
Abstract
Aim:
Although the relationship between red cell distribution width (RDW) and hypertension has been well documented, there is an absence of data on the association between RDW and preeclampsia. In the present study, we have aimed to investigate the correlation of RDW with preeclampsia and its severity.
Methods:
The study population consisted of 52 (35 mild and 17 severe) patients with preeclampsia and 50 control pregnancy patients. For the entire study population, baseline RDW was measured using an automatic blood counter.
Results:
Although there were no significant differences between the preeclampsia group and the control group in terms of hemoglobin and platelet counts, the RDW (14.1 ± 1.1 vs 16.9 ± 1.7, P < .001), systolic and diastolic blood pressure, proteinuria, white blood cell, and high-sensitivity C-reactive protein levels were significantly higher in the preeclampsia group. Moreover, subgroup analysis revealed that RDW levels were significantly increased in patients with severe preeclampsia when compared to the patients with mild preeclampsia (18 ± 1.5 vs 16.4 ± 1.5, P < .001).
Conclusion:
Our study results revealed that RDW levels were associated with both the presence and the severity of preeclampsia.
Introduction
Preeclampsia, characterized by high blood pressure (BP) and proteinuria, is a life-threatening medical condition for both mother and fetus, and it is seen frequently during pregnancy. 1 There is no definitive information about how preeclampsia causes growth retardation and preterm birth. Although there are many proposed theories, uncontrolled inflammatory changes appear to be the major cause during normal pregnancy. 2 Red cell distribution width (RDW) is an readily available hematologic index that shows a variation in erythrocyte volume (anisocytosis). 3,4 Although it has been utilized in the differential diagnosis of anemia, recently RDW has been shown to be associated with hypertension and many other cardiovascular risk factors. Furthermore, it is known to have a prognostic value in cases of acute–chronic cardiac events and in the healthy population. 5 Although the exact mechanism behind this relationship is not known, high-RDW levels are believed to reflect increased inflammation.
Although the relationship between RDW and hypertension has been clearly shown, there is absence of data on the relationship between RDW and preeclampsia. In the present study, we have aimed to investigate the association between preeclampsia and RDW.
Materials and Methods
The study population consisted of 52 patients with preeclampsia and 50 control participants matched for maternal and gestational age. Of the patients with preeclampsia, 35 had mild and 17 had severe preeclampsia. Preeclampsia diagnosis was achieved based on the 2002 criteria of the American College of Obstetricians and Gynecologists 6 ; a systolic BP of 140 mm Hg or higher or a diastolic BP of 90 mm Hg or higher occurring after 20 weeks of gestation in a woman whose BP has been previously normal and detectable urinary protein (>1 + by dipstick or 0.3 g/24 hour and more). Clinical definition of severe preeclampsia (if any) was as follows: a BP ≥ 160 mm Hg/110 mm Hg, with either a proteinuria greater than 5 g over 24 hours or a urine dipstick showing 3+ or 4+ in a random urine analysis. Eclampsia, pulmonary edema, increased serum creatinine, oliguria (less than 500 mL/24 hour), fetal growth restriction, oligohydramnios, and symptoms suggestive of significant end-organ involvement (headache and visual disturbance) were accepted as other evidences of the severe disease. Women who met the criteria of preeclampsia but not severe preeclampsia were diagnosed as mild preeclampsia. Patients with multiple gestation, diabetes mellitus, chronic hypertension, infectious diseases diagnosed during pregnancy, premature rupture of membrane, active labor, polyhydramnios, anemia, inflammatory diseases, kidney diseases and signs of other concurrent medical complications were excluded from the study. The control group had no sign of any gestational complication or fetal distress, with no evidence of hypertension or proteinuria, and delivered healthy neonates of appropriate size for their gestational age. Anemia on admission was defined as a baseline hemoglobin (Hb) concentration less than 11 mg/dL in women, in accordance with the World Health Organization criteria. Our study was approved by the local ethics committee.
All participants underwent blood collection before birth via antecubital vein puncture. The Hb, RDW, white blood cell count, and other hematological indices were measured as part of the automated complete blood count using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). High-sensitivity C-reactive protein (hs-CRP) was measured using a BN2 model nephlometer (Dade-Behring, Marburg, Germany). All the pregnant participants received a daily supplementation of 0.4 mg folic acid in the first trimester and a daily supplementation of ferrous sulfate (90 mg of elemental iron) beginning at the second trimester.
