
Abstract
Red cell distribution width (RDW) is an index that has been shown to be an independent correlate of adverse outcomes in some cardiac conditions. Isolated coronary artery ectasia (CAE) is an abnormality of the coronary anatomy and can cause ischemia. We hypothesized that increased RDW would be associated with isolated CAE because both are associated with inflammation. In this study, 2345 patients who received coronary angiography were retrospectively evaluated. After exclusion, 75 patients with isolated CAE and 96 consecutive patients with normal coronary were included in the study. The severity of isolated CAE was determined according to the Markis classification. Baseline RDW was measured as part of the automated complete blood count. Red cell distribution width was observed to be an independent predictor of both presence and severity of isolated CAE. In conclusion, RDW is associated with both the presence and severity of isolated CAE.
Introduction
Red cell distribution width (RDW) is a measure of the variability in the size of circulating erythrocytes and it has been utilized in the differential diagnosis of anemia. 1 An elevated RDW levels are observed in many clinical settings, such as hemolysis, increased red cell destruction after blood transfusion and in the setting of ineffective red cell production, such as that of iron deficiency, vitamin B12, or folate. Red cell distribution width is also increased in clinical states such as pregnancy, thrombotic thrombocytopenic purpura (TTP), and inflammatory bowel diseases (IBDs). 2 –4 In addition, there are many reports showing association between RDW and inflammation and neurohormonal and cardiovascular risk factors. 5 –9
Coronary artery ectasia (CAE), an abnormality of the coronary anatomy, has been defined as a dilated artery luminal diameter, that is, 1.5 or more times greater than the diameter of the normal portion of the artery. 10 Isolated CAE is defined as CAE without significant coronary artery stenosis. The underlying mechanisms responsible for ectasia formation are not clearly known. However, the underlying histopathological changes in CAE are shown to be similar to the changes that are observed in atherosclerotic lesions and they include intimal–medial degeneration and hyalinization. 11 As half of the patients with CAE have coronary artery disease (CAD), we are led to believe that CAE is a variant of the CAD. 10 In addition, previous studies demonstrated that inflammation, neurohormonal process, and cardiovascular risk factors were related with CAE. 12 –14
Given that the mechanism of increased RDW and pathogenesis of CAE are similar, we hypothesized that increased RDW would be associated with the presence and severity of isolated CAE. We evaluated this hypothesis in a real world population of patients who underwent coronary angiography for suspected or known ischemic heart disease.
Methods
Patient Selection
In this study, 2345 patients who received coronary angiography between April 2009 and July 2011 were retrospectively evaluated. Of these, 103 (4.4%) patients had isolated CAE. Patients were excluded from study due to anemia, history of myocardial infarction (MI), percutaneous coronary intervention or coronary artery bypass grafting, heart failure, valvular heart disease, end-stage renal disease (ESRD), inflammatory diseases, malignancy, and menorrhagia. Twenty-eight patients were excluded due to exclusion criteria. Finally, 75 nonanemic patients with isolated CAE were included in the study. For the control group, first 96 nonanemic consecutive patients with normal coronary angiography and without exclusion criteria were included in the study.
All patients recruited in the study underwent coronary angiography for the presence of chest pain or had objective signs of ischemia (treadmill exercise or myocardial single-photon emission computed tomography). Coronary angiographies were performed in our clinic using the standard Judkins technique without nitroglycerin. Right anterior oblique view was used to evaluate the ectasia for the left coronary system and left anterior oblique view was used for the evaluation of the right coronary artery. Evaluations were visually performed by 2 experienced angiographers. The vessel diameter was calculated quantitatively in case of the presence of conflict about CAE. The severity of isolated CAE was determined according to the Markis classification. 11 Patients’ laboratory and clinical characteristics, such as age, sex, diabetes mellitus (DM), hypertension (HTN), hypercholesterolemia, smoking, family history of cardiovascular disease, height, and weight, were accessed through the medical records. In cases of inconsistencies, the patients were phoned. By dividing weight in kilograms by height in squared meters (kg/m2), the body mass index (BMI) was calculated.
