
Abstract
In this study, we aimed to investigate the association of the neutrophil-to-lymphocyte ratio (NLR) with Global Registry of Acute Coronary Events (GRACE) risk score in patients with ST-segment elevated myocardial infarction (STEMI). We analyzed 101 consecutive patients with STEMI. Patients were divided into 3 groups by use of GRACE risk score. The association between NLR and GRACE risk score was assessed. The NLR showed a proportional increase correlated with GRACE risk score (P < .001). The occurrence of in-hospital cardiac death, reinfarction, or new-onset heart failure was significantly related to NLR at admission (P < .001). Likewise, NLR and GRACE risk score showed a significant positive correlation (r = .803, P < .001). In multivariate analysis, NLR resulted as a predictor of worse in-hospital outcomes independent of GRACE risk score. Our study suggests that the NLR is significantly associated with adverse in-hospital outcomes, independent of GRACE risk score in patients with STEMI.
Introduction
Atherosclerosis is the major cause of cardiovascular disease that still accounts for most of the mortality worldwide. 1 The role of inflammation in the development and progression of atherosclerosis has been clarified. 2 Inflammation characterizes all phases of atherothrombosis, and the presence of inflammation at the site of the atherosclerotic lesion has a critical pathophysiological role in plaque formation and acute rupture. 2,3 The rupture of a vulnerable atherosclerotic plaque and consecutive thrombus formation leads to occlusion of the affected coronary artery followed by necrosis of the subtended myocardial tissue. These events are clinically referred to as acute coronary syndrome (ACS), which includes ST-segment elevated myocardial infarction (STEMI), non-STEMI, and unstable angina pectoris. 3,4
The ACSs are a heterogeneous population with varying risks of death and recurrent cardiac events, in long-term as well as short-term follow-up. In these patients, early risk stratification plays a central role, as the benefit of more aggressive treatment strategies seems to be proportional to the risk of adverse outcomes. The Global Registry of Acute Coronary Events (GRACE) risk scores has a high diagnostic performance for adverse outcomes in ACS and are the preferred scoring system that current European Acute Coronary Syndrome guidelines recommend to apply on admission and at discharge in daily clinical practice. 5
White blood cell (WBC) count and its subtypes are also known as classic markers of inflammation in cardiovascular diseases. 6 In recent years, neutrophilia and relative lymphopenia were shown to be an independent predictor of mortality in patients with acute heart failure. 7,8 Moreover, neutrophil-to-lymphocyte ratio (NLR) was introduced as a potential marker to determine inflammation in cardiac and noncardiac disorders and shown as a predictor of long-term mortality in patients who underwent percutaneous coronary intervention (PCI). 9 –14 Additionally, the NLR has been associated with long-term mortality in patients with STEMI. 10,15,16 As neutrophil and lymphocyte values are readily available in routine blood count analysis, NLR may be used as a cost-effective predictor of inflammation and cardiovascular complications.
The relationship between NLR and STEMI has been shown in several studies, but there are no data available about the association of NLR levels with GRACE risk score. In this study, we aimed to investigate the association of the NLR with GRACE risk score and in-hospital major advanced cardiac events in patients with STEMI undergoing primary PCI.
Methods
Study Design, Definitions, and End Points
In this retrospective observational study, between May 2010 and December 2010, 101 consecutive patients with STEMI treated with PCI within 6 hours from symptoms onset were investigated. The STEMI was defined based on the criteria formulated by the American College of Cardiology and the European Society of Cardiology. 17 Briefly, typical chest pain >30 minutes with a new ST-segment elevation measured from the J point in ≥2 consecutive leads with at least 0.2 mV in leads V1, V2, and V3 or at least 0.1 mV in the remaining leads on the electrocardiogram or new on set left bundle branch block. Demographic data and variables that determine the in-hospital death or myocardial infarction (MI) GRACE risk score points (that include age, creatinine, heart rate, systolic blood pressure, Killip class, cardiac arrest at admission, elevated cardiac markers, and ST-segment deviation) were recorded. 18 The GRACE risk scores were stratified as low (<108 points), intermediate (108-140 points), and high (>140 points). For each patient, we estimated the risk of in-hospital mortality and coronary events according to Grace risk score. Diabetes mellitus was defined as a fasting blood glucose level >126 mg/dL or current use of a diet or medication to lower blood glucose and/or hemoglobin A1c >6.5%. Hypertension was considered to be present if the systolic pressure was >140 mm Hg and/or diastolic pressure was >90 mm Hg as well as patients receiving antihypertensive treatment were accepted as hypertensive. Hyperlipidemia was defined as low-density lipoprotein cholesterol >130 mg/dL, total cholesterol >200 mg/dL, triglyceride >200 mg/dL, or current use of any antihyperlipidemic medication. We considered depressed left ventricle ejection fraction as values <50%. Smoking was defined as active smoking in the last 6 months.
