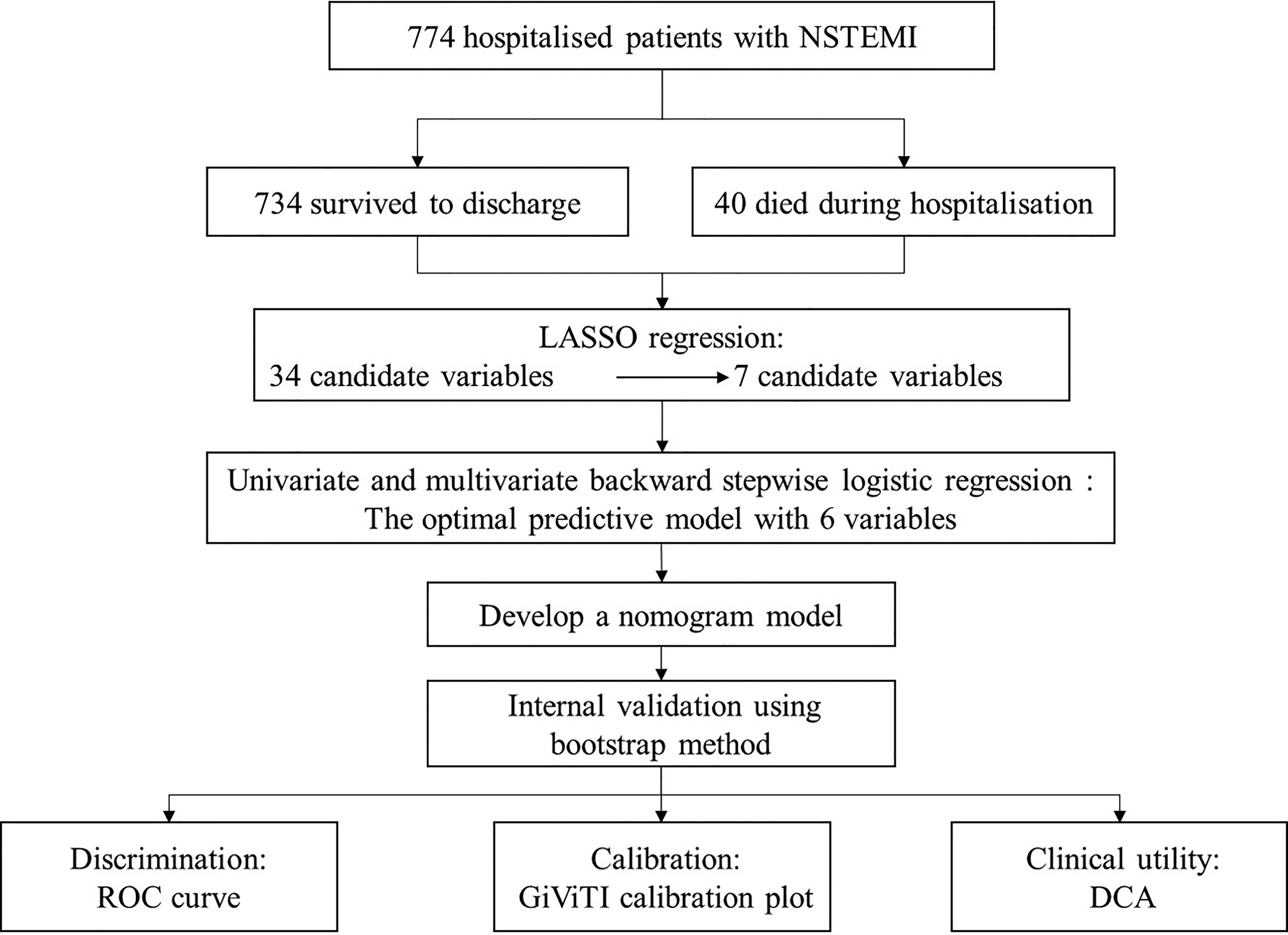
Research flow chart.
Results
Baseline Characteristics
A total of 774 eligible patients were enrolled in this study, 734 of them survived to discharge and 40 died during their hospitalization. The baseline characteristics of the included participants are presented in Table 1. NSTEMI patients who die in-hospital tend to be older, more likely to have comorbid CKD, have lower SBP and DBP, faster pulse rates, and lower LVEF than those who survive to discharge (all P < .05). In terms of laboratory tests, NSTEMI patients who died in-hospital had higher WBC counts, neutrophil counts, D-dimer, LDH, BUN, and creatinine, and lower lymphocyte counts, Hb, ALB, LDL-C, and TC (all P < .05). In terms of medication use, patients who died in the hospital had significantly lower rates of use of antihypertensive drugs, lipid-lowering drugs, aspirin, diuretics, and β-blockers than those who survived (all P < .05).