Statistics
Continuous variables are expressed as mean ± standard deviation. Categorical variables are expressed as percentages. To compare parametric continuous variables, the Student t test was used; to compare nonparametric continuous variables, the Mann-Whitney U test was used; and to compare categorical variables, the chi-square test was used. Two-tailed P values <.05 were considered to indicate statistical significance. Statistical analyses were performed using SPSS, version 15.0 for Windows.
Results
A total of 52 patients (mean age 28 ± 2) were included in the study. In the preeclampsia group, the RDW ranged from 13.4% to 21.3% (median 16.8%, mean 16.9% ± 1.7%), whereas in the control group it ranged from 11.5% to 16.6% (median 14.3%, mean 14.1% ± 1.1%, P < .001). The baseline characteristics of the patients with and without preeclampsia are summarized in Table 1. There was no significant difference between the groups in terms of age, parity, and labor; however, RDW, systolic and diastolic BP, neutrophil count, proteinuria, and hs-CRP values were significantly higher in the preeclampsia group than in the control group. Furthermore, hs-CRP and RDW levels were correlated in all pregnant women (r = .249; P: .012; Figure 1). The Hs-CRP levels were found to be elevated (>3 mg/dL) in 54, 3% of mild preeclampsia, 76, 5% of severe preeclampsia patients, and 48% of the control group. Of the women with preeclampsia, 32.7% had severe preeclampsia. In addition, subgroup analysis revealed that RDW level was significantly higher in patients with severe preeclampsia (Table 2; Figure 2).
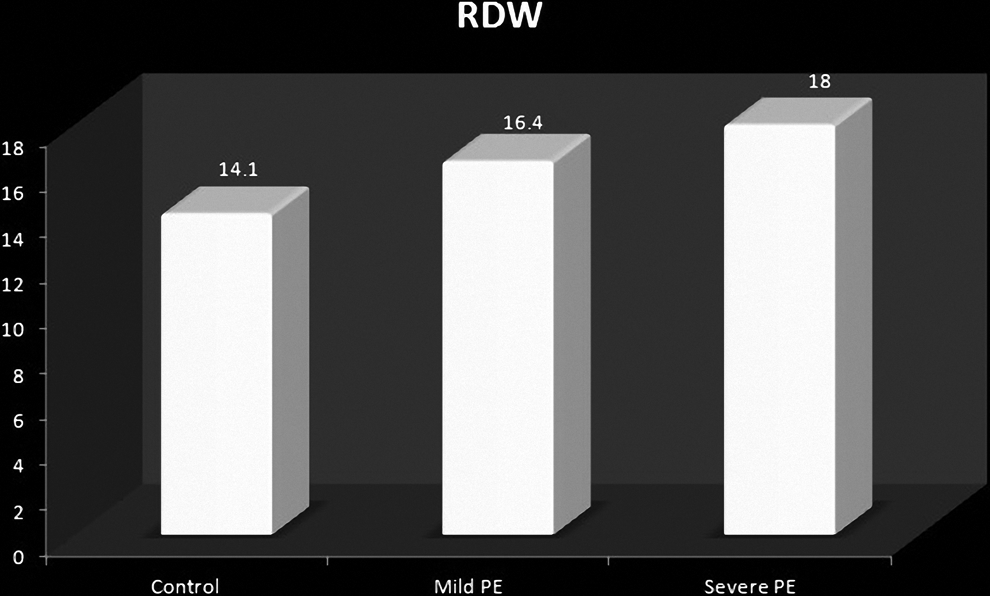
Comparison of red cell distribution width (RDW) levels in the control and the preeclampsia subgroups.