Hemoglobin (Hb), RDW and white blood cell (WBC) count, and other hematological indices were measured as part of the automated complete blood count (CBC) using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). The glomerular filtration rate (GFR) was estimated by the simplified Modification of Diet in Renal Disease Equation.
Transthoracic echocardiography was performed on patients before they were discharged using a system V (Vingmed; GE, Horten, Norway) with a 2.5-MHz phased-array transducer. Recordings were taken on patients positioned in the left lateral decubitus position. The left ventricular ejection fraction was measured using modified Simpson rule. 15
Definitions
Anemia on admission was defined as a baseline Hb concentration less than 13 mg/dL in men and less than 12 mg/dL in women, in accordance with the World Health Organization criteria. The diagnosis of DM was based on previous history of diabetes treated with or without drug therapies. Hypercholesterolemia was defined as total cholesterol of ≥200 mg/dL. A BMI of ≥30 kg/m2 was defined as obese. According to the results of coronary angiography, significant coronary artery stenosis was defined as ≥50% of major coronary arteries. Types 1 and 2, which indicate severe ectatic involvement according to the Markis classification, were defined as group 1, and types 3 and 4, which indicate milder ectatic involvement, were defined as group 2. Absence of any atherosclerotic plaques was regarded as normal coronary artery.
Stable angina was defined as discomfort in the chest, jaw, shoulder, back, or arms, typically elicited by exertion or emotional stress and relieved by rest or nitroglycerin. Current smokers were defined as those who had smoked for some period during the past year. Patients were considered as having ESRD, if they were dependent on chronic dialysis. Renal insufficiency was defined as a GFR of <60 mL/min per 1.732 m2. The local ethics committee approved this study.
Statistics
Continuous variables are expressed as mean ± standard deviation. Categorical variables are expressed as percentages. To compare parametric continuous variables, the Student t test or analysis of variance was used; to compare nonparametric continuous variables, the Mann-Whitney U or Kruskall-Wallis test was used. To compare categorical variables, the chi-square test was used. Multivariate logistic regression analysis was used to identify the independent predictors of presence and severity of isolated CAE. All variables showing significance values <.1 on univariate analysis (age, sex, DM, HTN, hypercholesterolemia, current smoker, obesity, RDW, and platelet) were included in the model. Association between variables was tested using Spearman or Pearson correlation coefficient, whichever was more appropriate. Two-tailed P values <.05 were considered to indicate statistical significance. Statistical analyses were performed using SPSS, version 15.0 for Windows.
Results
Among 171 patients (mean age 54.5 ± 11.4, 54.4% male), RDW ranged from 12.4% to 16.0% (median 13.8%, mean 13.8 ± 0.6%). The baseline characteristics of angiographic normal vessels and the isolated CAE are summarized in Table 1. Patients with isolated CAE were more frequently of older age and male, had DM, HTN, hypercholesterolemia, smoking, or obesity. In addition, patients with isolated CAE had significantly elevated RDW (Figure 1A) values. Moreover, we found that isolated CAE most commonly affects right coronary artery (64%), left anterior descending artery (57.3%), and left circumflex artery (46.7%). Isolated CAE mostly affects 1 vessel (44%) or 2 vessels (42.7%), and less frequently 3 vessels (13.3%). According to the Markis classification, type 3 (30.7%) was the most common type of isolated CAE and after that types 1 and 2 (28%). The least common form was type 4 (13.3%), which was characterized by localized 1 vessel involvement.