Baseline Characteristics of Patients with NSTEMI.
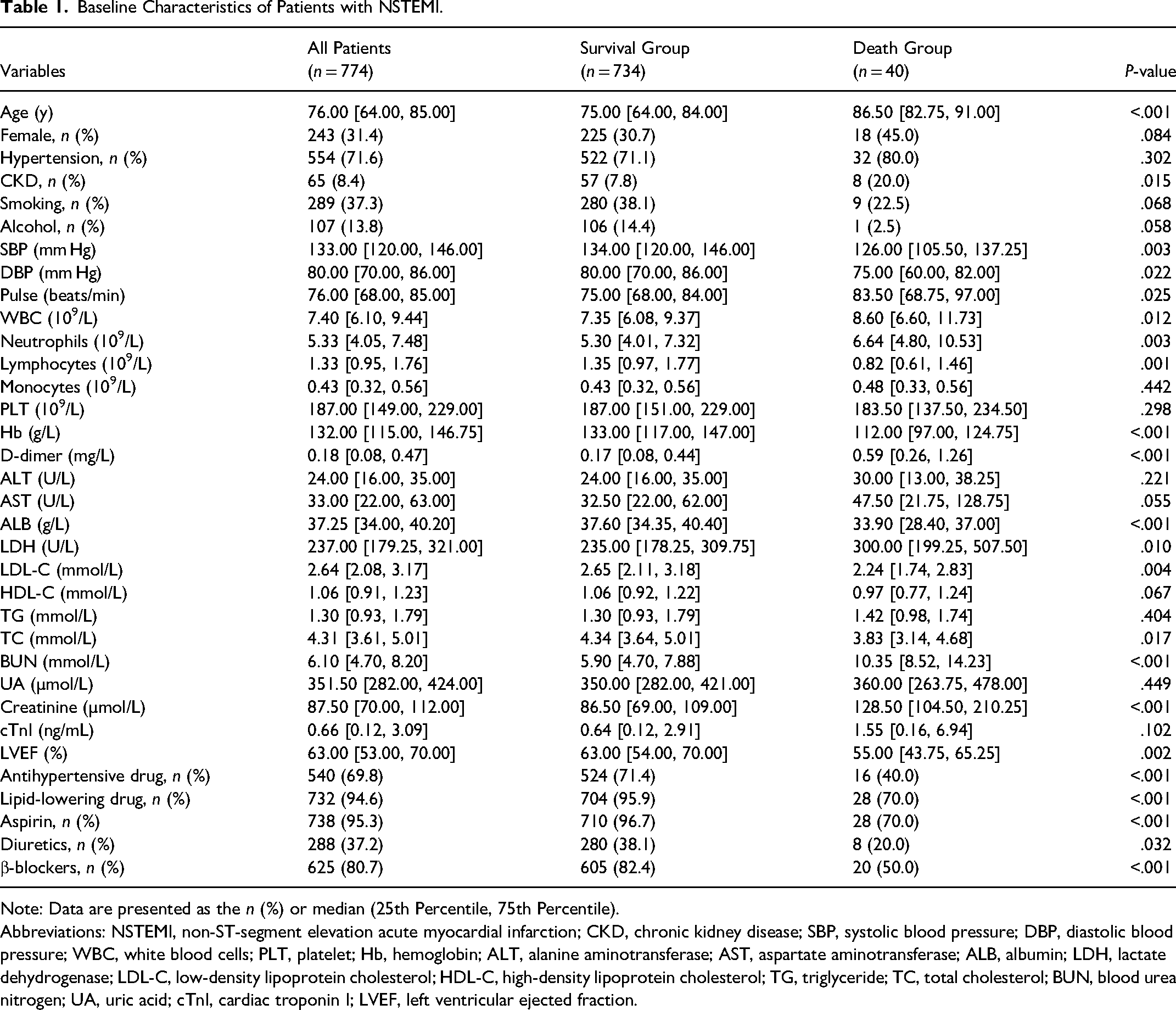
Note: Data are presented as the n (%) or median (25th Percentile, 75th Percentile).
Abbreviations: NSTEMI, non-ST-segment elevation acute myocardial infarction; CKD, chronic kidney disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; WBC, white blood cells; PLT, platelet; Hb, hemoglobin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALB, albumin; LDH, lactate dehydrogenase; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; TC, total cholesterol; BUN, blood urea nitrogen; UA, uric acid; cTnI, cardiac troponin I; LVEF, left ventricular ejected fraction.
