
Abstract
Objectives:
In this study, we aimed to investigate the relationship between neutrophil to lymphocyte ratio (NLR) and infarct-related artery (IRA) patency in patients with ST-segment elevation myocardial infarction (STEMI).
Methods:
A total of 349 patients with STEMI were recruited to this retrospective study. Baseline characteristics were reviewed. Patency of IRA was evaluated by thrombolysis in myocardial infarction flow grade.
Results:
Of all patients, 293 patients formed the occluded IRA group and 56 patients formed the patent IRA group. The NLR was significantly higher in occluded IRA group (4.4 ± 4.1 vs 1.9 ± 1.1, P < .001). Glucose levels were also higher in occluded IRA group (171.3 ± 78.0 vs 144.7 ± 49.7, P = .022). Regression analysis demonstrated admission NLR and plasma glucose levels as independent predictors of IRA patency.
Conclusion:
In this study, we found that admission NLR and glucose levels were higher in patients with occluded IRA than in patients with STEMI. We also found that NLR and glucose levels were independent predictors of IRA patency. Because hemogram is a cheap, fast, and widely available test, it can be used in daily practice as a predictor of IRA patency.
Introduction
ST-segment elevation myocardial infarction (STEMI) is a significant disease with its morbidity and mortality. Some predictors have been shown to be independently related to STEMI mortality. Patency of infarct-related artery (IRA) and flow rate in IRA before mechanical reperfusion are well-known predictors of worse outcomes in STEMI. 1
Inflammation has a crucial role in the pathophysiology of coronary artery disease and acute coronary syndromes. Recently, neutrophil to lymphocyte ratio (NLR) has been emerged as an important predictor of worse outcomes in many cardiovascular diseases. 2 –9 It was shown that NLR was a poor prognostic marker in acute coronary syndromes. 10 Recently, it was also shown that NLR was an independent predictor of mortality in patients with STEMI. 11 –13
Therefore, we hypothesized that there might be a relationship between NLR and flow rate in the IRA of patients with STEMI. Because complete blood count is an easy, cheap, and fast method, findings can be helpful in daily clinical practice.
Methods
Coronary angiographies between April 2011 and September 2012 were reviewed retrospectively, and 376 patients with STEMI who were admitted to coronary angiography laboratory for primary percutaneous coronary intervention (PCI) were evaluated for the present study. After excluding patients who had at least one of the exclusion criteria, 349 patients remained for further analysis. Exclusion criteria were acute or chronic infections, pulmonary thromboembolism, malignancies, renal, or hepatic diseases.
Definition of STEMI was accepted as a typical chest pain lasting for more than 30 minutes with >1-mm ST-segment elevation in 2 or more contagious leads (including posterior derivations) or new onset left bundle branch block. 13
In all patients, basal demographic properties and admission laboratory panels were reviewed. For complete blood count (CBC) analysis, Coulter Counter LH Series (Beckman coulter Inc, Hialeah, Florida) was used.
Standart Judkins technique was used for visualization of coronary grafts. Each coronary artery was visualized in at least 2 plane images. Two cardiologists who were blinded to patients’ characteristics evaluated the coronary angiograms and coronary artery flow rates. The thrombolysis in myocardial infarction (TIMI) scale was defined previously, and the flow rate in IRA was evaluated accordingly. 14 The TIMI 3 flow rate in culprit coronary artery was accepted as patent IRA and TIMI 0, TIMI 1, and TIMI 2 flows in IRA are accepted as “nonpatent” IRA.
The study was approved by the local ethics committee.
Statistical Analysis
All statistical analyses were performed using SPSS 16.0 Statistical Package Program for Windows (SPSS Inc, Chicago, Illinois). Continuous variables were given as the median ± standard deviation, and categorical variables were given as percentages. To test normality of distribution, Kolmogorov-Smirnov test was used. Mann-Whitney U test or Student t test was used to compare continuous variables. Categorical variables were compared with chi-square test. To find the predictors of IRA patency, logistic regression analysis was used. A P value of <.05 was accepted for statistical significance.
