
Abstract
We aimed to investigate the association of aspirin and/or clopidogrel low response with −455G/A polymorphism of β-fibrinogen in patients with acute coronary syndrome (ACS). We enrolled 114 consecutive patients (mean age 61 ± 7, 31 female [27.2%], 83 male [72.8%]) with a first ACS. The diagnostic criteria for ACS were based on current guidelines. The -455 G/A β-fibrinogen polymorphism genotype distribution in the patient group was determined as the following: 54.4% GG homozygote, 39.5% GA, and 6.1% AA homozygote. Clopidogrel low response was present in 25 (21.9%) patients, aspirin low response in 21 (18.4%) patients, and dual antiplatelet low response in 9 (7.9%) patients. In our study, no difference was observed in terms of the distribution of -455 G/A β-fibrinogen polymorphism between the groups with and without aspirin and/or clopidogrel or dual antiplatelet low response in the patient group who underwent aspirin and clopidogrel treatment for ACS (P > .05).
Introduction
Platelet activation plays a crucial role in the pathogenesis of coronary artery disease (CAD). 1,2 The activation and aggregation of platelets are involved in the process of intracoronary thrombus proliferation, following atherosclerotic plaque rupture and/or mechanical disruption in the coronary artery due to percutaneous coronary intervention (PCI). 3 Dual antiplatelet agent treatment with aspirin and clopidogrel is the standard therapy in CAD. 1 Previous data strongly supported antiplatelet low response to aspirin and/or clopidogrel bearing a significantly high risk of cardiovascular complications related to stent thrombosis. 4 –7 A meta-analysis by the Antithrombotic Trialists’ Collaboration revealed a 25% decrease in recurrent serious vascular events in patients with high-risk CAD with antiplatelet therapies. 1 However, the antiplatelet effects of the treatments are not observed in all patients, and some patients experience thromboembolic events despite regular antiplatelet treatments. Those patients are clinically designated as aspirin or clopidogrel resistant or nonresponders. A number of studies have shown that aspirin or clopidogrel low response, proven by laboratory testing, is associated with increased risk of recurrent cardiovascular events. 8,9
Fibrinogen levels are strongly correlated with traditional vascular risk factors, including age, physical inactivity, hypertension, smoking, and features of the insulin resistance syndrome. Furthermore, fibrinogen is an acute-phase reactant, and the acute-phase response is strongly implicated in the development of arterial disease. 10 Several polymorphisms have been identified in the genes encoding the 3 pairs of fibrinogen polypeptide chains (α, β, and γ). Of the β-chain polymorphisms, the −455G/A has been the most extensively studied clinically. Nevertheless, the relation between the −455G/A variant and the risk of arterial thrombotic disease is controversial; only limited case–control studies have been performed. 11,12 However, according to our knowledge there is no sufficient number of studies evaluating the association between fibrinogen gene polymorphism and antiplatelet low response. Therefore, we aimed to investigate the association of aspirin and/or clopidogrel low response with −455G/A polymorphism of β-fibrinogen in patients with acute coronary syndrome (ACS).
Methods
Patients
A total of 114 consecutive patients (mean age 61 ± 7, 31 female [27.2%], 83 male [72.8%]) with a first ACS were recruited to the study between January 2009 and February 2011. The diagnostic criteria for ACS were based on the current guidelines. 13 Written informed consent was obtained from all the study participants. All patients were treated with coronary stenting and had received an initial aspirin loading dose of 300 mg and clopidogrel 600 mg before coronary stenting and were discharged on a dose of either 100 or 300 mg aspirin and 75 mg clopidogrel daily. Patients with concomitant abnormal platelet counts, previous myocardial infarction (MI), current infection, bleeding diathesis, severe liver disorders, cerebrovascular disease, and glycoprotein (GP) IIb/IIIa use during hospitalization were excluded from the study. The study was approved by the ethics committee of the hospital.
Coronary angiography and PCI
All patients underwent PCI within 72 hours after the admission, and PCI procedures were performed using the standard femoral approach with a 7F guiding catheter. All patients were given a loading dose of aspirin (300 mg) and clopidogrel (600 mg) immediately at the emergency department. Heparin (100 IU/kg) was administered before PCI but the use of GP IIb/IIIa inhibitors (tirofiban) was at the discretion of the operator. The infarct-related artery (IRA) was the only target of the procedure. Procedures were considered successful when thrombolysis in MI grade 3 coronary flow was achieved in the IRA. Analysis was carried out by 2 experienced cardiologists who were blinded to the patients’ clinical data.