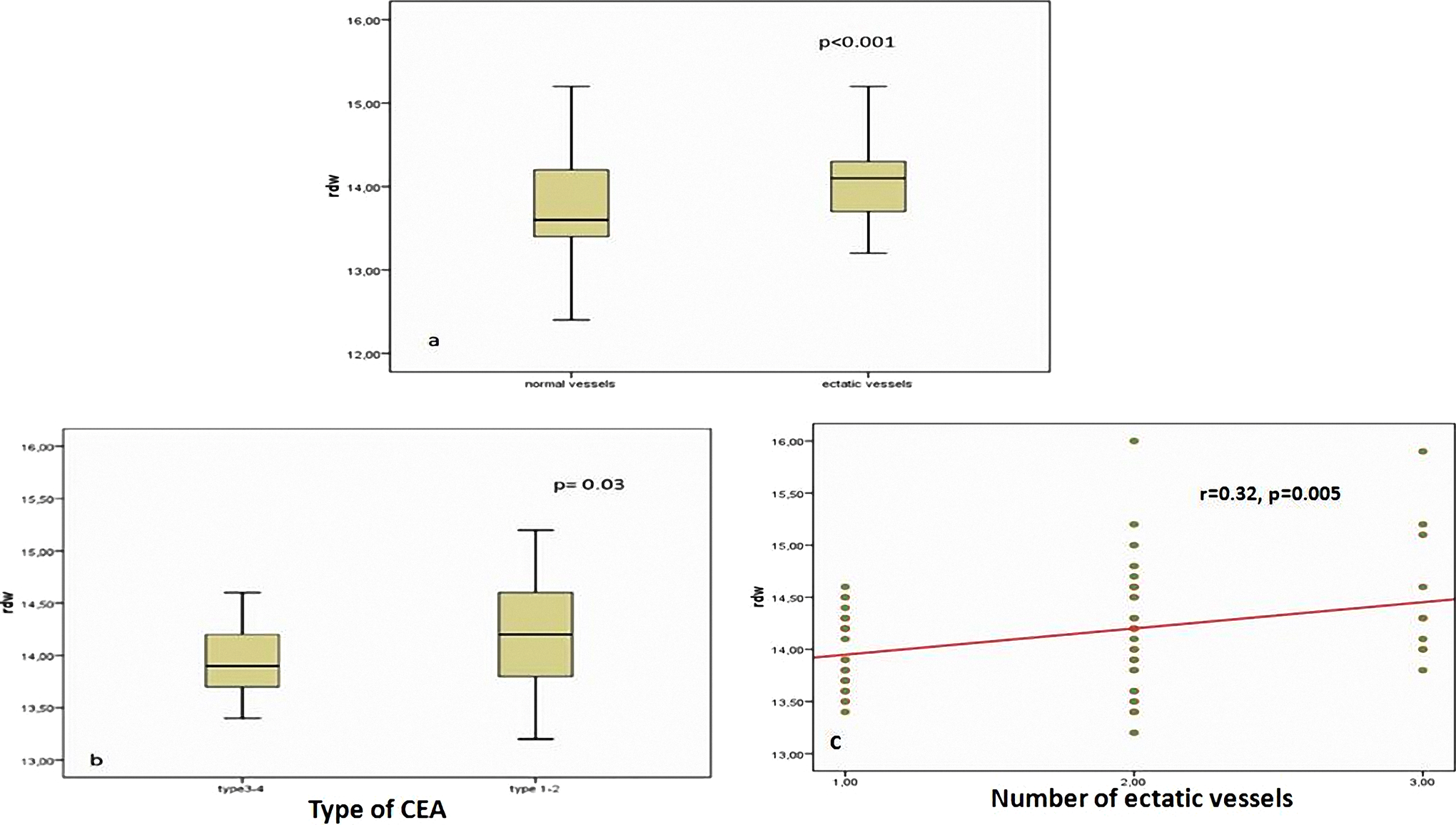
A, Red cell distribution width values of normal and ectatic vessels. B, Red cell distribution width values with severity of CAE. C, Correlation between number of ectatic vessels and RDW values. RDW indicates red cell distribution width; CAE, coronary artery ectasia.