Patients with clinical evidence of active infection, cancer, hematological disease, systemic inflammatory conditions, autoimmune disease, end-stage liver disease, and renal failure were excluded from the study.
The primary end point was the combination of death of any cause, acute MI, and onset of heart failure in-hospital period. Reinfarction was defined as the appearance of new ischemic symptoms or electrocardiographic ischemic changes accompanied by reelevation of cardiac biomarkers.
Laboratory Analysis
On admission, venous blood was obtained from all the patients. Neutrophils, lymphocytes, and WBC were measured as part of the automated complete blood count before starting any medication. The NLR was calculated as the ratio of the neutrophils and lymphocytes, both obtained from the same automated blood sample at admission. All measurements were performed 30 minutes after blood collection by an automatic blood counter.
Statistical Analysis
Statistical analyses were performed using the SPSS software version 17.0 (SPSS Inc, Illinois). Categorical variables were summarized as percentages and compared with Pearson chi-square test. Continuous variables were presented as mean ± standard deviation and tested for normal distribution by the Kolmogorov-Smirnov test. Comparison analyses between groups were made using Kruskal-Wallis test and one-way analysis of variance test followed by Mann-Whitney U test and Tukey test where appropriate. Spearman test was used for correlation analysis between NLR and GRACE risk score. A multivariable logistic regression model was used to evaluate the independent contribution of NLR to the risk of new cardiac events. Age, NLR, GRACE risk score, MPV, and troponin T levels were selected for multivariable logistic regression analyses. The adjusted odd ratios and 95% confidence intervals (CIs) are presented. A P value lower than .05 was considered significant.