Blood Sampling
Blood samples were collected using a 21-G needle inserted into an antecubital vein with the cuff applied to the upper arm. The cuff was removed once the first trickle of blood appeared into the 1:10 3.2% sodium citrate Vacutainers. Samples were obtained after stabilization on day 5 after ACS onset and processed within 3 hours after collection.
Clopidogrel and Aspirin Low Response
Venous blood samples from all the patients receiving clopidogrel were collected in test tubes containing hyrudin. Clopidogrel antagonists were measured by impedance aggregometry method with multiple electrode aggregometry device. Blood samples were collected in 4-mm tubes containing hyrudin for testing, then analyzed after keeping under room temperature for 30 minutes. Blood was diluted with 0.9% NaCl in the ratio of 1:2, mixed for 3 minutes in the temperature of 37°C, and 20 μL of adenosine diphosphate (ADP) was added. The changes in low response created by the platelet aggregation and adhesion with 2 pairs of electrodes in the cell during the whole process were recorded. The low response increase by the platelet adhesion to the electrodes was converted into aggregation unit (AU), and aggregation time graphic (AU/min) was drawn. The space under the aggregation line, which is the best parameter for platelet activity, was calculated. The response or low response for clopidogrel was evaluated in regard to the platelet aggregation taken at 1 week after the clopidogrel treatment. The ones with platelet aggregation >480 AU/min measured on the fifth day were assessed as resistant or nonresponder to clopidogrel. Aspirin low response is also studied and evaluated by the same method. A value of 500 AU/min is considered as the minimal resistance value for patients under dual antiplatelet therapy and 470 AU/min for patients receiving aspirin or clopidogrel alone. 14,15 In our study, we divided our study group into 5 equal groups similar to the study of Sibbing et al and accepted the group with the highest value to be nonresponsive. 16
-455G/A Polymorphism of the β-Fibrinogen Gene
Blood samples were drawn from all patients via peripheral venous route, and all samples were stored in deep freeze until analysis. Genomic DNA was isolated from peripheral blood leukocytes with use of a commercially available reagent (Invisorb Spin Blood Mini Kit; Invitek, Biodesign GmbH, Berlin, Germany). The conditions for digestions were as recommended by the manufacturer, and the fragments was separated by electrophoresis in agarose and visualized with ethidium bromide under ultraviolet light. Finally, the amplification products were selectively hybridized to a test strip, which contains allele-specific (wild-type and mutant) oligonucleotide probes immobilized as an array of parallel lines. Bound biotinylated sequences are detected using streptavidin–alkaline phosphatase and color substrates (CVD Strip Assay; ViennaLab, Vienna, Austria).
Statistical Evaluation
Descriptive statistics are presented as the mean ± standard deviation for continuous variables, median (interquartile range) for discontinuous variables, and frequencies and percentages for categorical variables. The clinical characteristics and laboratory data were analyzed with an independent t test for continuous variables and chi-square tests for categorical data. The variables were evaluated using visual (histograms and probability plots) and analytical methods (Kolmogorov-Simirnov/Shapiro-Wilk test) to determine whether they are normally distributed or not. For all statistical analyses, significance was assumed at P value less than .05. Statistical analyses were performed using the SPSS software version 15 (SPSS Inc, Chicago, Illinois).
Results
A total of 114 consecutive patients with ACS (mean age was 61 ± 7 years, and male ratio was 72.8%) were included in the study. The -455 G/A β-fibrinogen polymorphism genotype distribution in the patient group was determined as the following: 54.4% GG homozygote, 39.5% GA, and 6.1% AA homozygote. The evaluations were carried out through G allele (GG vs G/A genotype) and A allele (AA genotype). The genotypes and alleles for -455 G/A β-fibrinogen gene polymorphism are shown in Figure 1.