Baseline Characteristics of Angiography of Normal and Ectatic Vessels a
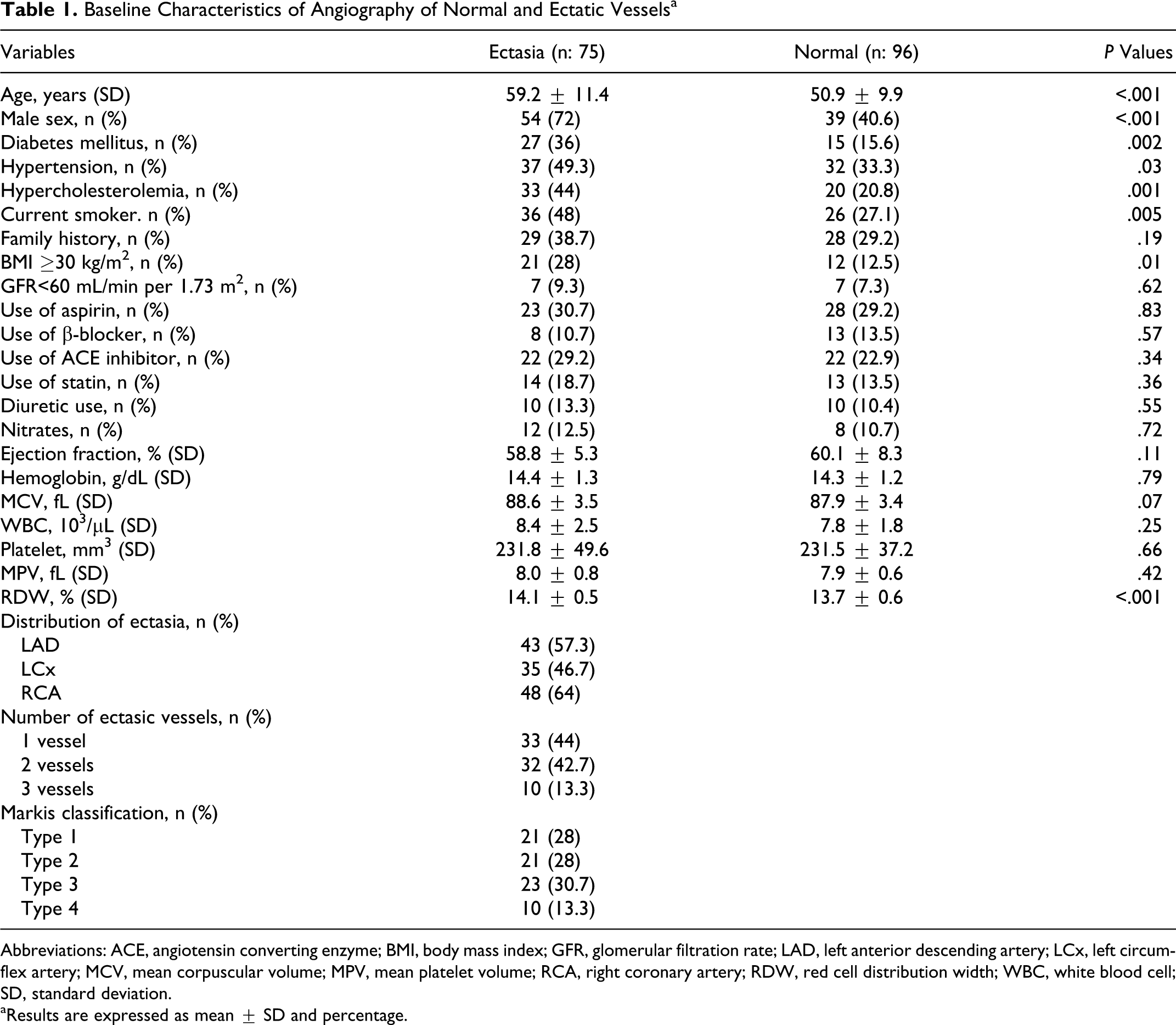
Abbreviations: ACE, angiotensin converting enzyme; BMI, body mass index; GFR, glomerular filtration rate; LAD, left anterior descending artery; LCx, left circumflex artery; MCV, mean corpuscular volume; MPV, mean platelet volume; RCA, right coronary artery; RDW, red cell distribution width; WBC, white blood cell; SD, standard deviation.
aResults are expressed as mean ± SD and percentage.
Variables found to be statistically significant in univariate analyses were entered into multivariate logistic regression analysis. Age (odds ratio [OR] = 1.07, 95% confidence interval [CI] 1.03-1.12, P < .001), DM (OR = 5.43, 95% CI 1.94-15.12, P = .001), HTN (OR = 2.88, 95% CI 1.14-7.31, P = .02), hypercholesterolemia (OR = 2.65, 95% CI 1.09-6.43, P = .03), smoking (OR = 7.01, 95% CI 2.51-19.60, P < .001), obesity (OR = 3.41, 95% CI 1.17-9.97, P = .02), and RDW (OR = 4.91, 95% CI 2.27-10.64, P < .001) were independent correlates of the presence of isolated CAE (Table 2).