Results
Baseline Characteristics
The study population consisted of 101 consecutive patients with STEMI. In all, 80.2% of the patients were male, and mean age of patients was 57.97 ± 12.24 years. In all, 42 (41.6%) patients were hypertensive, 23 (22.8%) patients were diabetic, 34 (33.7%) patients were hyperlipidemic, and 57 (56.4%) patients were smokers.
According to the GRACE risk score, 21 (20.8%) patients had low GRACE risk scores, 48 (47.5%) patients had intermediate GRACE risk scores, and 32 (31.7%) patients had high GRACE risk scores. Demographic and biochemical characteristics of patients in GRACE risk score groups are shown in Table 1. The NLR showed a proportional increase correlated with GRACE risk score (P < .001; Table 1; Figure 1).
Demographic and Biochemical Characteristics of Patients in GRACE Risk Score Groups.
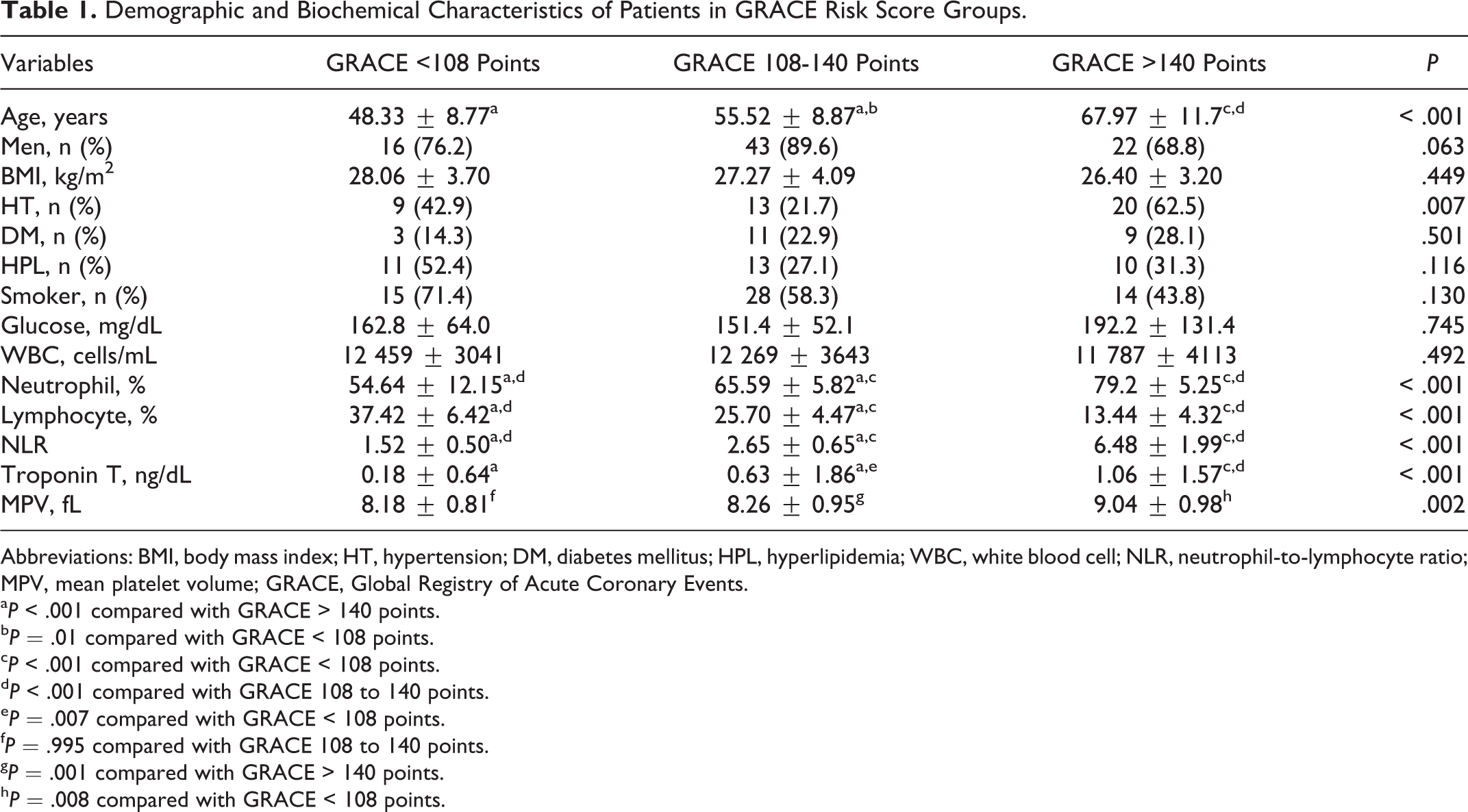
Abbreviations: BMI, body mass index; HT, hypertension; DM, diabetes mellitus; HPL, hyperlipidemia; WBC, white blood cell; NLR, neutrophil-to-lymphocyte ratio; MPV, mean platelet volume; GRACE, Global Registry of Acute Coronary Events.
a P < .001 compared with GRACE > 140 points.
b P = .01 compared with GRACE < 108 points.
c P < .001 compared with GRACE < 108 points.
d P < .001 compared with GRACE 108 to 140 points.
e P = .007 compared with GRACE < 108 points.
f P = .995 compared with GRACE 108 to 140 points.
g P = .001 compared with GRACE > 140 points.
h P = .008 compared with GRACE < 108 points.
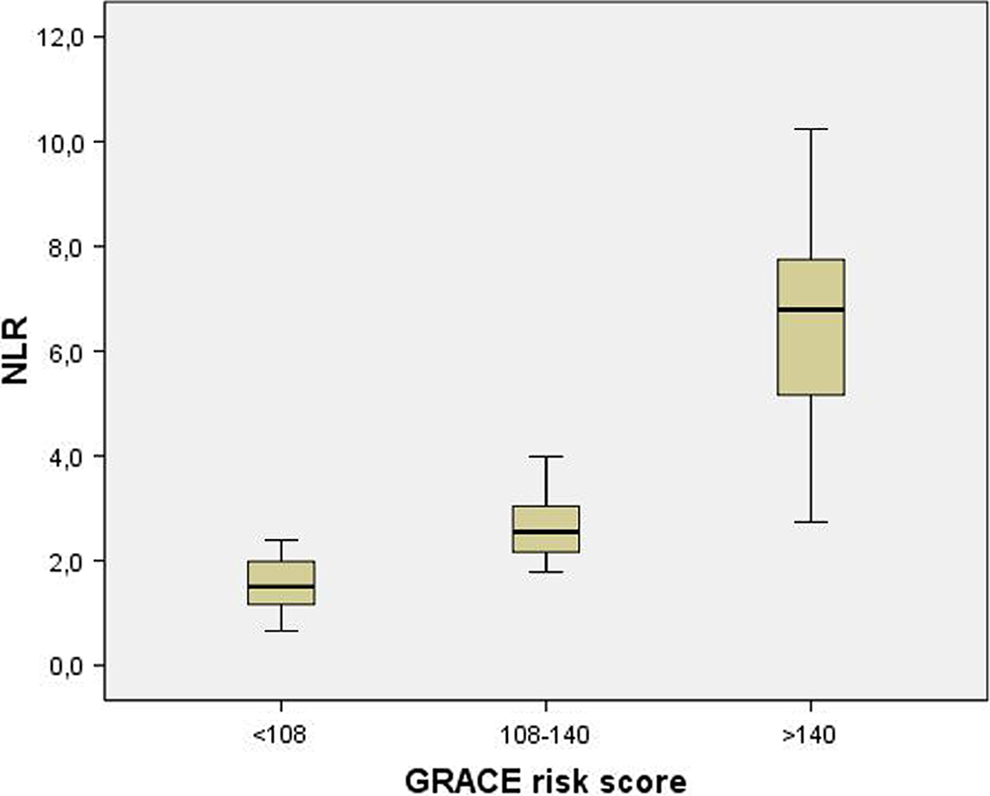
Comparison of Global Registry of Acute Coronary Events (GRACE) risk score groups in terms of neutrophil-to-lymphocyte ratio (NLR).