Variable Selection Based on the LASSO Regression
LASSO regression was used to initially screen the predictors. The LASSO regression included 34 candidate variables (all variables in Tables 1), and based on the result of the LASSO regression analysis, we screened the following seven variables with non-zero coefficients as predictors: age, BUN, ALB, TG, D-dimer, Aspirin and Lipid-lowering drug (Figure 2).
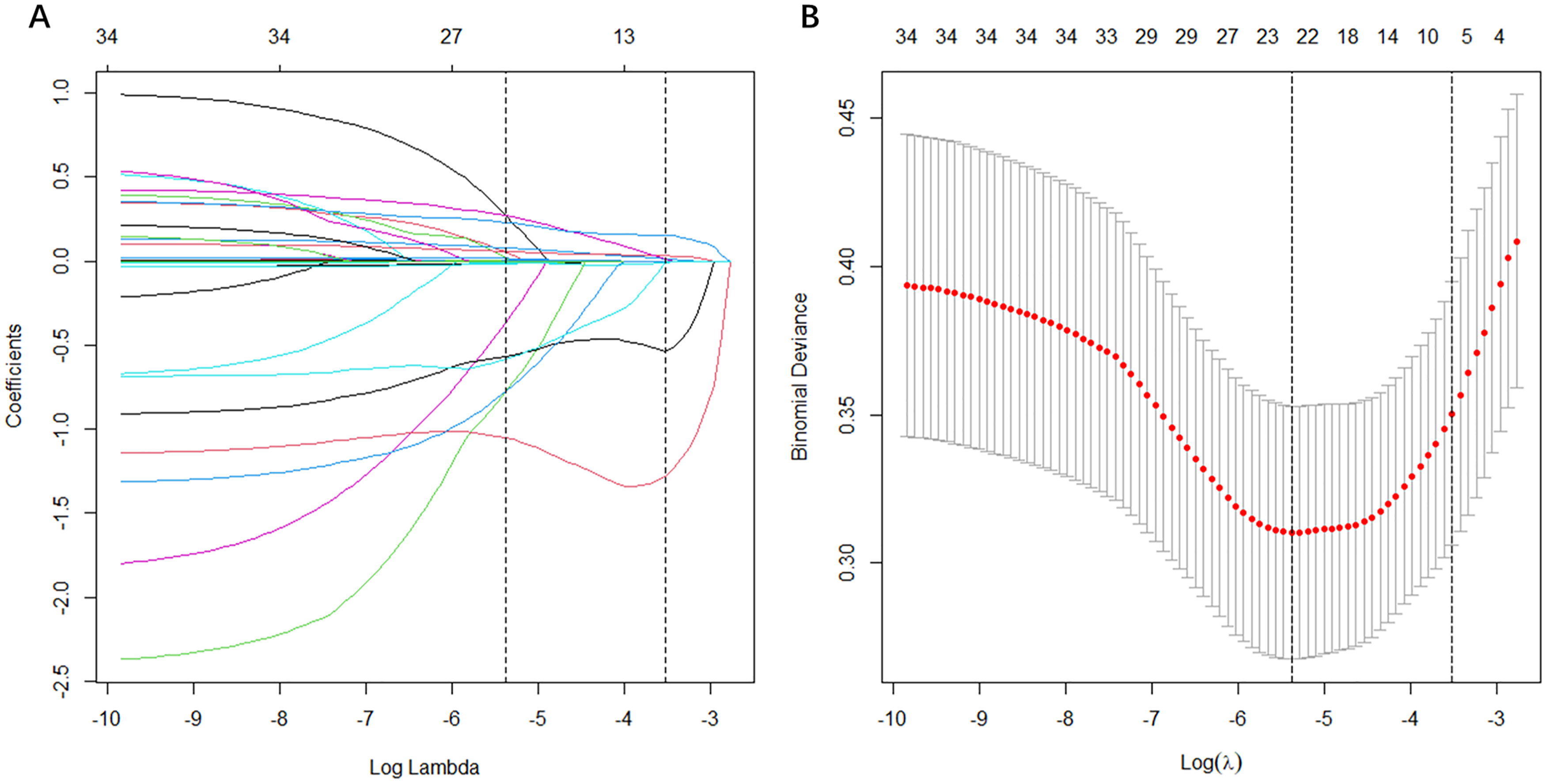
Feature selection using the least absolute shrinkage and selection operator (LASSO) binary logistic regression model. (A) LASSO coefficient profiles of the 34 baseline features; (B) The tuning parameter (λ) selection in the LASSO model using 10-fold cross-validation via minimum criteria. Vertical lines were drawn at the value selected using 10-fold cross-validation, where optimal λ resulted in 7 non-zero coefficients.