Results
A total of 349 patients were recruited to the present study. Basal characteristics were similar between the groups (Table 1). Mean age of the patients was 55.4 ± 11.5 in patent IRA group and 57.7 ± 11.3 in occluded IRA group (P = .169). In patent IRA group, 12.5% of the patients were diabetic and in occluded IRA group 18.8% of the patients were diabetic (P = .261). Ratios of patients with hypertension were similar (41.1% vs 50.5%, respectively, P = .195).
Basal Characteristics of Groups.
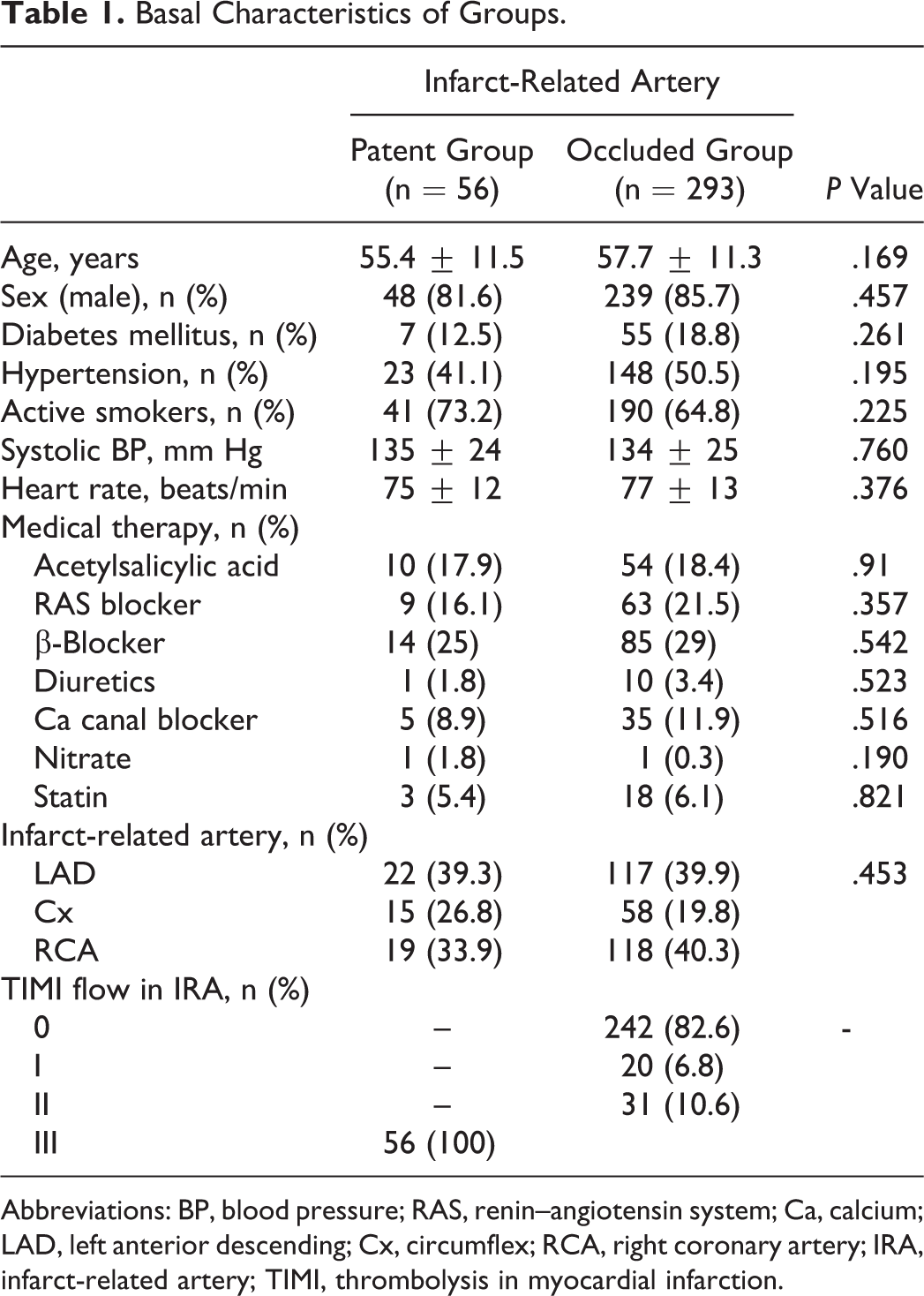
Abbreviations: BP, blood pressure; RAS, renin–angiotensin system; Ca, calcium; LAD, left anterior descending; Cx, circumflex; RCA, right coronary artery; IRA, infarct-related artery; TIMI, thrombolysis in myocardial infarction.