Independent Predictors of Angiographic Ectasia in Multivariate Logistic Regression Analysis
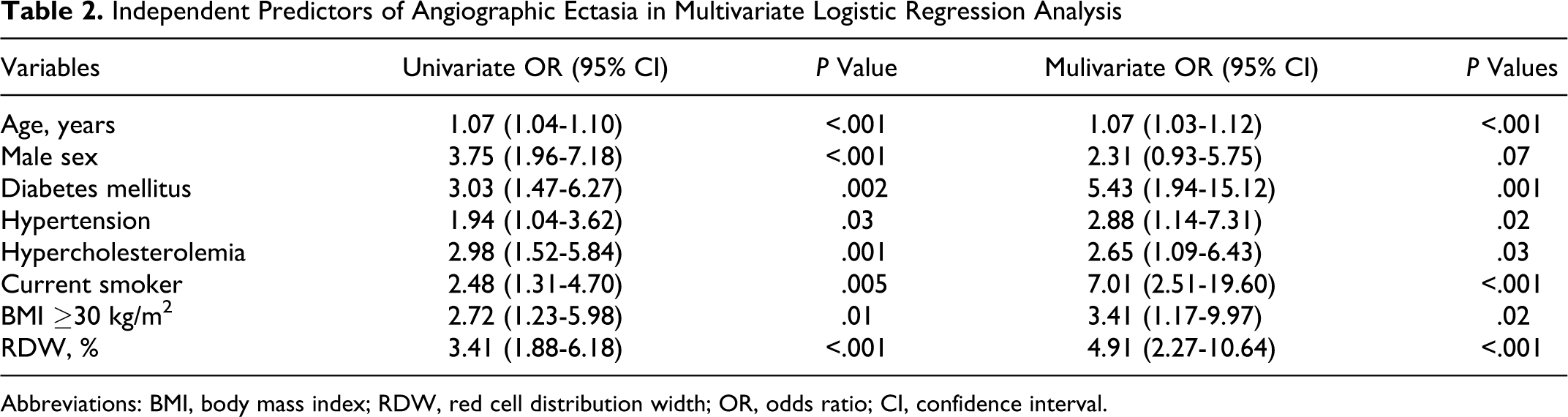
Abbreviations: BMI, body mass index; RDW, red cell distribution width; OR, odds ratio; CI, confidence interval.
The patients with severe ectasia (group 1, types 1-2) and milder ectasia (group 2, types 3-4) were compared in Table 3. Group 1 patients were more frequently of older age and had DM, as well as significantly elevated platelet and RDW (Figure 1B) values. In the multiple logistic regression analysis, only DM (OR = 5.34, 95% CI 1.56-18.26, P = .008), age (OR = 1.05, 95% CI 1.00-1.10, P = .05), and RDW (OR = 4.92, 95% CI 1.41-17.13, P = .01) were identified as independent correlates with severity of CAE (Table 4). Furthermore, there was a moderate correlation between number of ectatic vessels and RDW values (r: 0.32, P: .005; Figure 1C).