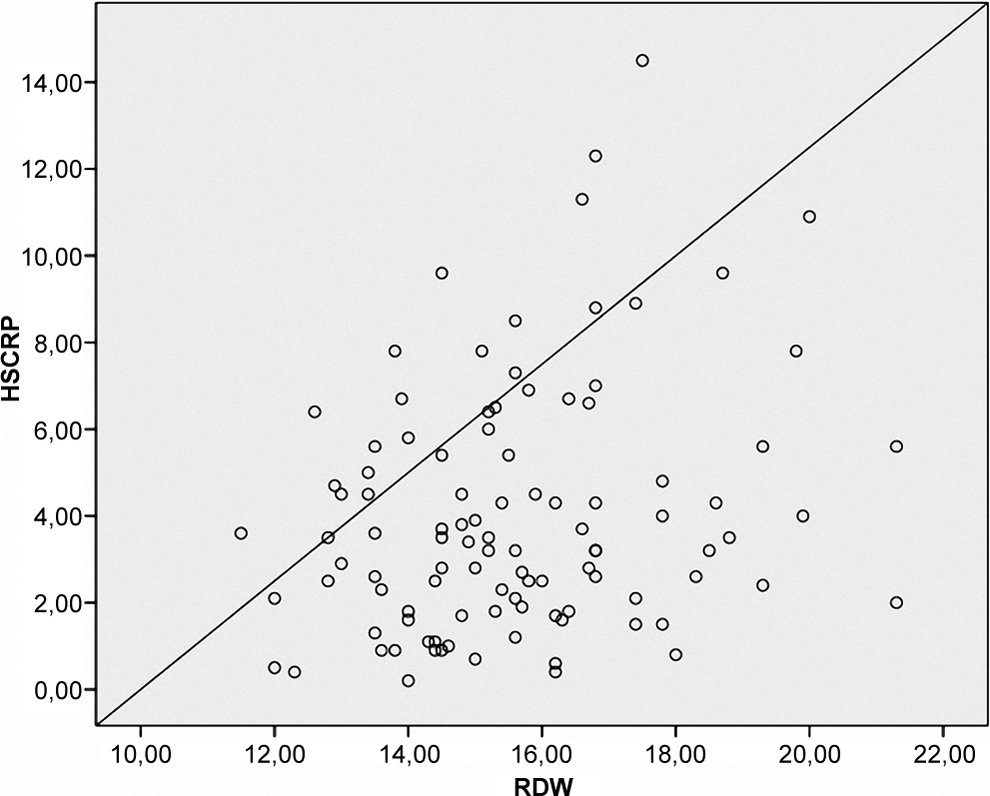
The correlation of red cell distribution width (RDW) and high-sensitive C-reactive protein (hs-CRP) in the whole population.
Baseline Characteristics of Pregnant Women With Preeclampsia and Those Without Preeclampsia.
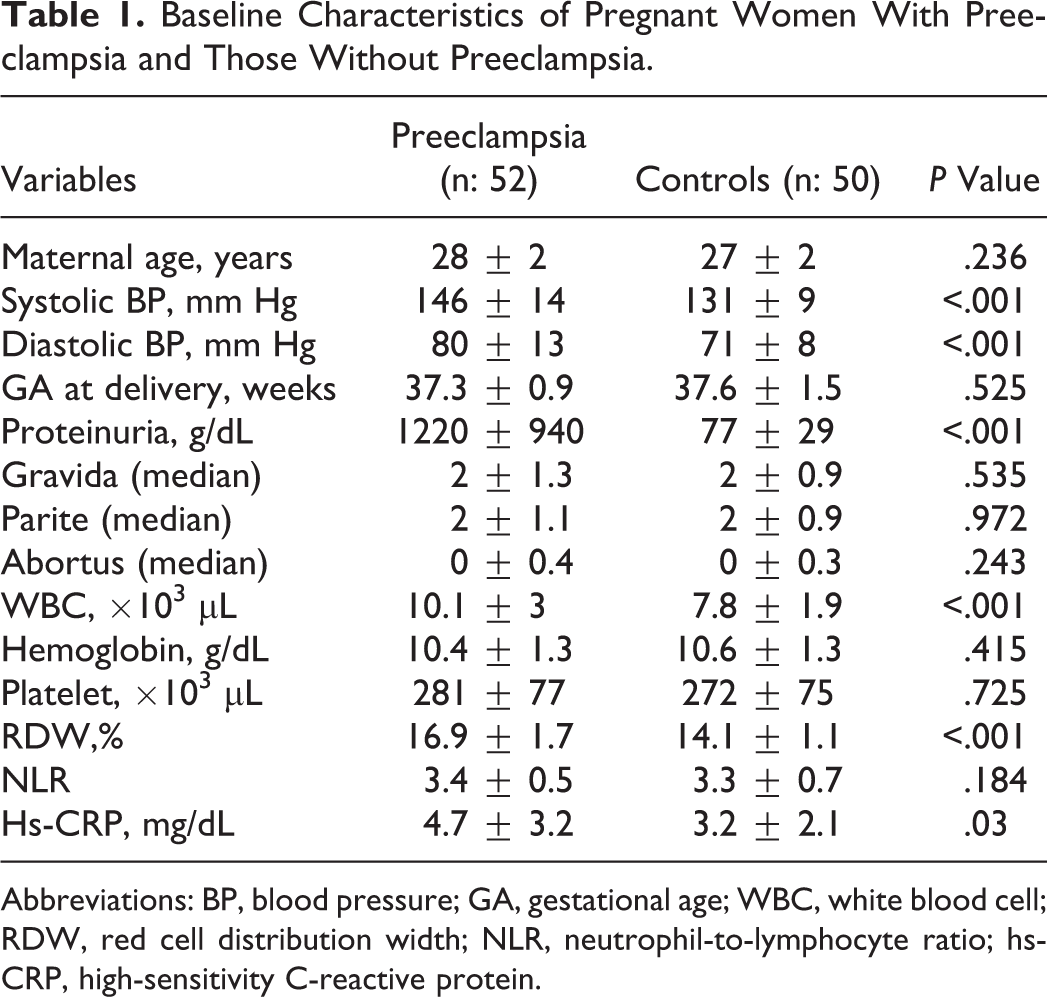
Abbreviations: BP, blood pressure; GA, gestational age; WBC, white blood cell; RDW, red cell distribution