Culprit artery for STEMI was left anterior descending artery in 39.3% of the patent IRA group and 39.9% in the occluded IRA group (P = .453). In the occluded IRA group, it was seen that majority (82.6%) of patients were having TIMI 0 flow in IRA.
Basal laboratory findings were presented in Table 2. Admission hemoglobin levels were higher in patients with patent IRA (15.4 ± 0.9 vs 14.9 ± 1.5, P = .028). Admission glucose levels were higher in occluded IRA group (171.3 ± 78.0 vs 144.7 ± 49.7, P = .022). Admission troponin levels were higher in occluded IRA group than that in the patent IRA group. White blood cell count was also higher in patients with occluded IRA (12.0 ± 3.2 vs 10.9 ± 3.2, P = .023). Similarly, NLR was significantly higher in occluded IRA group than patent IRA group (4.4 ± 4.1 vs 1.9 ± 1.1, P < .001; Figure 1). When NLRs were compared within TIMI groups, it was seen that NLR was lowest in TIMI 3 group (1.9 ± 1.1), but NLR levels were similar between TIMI 0 (4.6 ± 4.3), TIMI 1 (3.3 ± 2.7), and TIMI 2 (3.7 ± 3.2) groups (P < .001; Figure 2).
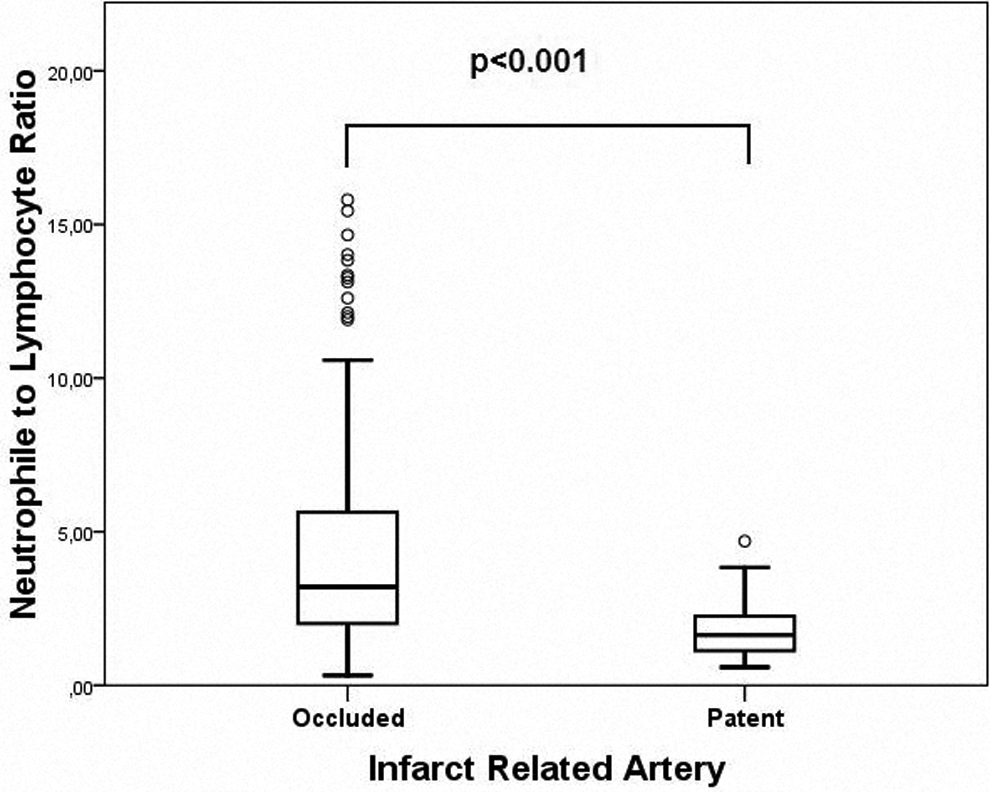
Neutrophil to lymphocyte ratios according to infarct-related artery groups.