Univariate and Multivariate Logistic Regression Analysis
As shown in Table 2, seven variables screened by LASSO regression were included in the univariate logistic regression analysis and those variables that were statistically significant (P < .05) in the univariate analysis were subsequently included in the multivariate logistic regression model in a backward stepwise fashion.
Univariate and multivariate logistic regression analyses.
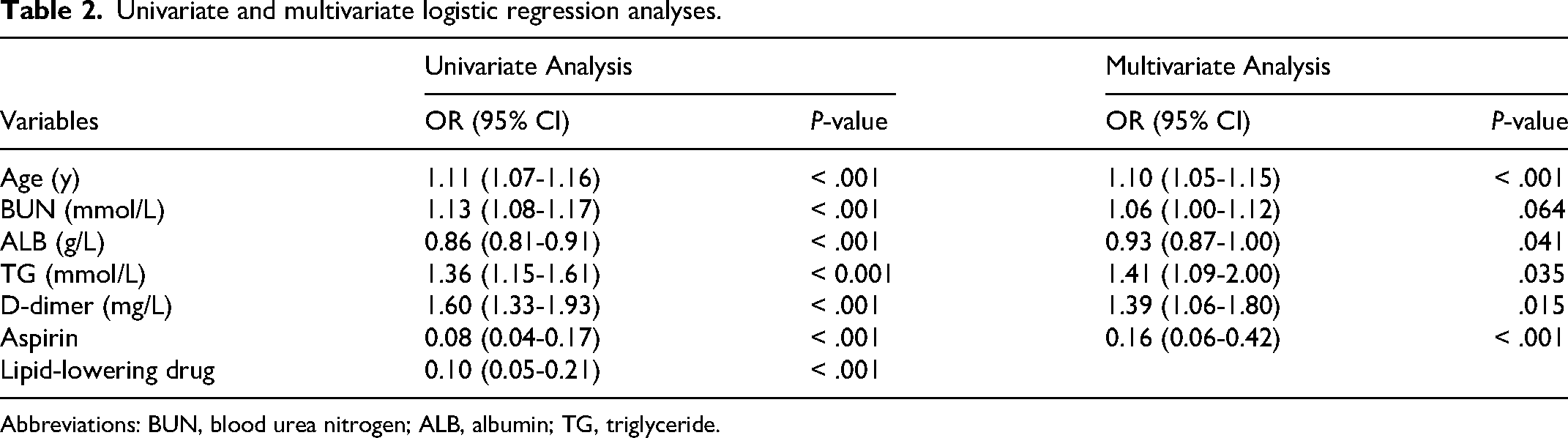
Abbreviations: BUN, blood urea nitrogen; ALB, albumin; TG, triglyceride.
Finally, an optimal predictive model consisting of six variables (age, BUN, ALB, TG, D-dimer and Aspirin) was determined according to the AIC.
Development and Validation of a Mortality-Predicting Nomogram
As shown in Figure 3, a simple nomogram was formulated on the results of multivariate analysis to facilitate the calculation of risk scores and thus easily assess the probability of an individual's in-hospital mortality.