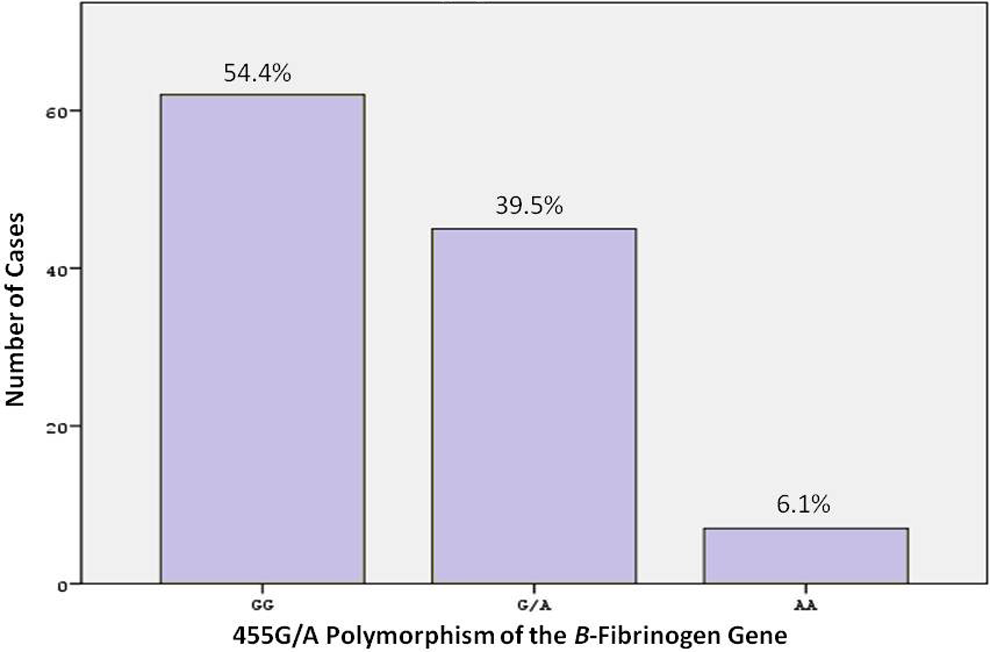
The -455 G/A β-fibrinogen polymorphism genotype distribution in overall population.
The platelet aggregation (ADP) in the patient group was 287 ± 252 AU/min (range: 0-1205) in average with a median of 221 AU/min. In all, 25 (21.9%) patients were detected to be nonresponding to clopidogrel. The ADP levels measured at 1 week after the clopidogrel treatment in the patient with and without clopidogrel low response were 709 ± 191 versus 181 ± 121, respectively. No difference was observed in terms of the frequency of 455 G/A β-fibrinogen polymorphism between the groups with and without clopidogrel low response (GG genotype: 40% vs 58.4%, GA genotype: 52% vs 36%, AA genotype 8% vs 5.6%, respectively, P = .268, G allele: 96% vs 94.4, A allele: 4% vs 5.6%, P = .749). The observation between the laboratory and the demographical features of the groups revealed significant difference only with regard to the basal platelet counts (290 ± 98 vs 256 ± 73, respectively, P = .024; Table 1). The distribution of -455 G/A β-fibrinogen polymorphism genotype in the patients with and without clopidogrel low response is shown in Figure 2.
The General and Clinical Characteristics of the Patients With and Without Clopidogrel Low Response.