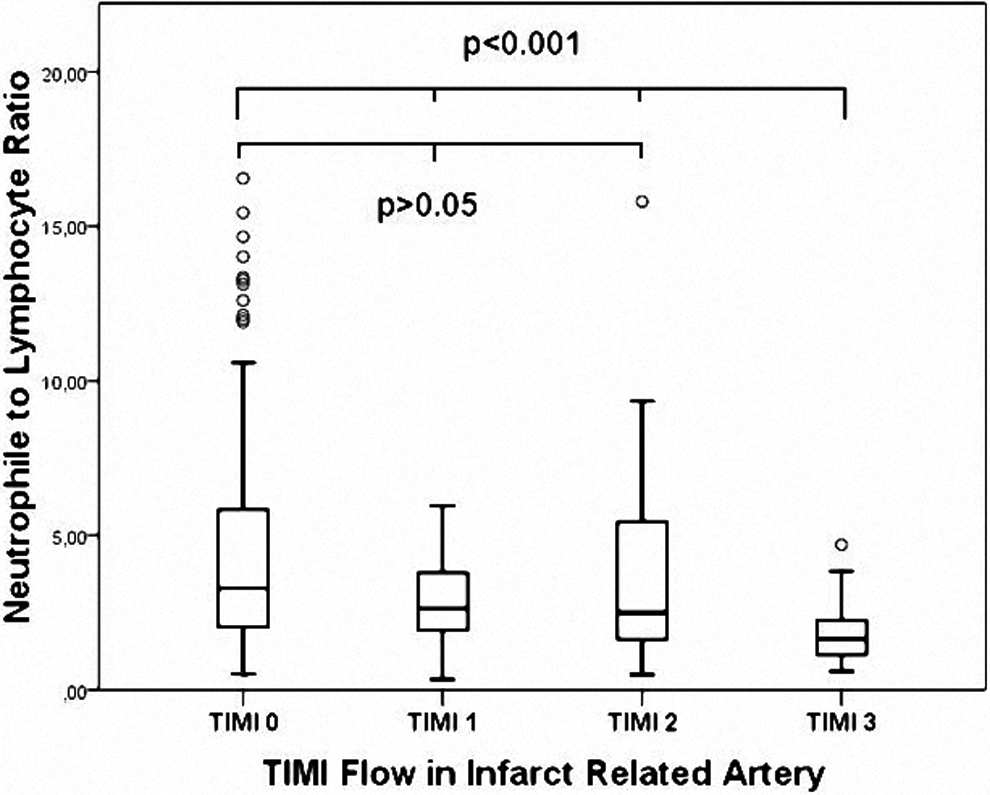
Neutrophil to lymphocyte ratios according to thrombolysis in myocardial infarction (TIMI) flow rates.
Laboratory Parameters of Groups.