Baseline Characteristics With and Without Severe Coronary Artery Ectasia a
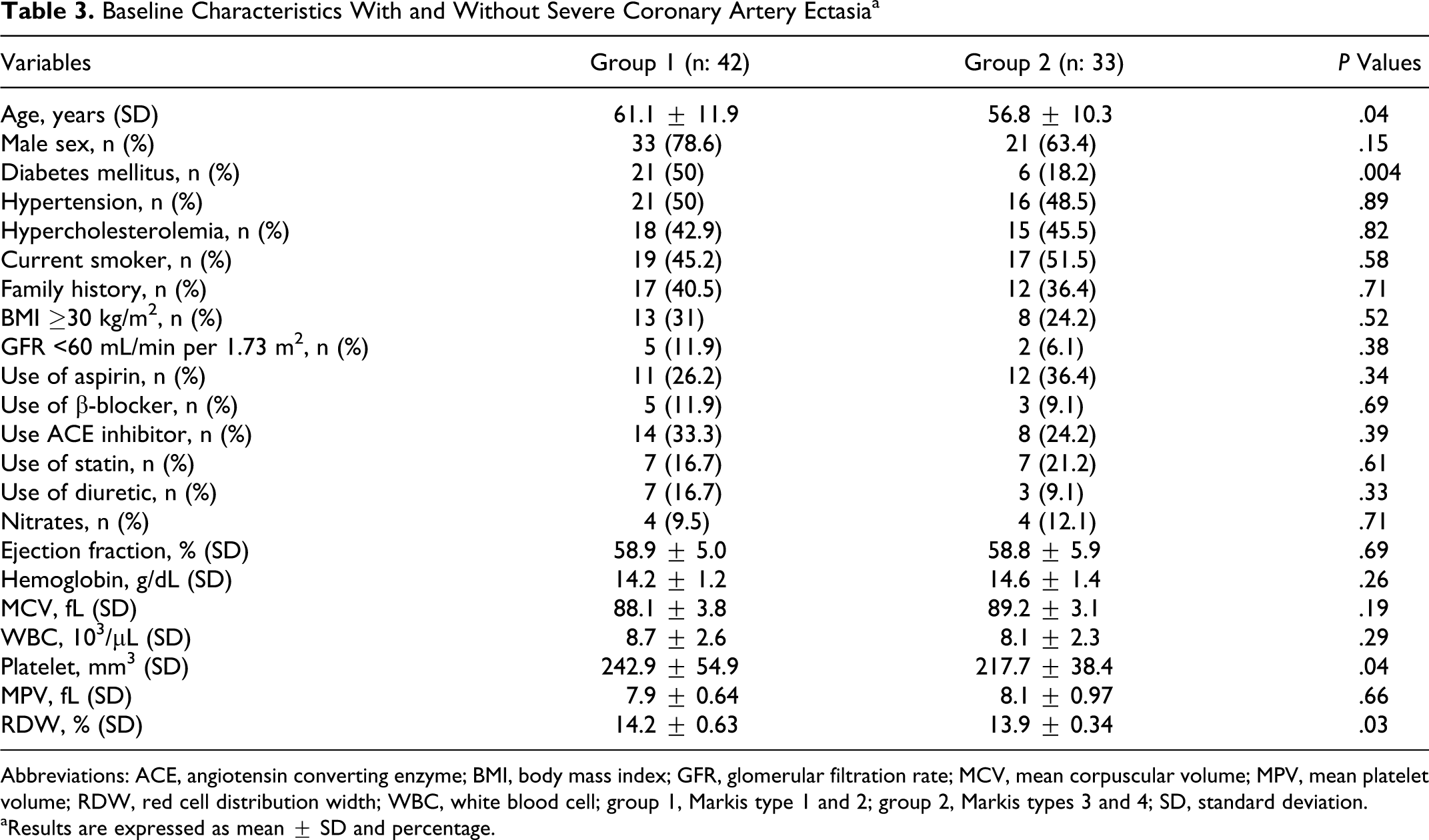
Abbreviations: ACE, angiotensin converting enzyme; BMI, body mass index; GFR, glomerular filtration rate; MCV, mean corpuscular volume; MPV, mean platelet volume; RDW, red cell distribution width; WBC, white blood cell; group 1, Markis type 1 and 2; group 2, Markis types 3 and 4; SD, standard deviation.
aResults are expressed as mean ± SD and percentage.
Independent Predictors Severity of Ectasia in Multivariate Logistic Regression Analysis

Abbreviations: RDW, red cell distribution width; OR, odds ratio; CI, confidence interval.
Discussion
This is the first study that has been conducted that evaluates the relationship between RDW and the severity of isolated CAE. A greater baseline RDW value was independently associated with the presence and severity of isolated CAE. In this study, we showed that isolated CAEs were associated with cardiovascular risk factors such as diabetes. In addition, we found that isolated CAE most commonly affects 1 vessel, right coronary artery, and the most common type of isolated CAE was type 3 according to the Markis classification.