width; NLR, neutrophil-to-lymphocyte ratio; hs-CRP, high-sensitivity C-reactive protein.
Baseline Characteristics of Pregnant Women With Mild and Severe Preeclampsia.
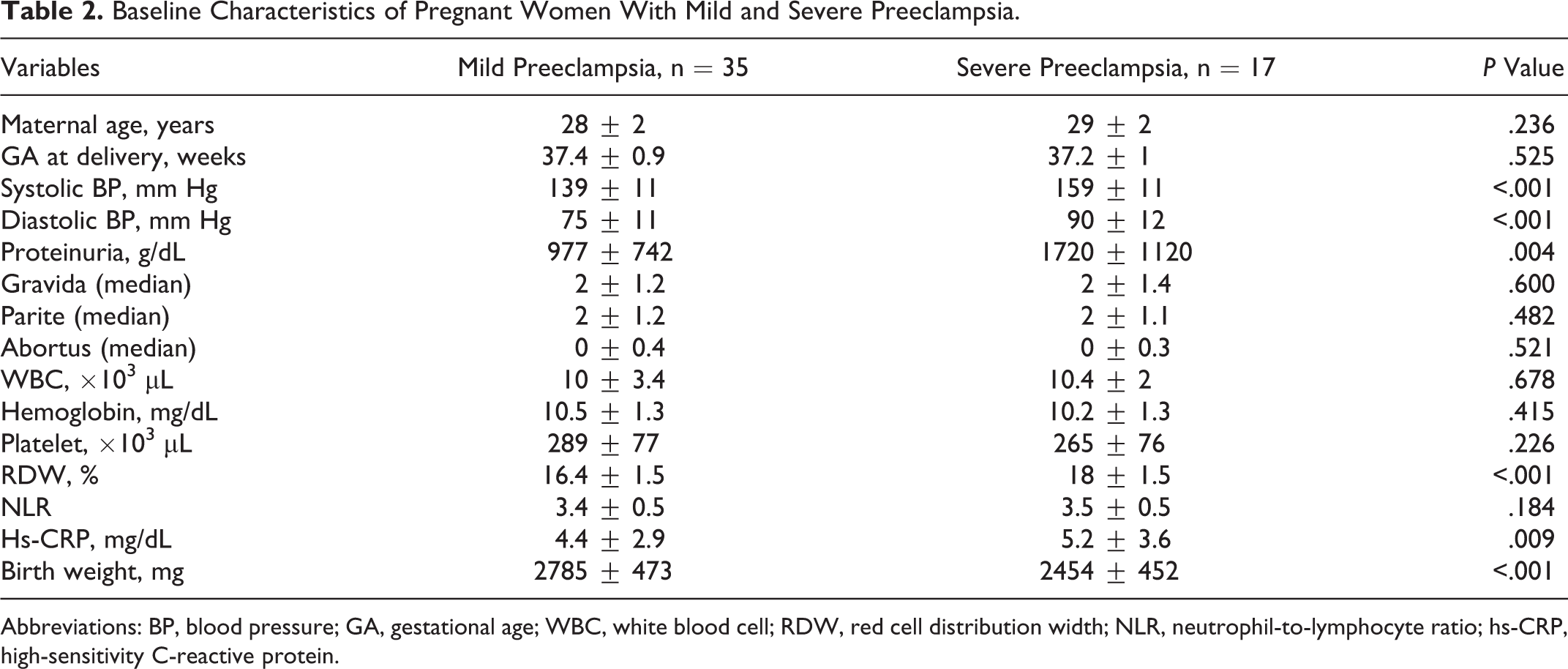
Abbreviations: BP, blood pressure; GA, gestational age; WBC, white blood cell; RDW, red cell distribution width; NLR, neutrophil-to-lymphocyte ratio; hs-CRP, high-sensitivity C-reactive protein.