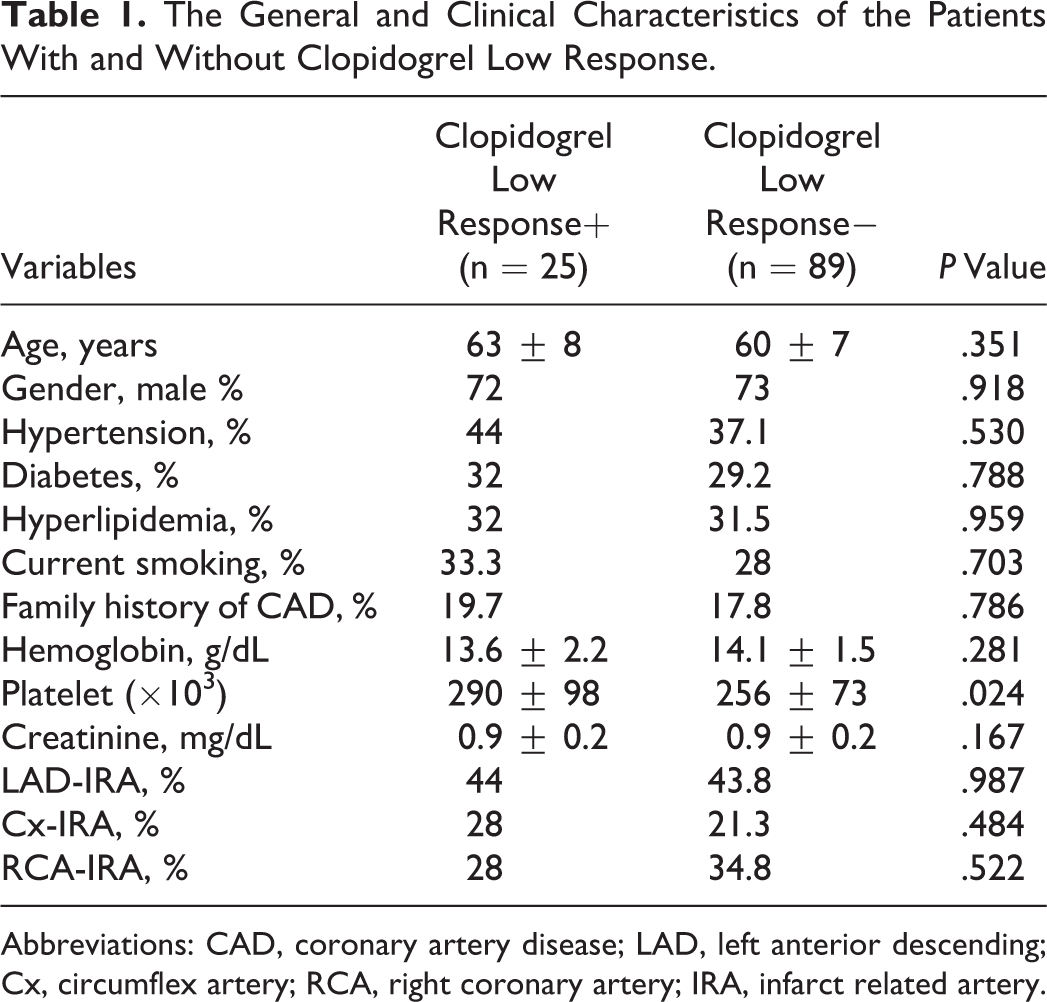
Abbreviations: CAD, coronary artery disease; LAD, left anterior descending; Cx, circumflex artery; RCA, right coronary artery; IRA, infarct related artery.
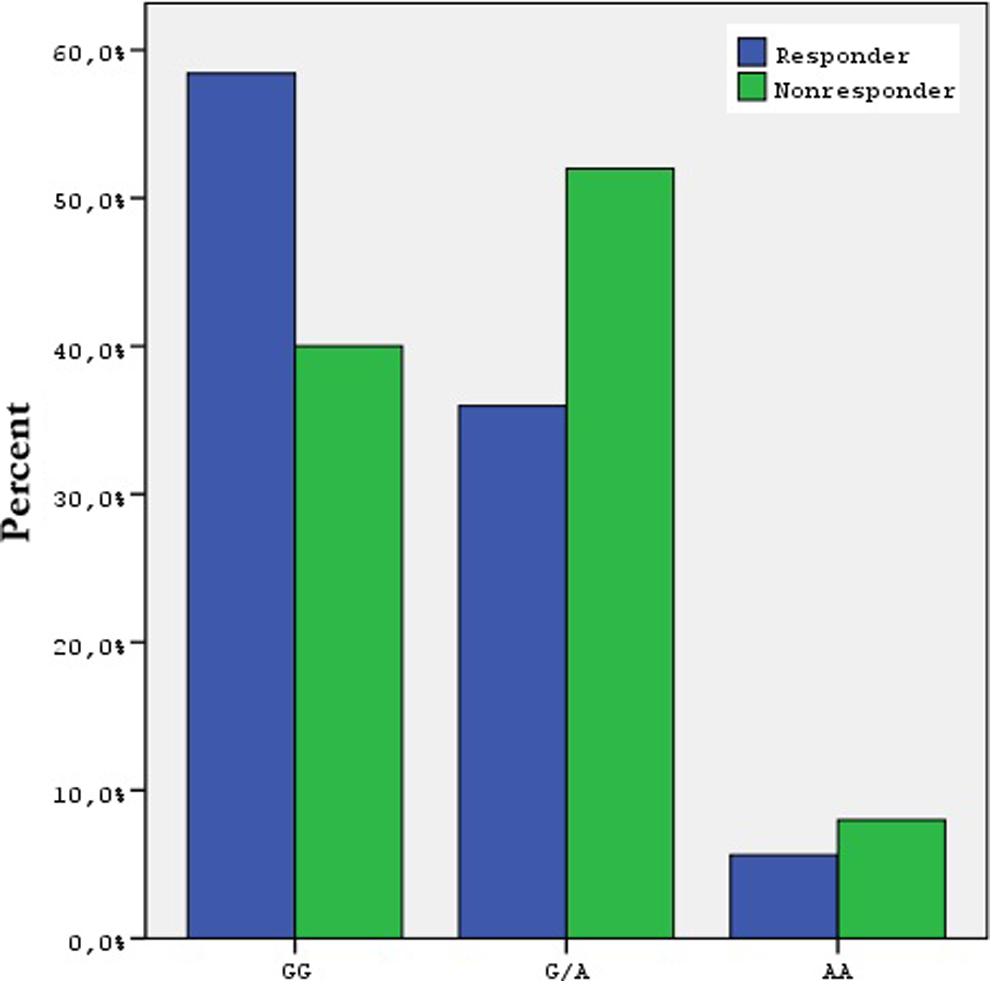
The -455 G/A β-fibrinogen polymorphism genotype distribution according to clopidogrel response.
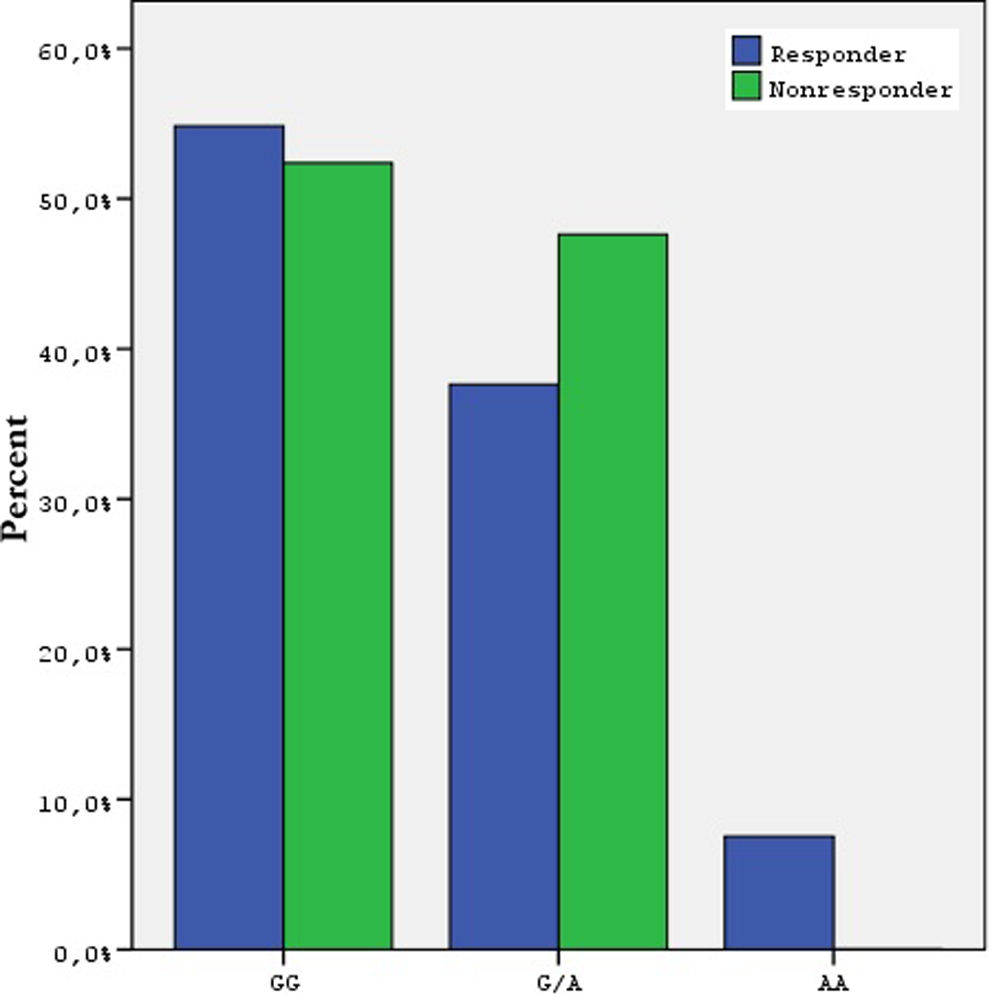
In all, 21 (18.4%) patients were detected to be aspirin nonresponders. The median collagen value measured by impedance aggregometry was 157 AU/min, 240 ± 216 AU/min (range: 0-1070) in average. The general characteristics of the patients