Coronary artery ectasia is an abnormality of the coronary anatomy and might be a variant of the CAD. The CAE can cause angina pectoris and even MI with vasospasm, dissection, or thrombus in patients without CAD. 16 In several studies, patients with CAE have been shown to have increased risk of mortality, equivalent to the patients with CAD. 17 Determination of the factors associated with the presence and severity of CAE may have a salutary influence on the management of these patients. Although the underlying mechanisms responsible for ectasia formation are not clearly known, previous studies reported that inflammation, neurohormonal process, and cardiovascular risk factors were associated with CAE. 12 –14,18 –21
Red cell distribution width is a marker of variation in size of circulating red cells (anisocytosis) and is routinely reported by RBC analyzers as part of a routine CBC. 1 Thus, an elevated RDW reflects greater heterogeneity in cell sizes in the peripheral blood smear. Recently, in many studies, baseline RDW value was shown to be associated with the long-term adverse events in both acute coronary syndromes and chronic CAD. 22 –24 In addition, there are many studies showing a close relationship between RDW and inflammation and neurohormonal and cardiovascular risk factors. 5 –8,24 Dogdu et al showed that RDWs were higher in the patients with CAE than patients with normal coronary arteries. 21 In this study, we demonstrated that baseline RDW value was independently associated with the presence of, and for the first time, severity of isolated CAE.
We proposed some possible mechanistic explanations of the relationship between RDW and CAE. One of the possible mechanisms is inflammation, which plays an important role in the whole setting of the ectatic process. It is a known fact that elevated inflammatory markers, such as C-reactive protein (CRP), 12,13,21 interleukin-6, 18 –20 tumor necrosis factor-α, 19 matrix metalloproteinases, 18 and WBC counts, 12 are associated with the presence and severity of CAE. Similarly, pro-brain natriuretic peptide (BNP), which is an important index of the neurohormonal pathway, is also associated with the presence of CAE, independent of hemodynamic overload. 14 In our study, we did not measure those markers mentioned above, however, elevated RDW values have readily been shown to be associated with markers such as BNP 7,8 and CRP 5,6 as in the previous studies. Inflammation possibly contributes to an increased RDW by impairing iron metabolism, inhibiting the production of or response to erythropoietin, and shortening red blood cell (RBC) survival. 25 Additionally, in previous studies, inflammatory cytokines have been found to suppress the maturation of erythrocytes; thus, immature erythrocytes enter into the circulation and may accelerate erythropoiesis. 26 Furthermore, elevated levels of inflammatory and neurohormonal markers have been shown to cause formation of ectasia by damaging vessel wall, and also, the relation of the levels of these markers with ectatic vessel diameter has been demonstrated. 27,28 Consequently, we propose that the link between increased inflammatory activity, neurohormonal activation, and elevated RDW value is closely related with CAE.
Additionally, Finkelstein et al demonstrated that atherosclerotic risk factors (eg, DM, smoking, and advanced age) were found to be independent determinants of the presence of CAE, similar to our study. 14 Tonelli et al showed that elevated RDW is associated with HTN, DM, obesity, and lower GFR values. 24 Based on these facts, we propose that the link between elevated RDW and atherosclerotic risk factors might be closely associated with the presence of CAE.
Previous studies showed that elevated RDW values are found to be a risk factor for the presence of CAE. In concordance with the literature, we have found that elevation in the RDW values is associated with both the presence and severity of the CAE. The pathophysiological mechanistic link driving this association remains obscure for time being and a more thorough understanding of the physiological mechanism is needed. However, theoretically, we believe that neurohormonal, inflammatory activation, and the presence of atherosclerotic factors, all of which are considered risk factors for the presence and severity of CAE, affect the erythropoiesis and thereby lead to elevated RDW values.
Limitation
First, only Hb levels were measured in this study, and other factors, including iron, vitamin B12 and folate, were not measured. None of our patients received blood transfusions nor were there any pregnant IBD, TTP, or malnourished patients. Second, this was a cross-sectional study; therefore, we did not perform an analysis related to long-term events. Third, as the definition of normal coronary arteries is based on angiographic views, all the atherosclerotic plaques could not be excluded.
Conclusions
A greater baseline RDW value was independently associated with the presence and severity of CAE.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.