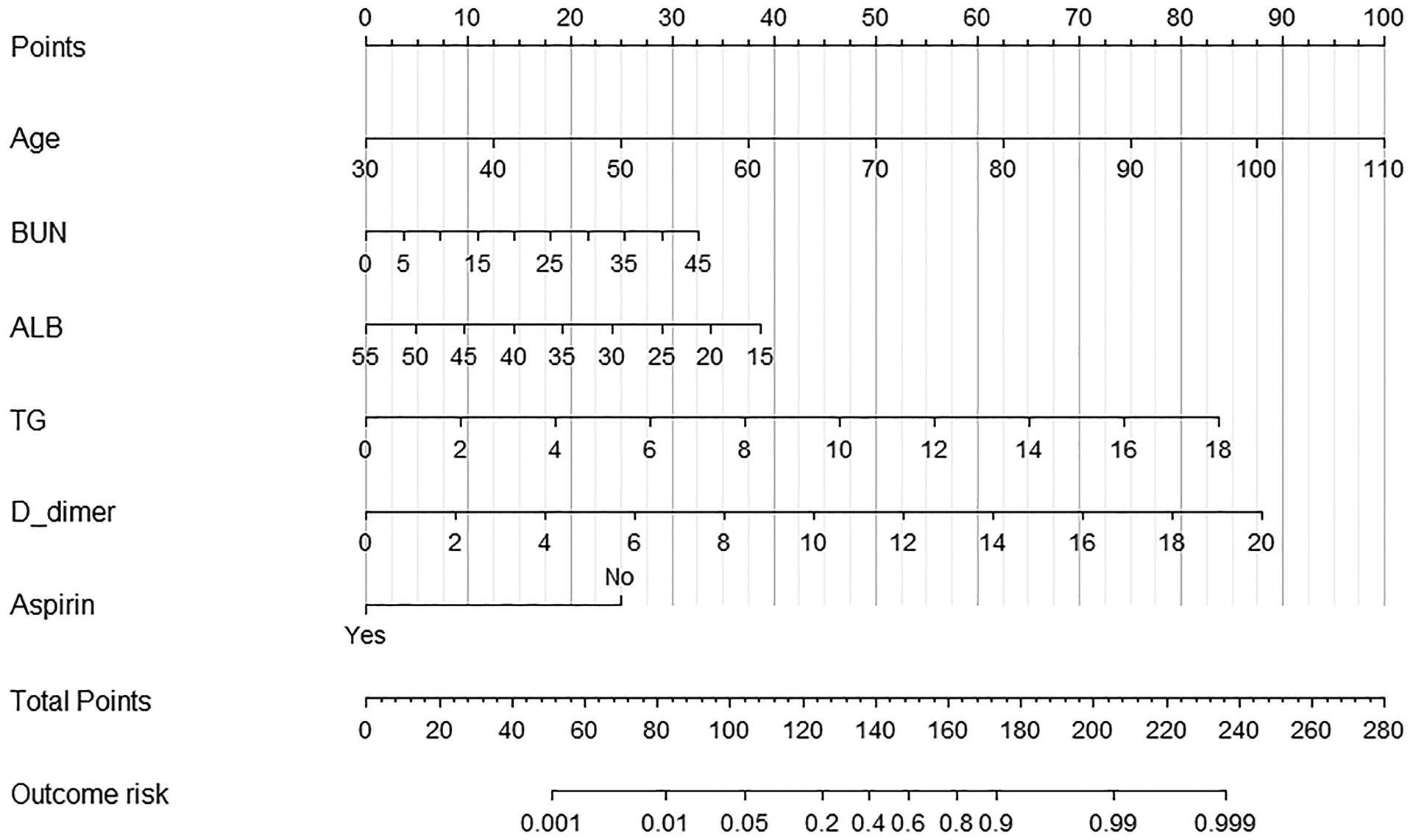
The nomogram for the prediction of in-hospital mortality in patients with NSTEMI.
Each of these independent predictors was projected upwards onto the ‘point’ of that value at the top of the nomogram to obtain a score from 0 to 100, and the total score of these points were then recorded to predict the probability of NSTEMI patients in-hospital mortality risk.
We evaluated the performance of the nomogram in the internal validation. ROC analysis showed that the developed nomogram model had good discriminatory power with a specificity of 86% and a sensitivity of 80%, corresponding to an area under the curve (AUC) of 0.89 (95% CI: 0.84-0.94) (Figure 4).