with and without aspirin low response are given in Table 2. Collagen values measured at 1 week after the aspirin treatment in the patient with and without aspirin low response were 601 ± 167 versus 154 ± 112, respectively. No difference was observed in terms of the frequency of -455 G/A β-fibrinogen polymorphism between the groups with and without aspirin low response (GG genotype: 52.4% vs 54.8%, GA genotype: 47.6% vs 37.6%, AA genotype: 7% vs 0, respectively, P = .368, G allele 100% vs 93.5%, A allele 0 vs 6.5%, P = .232). Statistically significant difference was observed in terms of basal hemoglobin (Hb) values between the groups (11.7 ± 1.6 vs 12.7 ± 1.9, respectively, P = .032). The distribution of 455 G/A β-fibrinogen polymorphism genotype in patients with and without aspirin low response is shown in Figure 3.
The -455 G/A β-fibrinogen polymorphism genotype distribution according to clopidogrel response.
The General and Clinical Characteristics of the Patients With and Without Aspirin Low Response.
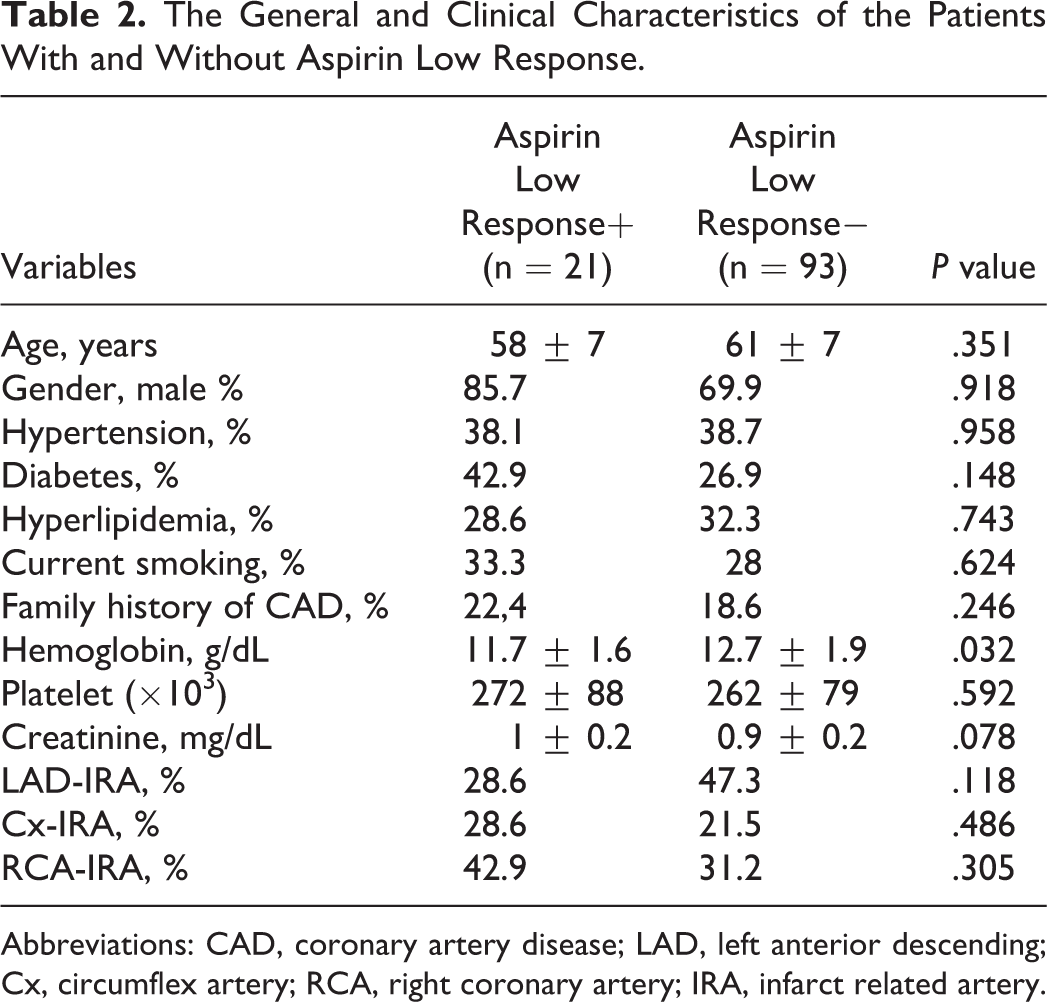
Abbreviations: CAD, coronary artery disease; LAD, left anterior descending; Cx, circumflex artery; RCA, right coronary artery; IRA, infarct related artery.