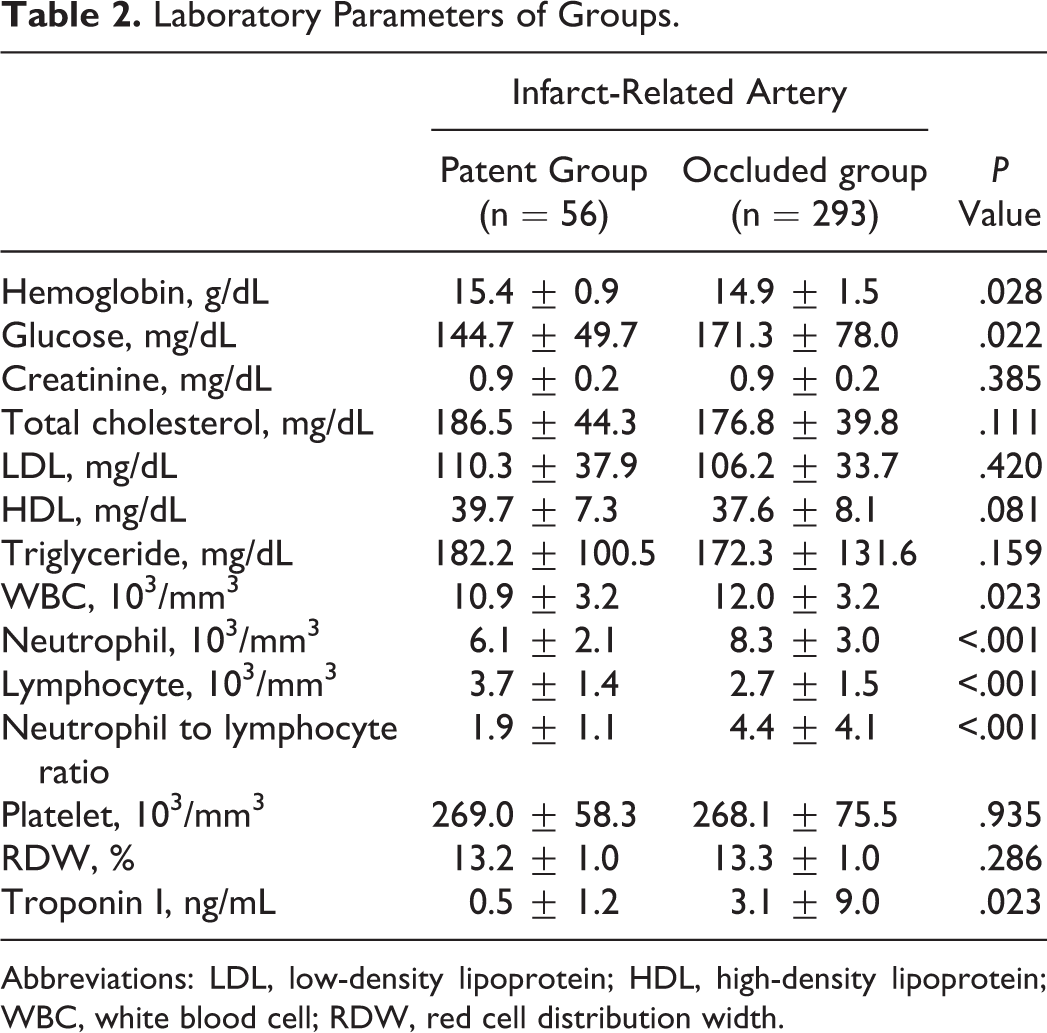
Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; WBC, white blood cell; RDW, red cell distribution width.
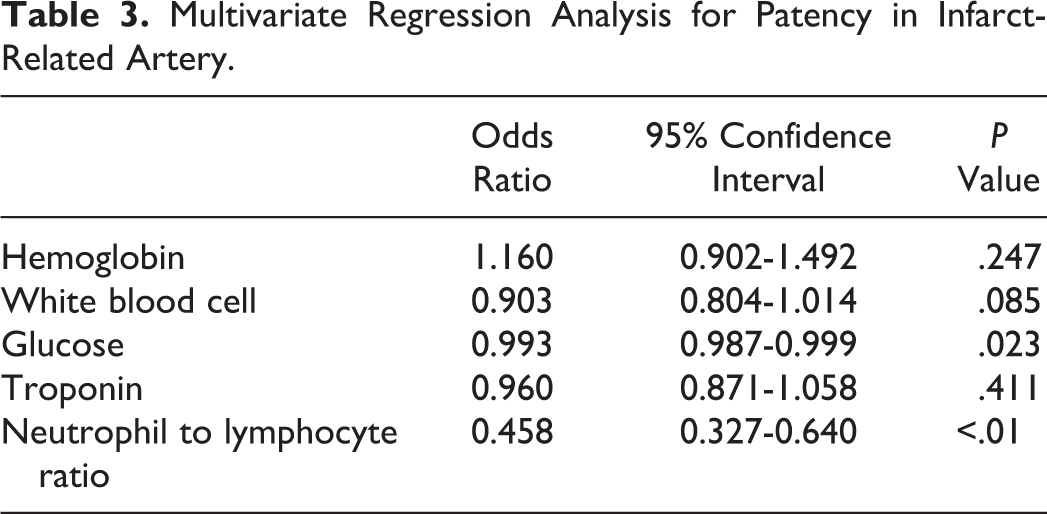
When regression analysis was performed in order to define independent predictors of IRA patency, admission hemoglobin, glucose, troponin, white blood cell count, and NLR remained for multivariate analysis. In multivariate analysis, admission NLR and glucose levels remained as independent predictors of IRA patency (Table 3).