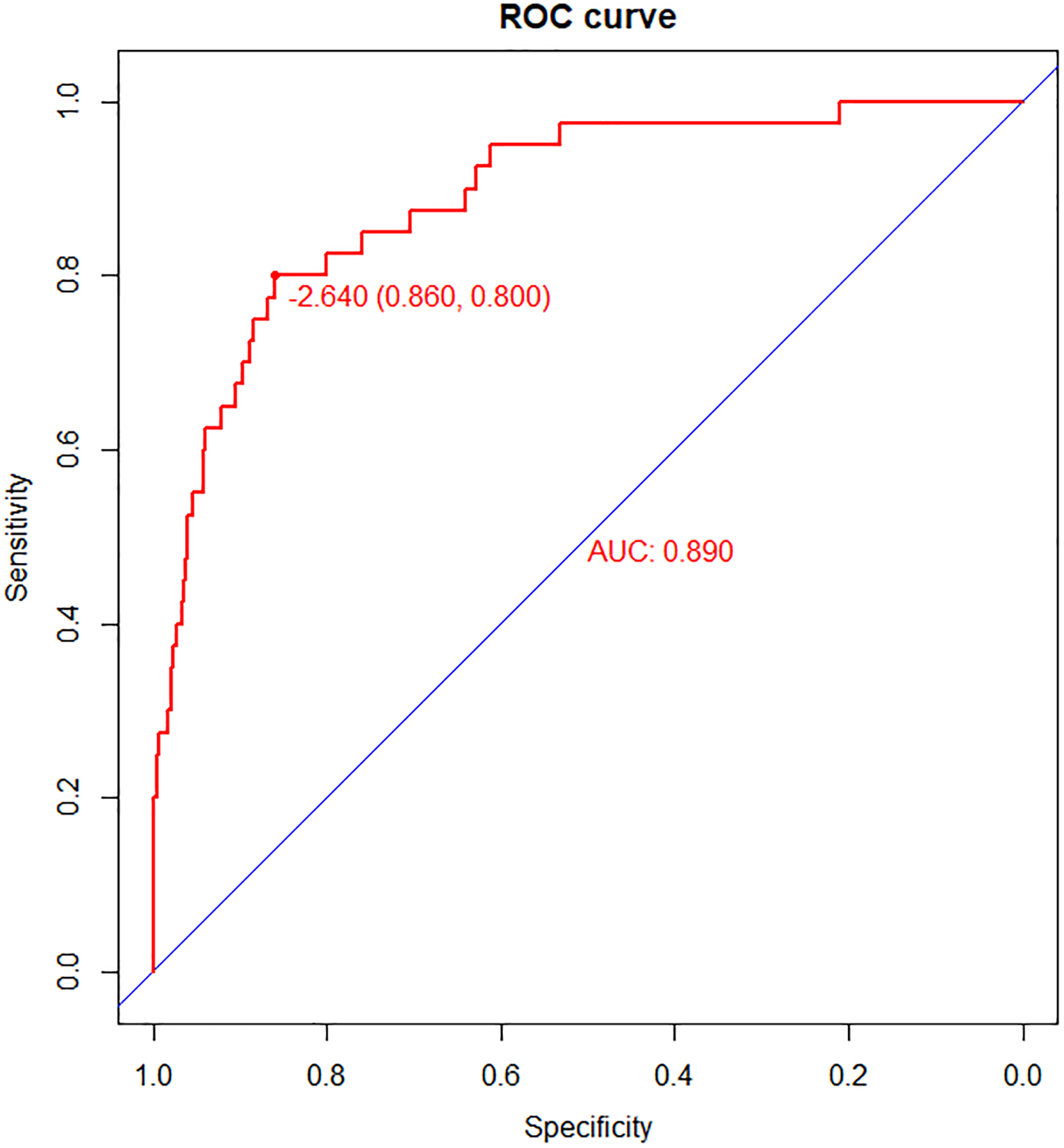
The receiver operating characteristic (ROC) curve of the nomogram.
The 80% and 95% CI regions of the GiViTI calibration bands did not cover the 45 degree diagonal divider (P = .645), indicating the consistency of the model's predicted probabilities with the actual probabilities and the high reliability of the prediction model (Figure 5A).
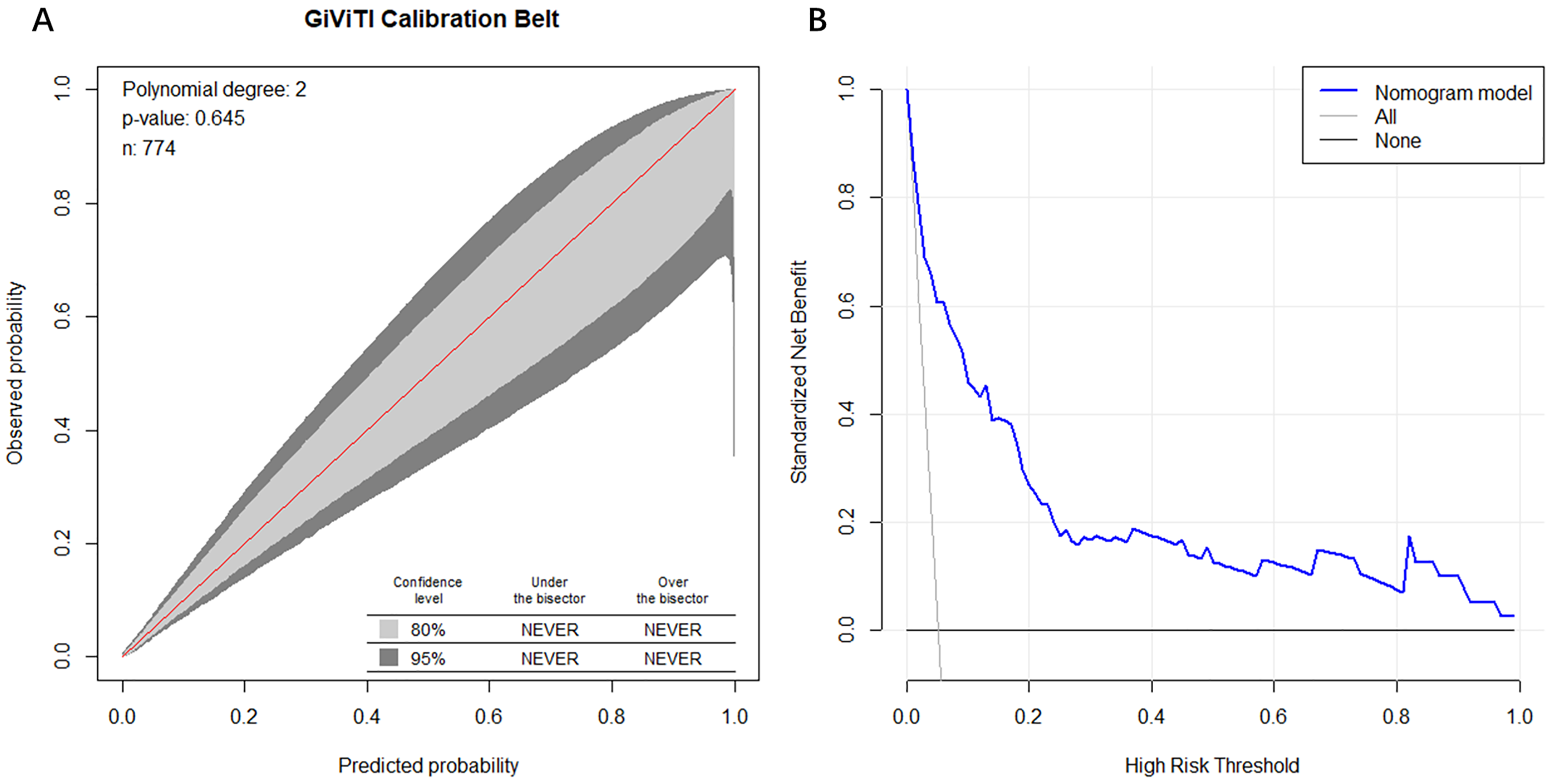
(A) The GiViTI calibration plot of nomogram model; (B) the clinical decision curve analysis (DCA) of nomogram model.
The DCA showed the clinical utility of the nomogram to predict in-hospital mortality of patients with NSTEMI (Figure 5B). A horizontal line represents the intervention-none and the net benefit with zero, the oblique line shows intervention-all-patients. As can be seen from the results of the DCA, the nomogram provided substantial net benefits over this broad range of threshold probability ranged from 5% to 100%, suggesting that the model we developed provided sound clinical guidance.
Discussion
NSTEMI is a common cardiac emergency with a poor prognosis. However, previous studies on cardiovascular disease risk assessment and prognosis have focused mostly on ST-segment elevation myocardial infarction (STEMI), and NSTEMI has been relatively understudied. Recent epidemiological studies have shown a decreasing trend in the relative incidence of STEMI and a gradual increase in the incidence of NSTEMI.3,12 Conducting relevant research on NSTEMI could help improve prognosis and reduce the economic burden. Our aim of this study was to provide early risk stratification of the risk of death during hospitalization in patients with NSTEMI in the expectation of individualized therapeutic management to reduce in-hospital mortality.
In this study, the in-hospital mortality rate for non-diabetic patients with NSTEMI was 5.2% (40/774), which is similar to previously published studies (5.3-6.3%).3,13,14 We developed a novel nomogram model based on 6 clinical parameters (age, BUN, ALB, TG, D-dimer and Aspirin) for assessing the risk of in-hospital mortality in patients with NSTEMI. The nomogram yielded satisfactory discrimination power, with AUC value of 0.89 (95% CI: 0.84-0.94). The GiViTI calibration plot demonstrated the good calibration of the nomogram and the DCA showed that the nomogram has good practical value.
It is well known that advanced age is both an important risk factor for heart disease and an influential factor in poor prognosis. In this study, we found that advanced age was an independent predictor of in-hospital mortality in patients with NSTEMI.
BUN is a protein metabolic product generated mainly in the liver and excreted through the kidney, and traditionally, the level of serum BUN is an indicator of renal function.