Nine (7.9%) patients were detected to be with dual antiplatelet low response. The platelet aggregation (ADP) in this group was 709 ± 132 AU/min (range: 498-878) in average with a median of 714 AU/min; the median collagen value was 627 AU/min and 634 ± 103 AU/min (range: 509-779) in average. The ADP levels measured at 1 week after the dual antiplatelet treatment in the patient with and without dual antiplatelet low response were 709 ± 132 and 251 ± 227, respectively. Collagen values measured at 1 week after the dual antiplatelet treatment in the patient with and without dual antiplatelet low response were 634 ± 103 and 206 ± 187, respectively. No difference was observed in terms of the frequency of -455 G/A β-fibrinogen polymorphism between the groups with and without dual antiplatelet low response (GG genotype: 44.4% vs 55.2%, GA genotype: 55.6% vs 38.1%, AA genotype: 0% vs 6.7, respectively, P = .492, G allele: 100% vs 94.3%, A allele: 0% vs 5.7%, P = .461).
Discussion
In our study, no difference was observed in terms of the distribution of -455 G/A β-fibrinogen polymorphism between the groups with and without aspirin and/or clopidogrel low response in the patient group who underwent aspirin and clopidogrel treatment forACS.
Identifying patients with an increased risk of the progression of stent thrombosis is important, because these patients may benefit from early treatment. In addition to measuring plasma levels of factors that are known to be associated with stent thrombosis, determination of genetic polymorphisms may offer a tool for identifying such a subgroup at increased risk of stent thrombosis. Patients with clopidogrel and/or aspirin low response are at greater risk and prone to have early stent thrombosis. 17 Several demographic and clinical characteristics as well as genetic factors have been described as predictors of antiplatelet low response. Therefore, the genetic analyses that may be associated with clopidogrel and/or aspirin low response are important. But no significant difference was observed with regard to the distribution of -455 G/A β-fibrinogen polymorphism in clopidogrel and/or aspirin low response.
Although the platelet counts were observed to be higher in the group with clopidogrel low response than the one without low response (290 ± 98 vs 256 ± 73, respectively, P = .024), basal Hb values were detected to be lower in the group with aspirin low response than the one without low response (11.7 ± 1.6 vs 12.7 ± 1.9, respectively, P = .032). This finding is consistent with those of the earlier studies, which reported that aspirin-resistant patients showed lower Hb values than aspirin-sensitive patients evaluated with VerifyNow method 18,19 and higher platelet counts in the clopidogrel low response group. 17
The importance of dual antiplatelet therapy to prevent recurrent ischemic events in patients who have ACS and who will undergo PCI is well known and widely accepted as a gold standard therapy in the current American College of Cardiology/American Heart Association and European Society of Cardiology guidelines. 20,21 Many tests are available to monitor antiplatelet therapies. 22 The reported prevalence of antiplatelet low response is discrepant, depending on different methods used and different cutoff values, varying time points, variable concentrations of agonists, and dosage of antiplatelet agents. An overall prevalence of laboratory-defined clopidogrel low response was reported to be 21% (range: 11%-44%) 9,23 and the prevalence of aspirin low response was reported to be 28% (range: 0%-57%) in average. 8 And the reported prevalence of dual low response was reported to be from 6% to 8.5%. 6,23 In our study, the measurements detected by impedance aggregometry method are as follows: clopidogrel low response 21.9%, aspirin low response 18.4%, and dual low response 7.9%.