Multivariate Regression Analysis for Patency in Infarct-Related Artery.
Discussion
In this study, we found that NLR was significantly increased in patients with STEMI who have an occluded IRA. We also showed NLR as an independent predictor of patency of IRA. Besides this, we also showed that increased admission glucose level was an independent predictor of an occluded IRA.
ST-segment elevation myocardial infarction is a devastating acute situation with its morbidity and mortality. Although in the era of primary PCI there was a significant decrease in STEMI complication rates, mortality ratio still remains to be high. For this reason, some worse prognostic markers are tried to be defined for more aggressive treatment options like glycoprotein IIb/IIIa inhibitor usage.
The flow in IRA was shown to be an independent predictor of worse outcomes in patients with STEMI. 15 In their study, Stone et al showed that patients with an occluded IRA have an increased mortality ratio than patients with a patent IRA. 16 Sen et al showed in their study that NLR was an independent predictor of no-reflow phenomenon in patients with STEMI and it is closely related to long-term prognosis. 17 It was also shown that preintervention IRA flow rate is closely related to postintervention coronary flow rate and it is known that the TIMI flow rate after primary PCI is closely related to worse outcomes in patients with STEMI. 18 –21 So early restoration of IRA patency is critical for a good prognosis. 20
Plaque rupture is generally the first event for the development of STEMI. Thrombus accumulation that eventually leads to complete occlusion of the coronary artery stops blood supply to myocardial tissue and eventually myocardial infarction starts to develop. Although the main pathophysiological mechanism of STEMI is known, some triggering mechanisms still remain to be unclear. For example, mechanism of plaque rupture and mechanism and triggering factors for platelet accumulation are not completely understood. But there are some clues for the role of neutrophils in this process. Because STEMI is closely related to inflammation and because neutrophils play a central role in inflammation, neutrophils are thought to be closely related to the development of STEMI. 22 Besides this, molecules such as leukotrienes that are secreted by neutrophils could take active role in platelet aggregation and by microvascular plugging eventually leads to vessel occlusion. 23
It is known that some vessels are completely occluded in patients with STEMI and some vessels are not. Although these patients come with similar clinical presentations, their prognosis differ from each other, and the patients with an occluded IRA have worse prognosis as compared to patients with a patent IRA. 1 Activation of a generalized inflammatory response, post-PCI coronary flow rate, and achievement of successful vessel patency after primary PCI could play role in different clinical prognosis. According to our findings, NLR was significantly higher in patients with an occluded IRA, and NLR was an independent predictor of good TIMI flow in IRA. So it can be proposed that neutrophils could play an important role in the process of complete occlusion of IRA. But increased NLR could also be a result of a more complicated process that resulted in a higher degree of inflammation that eventually leads to a higher NLR. We also think that increased NLR could also be a marker of activated inflammatory response that might have a role in microvascular plugging. 23 By this way, increased microvascular plugging might lead to IRA occlusion. Further studies are needed to clear whether increased NLR is a factor or a result of occluded IRA.
There are some limitations of our study. First of all this was a retrospective study. Second, we could not study the high-sensitivity C-reactive protein and cytokine levels, because these were not studied routinely. we also evaluated the initial presentation NLR levels in our study and we could not evaluate the follow-up values. But we think that our findings can be valuable for design of further studies, and also our findings can be used in risk stratification of patients with STEMI.
As a result, in this study, we found that NLR was significantly increased in patients with an occluded IRA, and NLR was an independent predictor of an occluded IRA in patients with STEMI who underwent primary PCI. According to our findings, it can be proposed that NLR can be used as a predictor of IRA patency. Evaluation of CBC can be useful in daily clinical practice, because it is relatively easy, cheap, and fast method that is routinely used in clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.