BUN has been shown to be independently associated with prognosis in patients with acute myocardial infarction (AMI). A retrospective analysis of 2995 AMI patients by Horiuchi et al found that a high level of BUN was independently and positively associated with the risk of in-hospital mortality in patients. 15 Another study showed that elevated BUN on admission was an independent predictor of long-term mortality in patients with STEMI. 16 Consistent with these studies, we found that a higher level of BUN was associated with higher in-hospital mortality in patients with NSTEMI.
Several previous studies have shown that low serum ALB is associated with poor in-hospital outcomes and long-term prognosis in patients with coronary artery disease (CAD).17–19 Similar results were obtained in the present study, where we found that for every 1 g/L decrease in serum ALB, there was a corresponding 7% increase in the risk of in-hospital death in patients with NSTEMI. This may be related to the fact that ALB is a negative acute phase reactant, whose synthesis decreases and catabolism increases in some cases of inflammation-related diseases such as AMI. 20
A study from China that included 5836 AMI patients identified D-dimer as a strong predictor of in-hospital death, 21 which is consistent with our findings. Interestingly, however, the analysis of another study that included 234 Turkish patients hospitalized with NSTEMI showed that D-dimer had no significant value in predicting the risk of death. 22 We hypothesize that this opposite finding may be due to the small relative sample size of the latter.
The results of existing studies on the effect of serum TG levels on cardiovascular prognosis are inconsistent. In a cohort study of 1836 Japanese patients with CAD undergoing complete revascularisation, Kasai et al found that elevated fasting TG level is associated with increased risk of cardiac death. 23 Similarly, we found that TG was strongly associated with in-hospital death, with a 41% increase in the risk of in-hospital death per 1 mmol/L increase in TG. However, other studies have suggested that lower TG on admission is associated with a poorer short- and long-term prognosis in patients with CAD.24,25 High TG level is generally recognized as a risk factor for cardiovascular disease, yet it is associated with a poor cardiovascular prognosis, a phenomenon Xia et al refer to as a “TG paradox” and suggest that this may be because high TG levels indicate a better overall nutritional status, and thus a better prognosis for the patient. 26
Aspirin has a wide application worldwide as a basic drug in the treatment of NSTEMI. As shown in Table 1, in our study, a significantly lower proportion of NSTEMI patients who died in-hospital used aspirin compared to those who survived to discharge (70% vs 96.7%, P < .001). There was no indication in the original study as to why individual patients did not use aspirin, and we speculate that this may be related to the risk of bleeding. Our study showed that aspirin use significantly reduced in-hospital mortality.
In this study, we developed a nomogram model for predicting in-hospital mortality in patients with NSTEMI. The nomogram showed good predictive performance and clinical utility. The predictors in the nomogram are readily available, which greatly extends its applicability and allows physicians to use the model to quickly and accurately determine the risk of in-hospital death in patients with NSTEMI and provide timely treatment to reduce mortality.
This study also has some limitations. Firstly, although the prediction model developed in this study was internally validated and performed well, it lacked external validation. Secondly, prospective studies and larger sample sizes are needed to validate the results. Finally, this was a retrospective and observational study and although we performed a multivariate analysis to eliminate confounding factors, there may still be bias due to unknown confounders.
Conclusions
In this study, we developed a nomogram model for predicting in-hospital mortality in patients with NSTEMI based on common clinical indicators. The prediction model was validated to have good discrimination, calibration and clinical utility. The model allows for rapid risk stratification of NSTEMI patients and provides a basis for individualized treatment.
limitations of the study. The present study was a secondary analysis based on the original study, which inevitably had some limitations due to the availability of primary data, such as our inability to obtain exhaustive patient history, in-hospital complications, electrocardiograms, coronary angiograms, and catheterization information. Therefore, larger prospective cohort studies are needed to confirm the findings of this study before the results can be generalized.
Footnotes
Acknowledgments
The authors thank Dr Yao from Zhongda Hospital affiliated to Southeast University for sharing the data.
Author Contributions
Wei Hu designed the study. Panpan Li wrote the manuscript, which was revised and statistically supervised by Wensen Yao. Jingjing Wu, Yating Gao, and Xueyuan Zhang participated in the analysis of the data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The Ethics Committee of Zhongda Hospital affiliated to Southeast University (2020ZDSYLL164-P01) approved the original study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Xiaogan Natural Science Program (XGKJ2020010005); Hubei Provincial Health Commission Joint Fund (WJ2018H0094); Hubei Provincial Key Laboratory of Occupational Hazard Identification and Control (JF2023-G10).