Platelet surface receptors provide the adherence and the aggregation of the platelets to subendothelial space in case of damage to the integrity of vascular endothelium. The activated platelets directly connect to the fibrinogen, which is a circulating coagulation protein, by the integrin on their surface, GpIIb/IIIa receptors. 24,25 Human fibrinogen is composed of 3 pairs of nonidentical polypeptide chains, denoted a, b, and g, assembled in a bilaterally symmetrical arrangement connected by disulfide bonds. The 3 chains of fibrinogen are encoded by 3 independent genes grouped in a cluster of 50 kb on chromosome 4 at 4q23 to 32. 26 Fibrinogen levels are strongly correlated with traditional vascular risk factors, including age, physical inactivity, hypertension, smoking, and features of the insulin resistance syndrome. Furthermore, fibrinogen is an acute-phase reactant, in part owing to its upregulation via activation of interleukin 6-responsive elements in the promoter of all 3 fibrinogen chains; the acute-phase response is strongly implicated in the development of arterial disease and may arise from , for example, viral infection, inflammatory stimuli, and smoking. Alternatively, elevated fibrinogen might reflect the inflammation associated with atherosclerosis rather than being a causal risk factor. 10
Several polymorphisms have been identified in the genes encoding the 3 pairs of fibrinogen polypeptide chains (α, β, and γ); however, because the synthesis of the β-chain is rate limiting in vitro, most studies have focused on this gene. The main β-chain variants include the Arg448Lys, BclI, −148C/T, −455G/A (HaeIII), and -854G/A polymorphisms. 27,28 Of the β-chain polymorphisms, the -455G/A has been the most extensively studied clinically. The -455AA genotype is present in 10% to 20% of the population and is correlated with fibrinogen levels that are 10% higher than in individuals with the GG genotype. Previous studies observed an association between elevated plasma levels of fibrinogen and the risk of cardiovascular disease 29,30 . In addition, the -455A allele has been associated with the progression of atheroma. 31 In a pooled analysis of inherited hemostatic risk factors and the risk of ACS, homozygosity for the fibrinogen -455A allele was significant although only marginally associated with a decreased risk of ACS. 32 In our study, no significant relation to aspirin and/or clopidogrel low response was detected in the patient group with 455 AA homozygote . Nevertheless, the relation between the -455G/A variant and the risk of arterial thrombotic disease is controversial; only limited case–control studies have been performed. 11,12 No significant relation between the patients with clopidogrel and/or aspirin low response or dual antiplatelet low response and 455 G/A genotype was detected in our study, too.
In our study, we investigated the platelet functions by multiplate impedance aggregometry. But different methods such as vasodilator-stimulated phosphoprotein phosphorylation, light transmission aggregometry, and VerifyNow were used in the other studies. In addition to this, the definition about clopidogrel and aspirin low response or the absence of platelet inhibition due to aspirin is not clear. Although there are limiting values defined in accordance with the measurement techniques, they are not ideal. In our study, we divided the study group into 5 equal groups similar to the study of Sibbing et al and accepted the group with the highest value as resistant. 16
Study Limitations
This is a single-center study with its inherent limitations. All participants were recruited from the same medical center, and the sample size was small, which may lead to selection bias. One of the other limitations of our study is the fact that the platelet aggregation values of the patients were not measured before starting the treatment of clopidogrel and aspirin. This limitation could be overcome to a certain degree by checking the aggregation values of all patients on the fifth day and giving the same dose of clopidogrel to the patients till obtaining the aggregation values checked. However, it is a disadvantage not to study the fibrinogen level and not to report the relation of fibrinogen level to 455 G/A polymorphism and aspirin and/or clopidogrel low response. Also, the fact that the clinical end points did not occur in our study is another limitation. One patient developed stent thrombosis, and death or MI was not observed during the follow-up. The limited number of the patients with aspirin and/or clopidogrel low response might affect the study results.
As a result, there is no difference in terms of -455 G/A β-fibrinogen polymorphism between patients with and patients without aspirin and/or clopidogrel or dual antiplatelet low response in the patient group who underwent aspirin and clopidogrel treatment forACS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.