Discussion
To our knowledge, this is the first study in the literature that shows a relationship between RDW levels and preeclampsia. Furthermore, we observed higher RDW levels in patients with severe preeclampsia than in patients with mild preeclampsia.
The RDW, previously used only as an index for the diagnosis of anemia, has been recently shown to be associated with the presence and severity of hypertension. 4,7 Moreover, high-RDW level is an indicator of poor prognosis in the general population and in many cardiac events such as acute myocardial infarction and heart failure. 5,8,9 The mechanism of the relationship between RDW and hypertension is not clearly known. There are several proposed theories. The most probable theory shows increased inflammation as the main cause. 10 Accordingly, in the present study, we found a positive correlation between CRP and RDW levels. Although there is no adequate data involving the influence of normal pregnancy over RDW, Shehata et al reported significantly high RDW between 34 weeks of gestation and the onset of labor. No significant changes occurred between 16 and 34 weeks of gestation or during the 7 days postpartum. 11
Preeclampsia is seen in 2% to 8% of pregnancies. 12,13 Although the exact reason behind it is not known, inadequate trophoblast invasion, altered immune tolerance, and aggravation of maternal vascular inflammatory response are regarded as being responsible for its pathophysiology. 14 In preeclampsia, fibrinoid material and foam cells stored around the spiral arteries cause deterioration of blood flow, thus leading to hypoxia. 15 In their study, Troeger et al observed increased erythropoietic stimulation and associated it with the underlying placental hypoxia in the patients with preeclampsia. 16 Since erythrocytes have a poor repair mechanism, they are destroyed by any minor event causing damage. Increased inflammatory process (eg, neutrophil, monocyte, and macrophage) in preeclampsia leads to the destruction of red blood cells by acting with oxygen radicals and proteolytic enzymes. After this destruction, the levels of some catabolic products, such as erythrocyte membrane band 3 protein, have been observed to increase. 17 –19 Tissue hypoxia-induced erythropoietin secretion stimulates bone marrow. Thus, the number of immature erythrocytes increases in the blood flow, and reticulocytosis takes place. 20
The relationship between RDW and preeclampsia can be explained by several possible mechanisms. Increased inflammatory response is the most probable underlying mechanism. Previous studies have reported that preeclampsia was associated with increased tumor necrosis factor α and interleukin 6 levels 21 while also revealing a close relationship between RDW levels and increased inflammation. 10 Inflammation likely increases RDW levels via impairment of iron metabolism, disruption of response to erythropoietin, and shortening of the lives of red blood cells. 22 Furthermore, inflammatory cytokines have been shown to cause the immature erythrocytes to enter the circulation by impairing erythrocyte maturation. 23
There is a need for further studies in order to completely understand the pathophysiologic relationship between RDW and preeclampsia. Nonetheless, we believe that activation of inflammation, which is thought to be closely related to preeclampsia, increases RDW levels through its impact on erythropoiesis.
Limitation
First, being a single-center study and including a relatively low number of patients may be regarded as a limitation. Second, since our study was of cross-sectional design, the predictors of preeclampsia and prognostic value of RDW in patients with preeclampsia were not investigated. Third, RDW may be increased in many clinical events causing ineffective erythropoiesis, such as hemolysis, transfusion, and deficiency of iron, vitamin B12, or folate. Furthermore, clinical diseases such as thrombotic thrombocytopenic purpura (TTP) and inflammatory bowel disease (IBD) can also lead to increased RDW levels. 24,25 In this study, we measured only Hb levels and did not evaluate iron, vitamin B12, and folic acid levels. However, none of the study patients had a diagnosis of IBD or TTP, and no case of malnutrition was observed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.