Correlation With In-Hospital Events
During the in-hospital period, 11 (10.9%) patients presented cardiac events (3 cardiac death, 2 reinfarction, and 6 new-onset heart failure). These patients had more advanced Killip functional class and higher GRACE risk score (all of these patients are in the GRACE > 140 points group). Demographic and biochemical characteristics of patients with and without in-hospital cardiac events are shown in Table 2. The occurrence of in-hospital cardiac death, reinfarction, or new-onset heart failure was significantly related to NLR at admission (8.18 ± 1.16 vs 3.07 ± 1.77, P < .001). In the correlation analysis, NLR showed a significant positive correlation with the following; GRACE risk score (r = .803, P < .001, Figure 2), age (r = .516, P < .001), and troponin T levels (r = .507, P < .001).
Demographic and Biochemical Characteristics of Patients With and Without In-Hospital Cardiac Events.
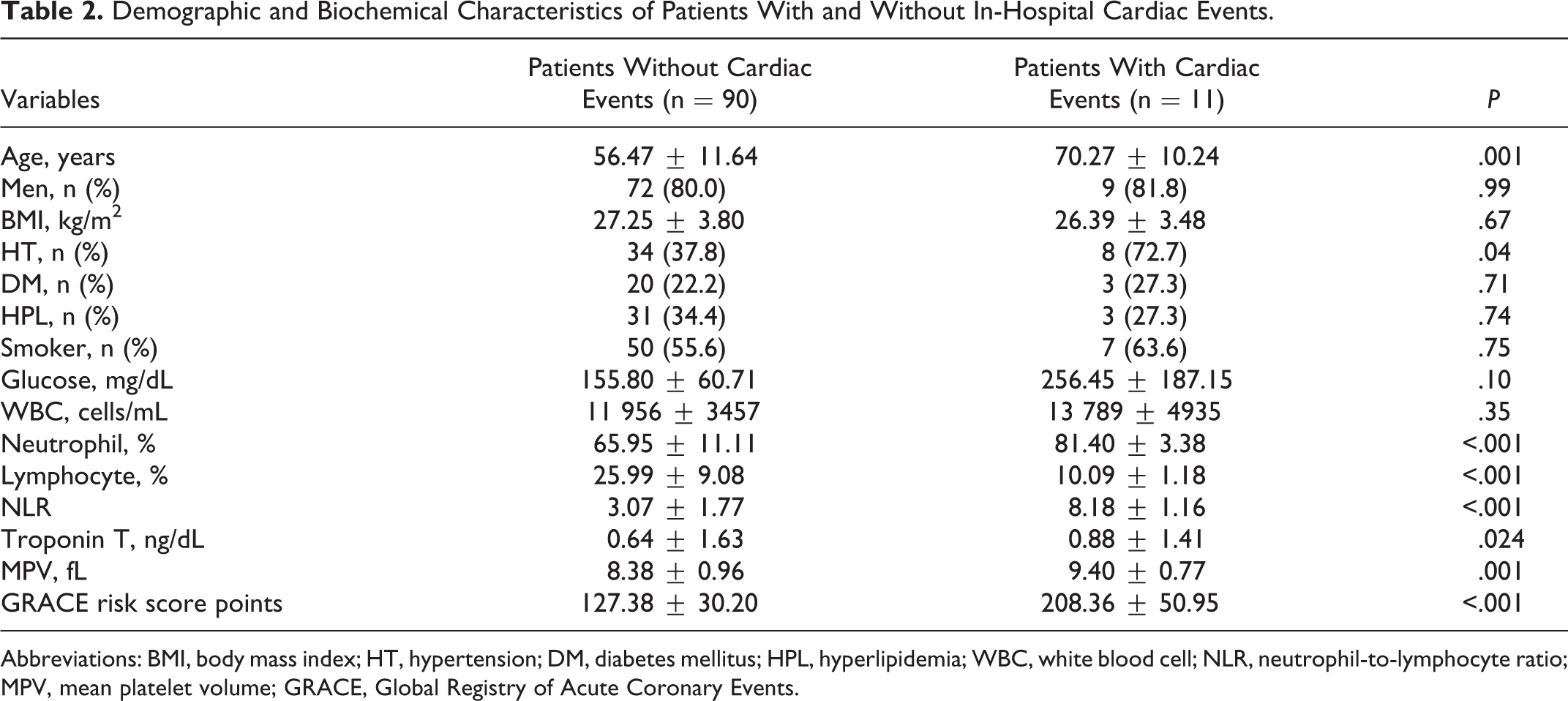
Abbreviations: BMI, body mass index; HT, hypertension; DM, diabetes mellitus; HPL, hyperlipidemia; WBC, white blood cell; NLR, neutrophil-to-lymphocyte ratio; MPV, mean platelet volume; GRACE, Global Registry of Acute Coronary Events.
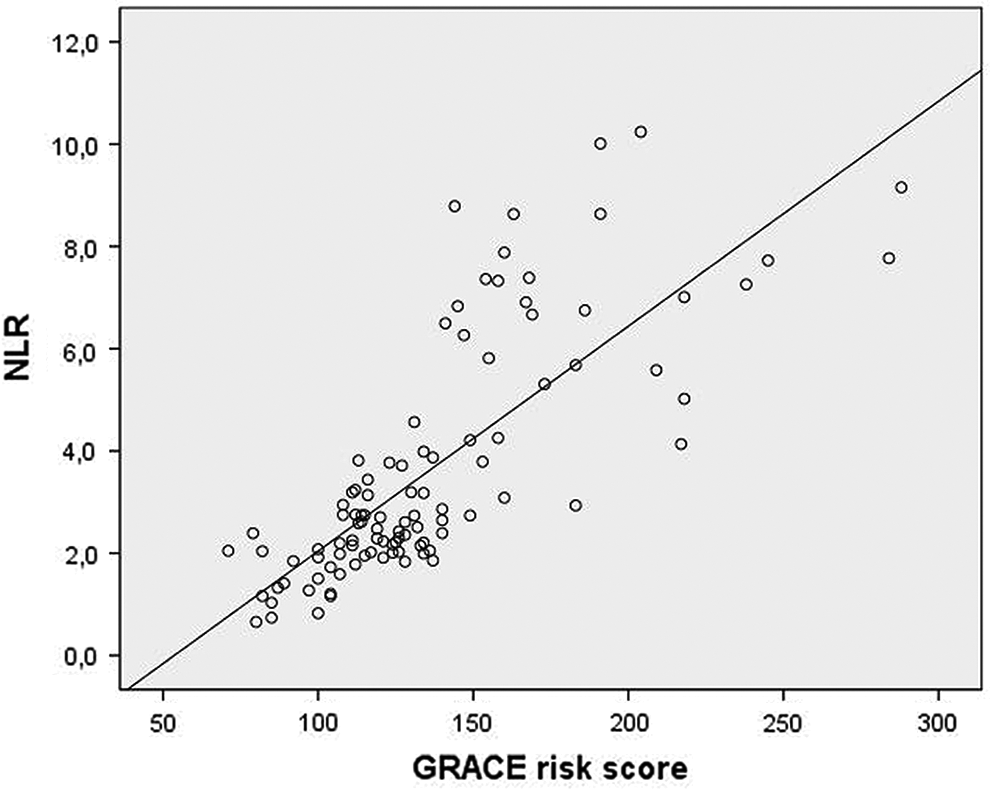
Correlation between neutrophil-to-lymphocyte ratio (NLR) and Global Registry of Acute Coronary Events (GRACE) risk score.
Multivariate Analysis
For in-hospital cardiac events, NLR, mean platelet volume at admission, troponin level at admission, in-hospital GRACE death or MI point, and age were analyzed using a multivariate logistic regression model. The NLR was the only independent predictor of in-hospital cardiac events (odds ratio 3.63, 95% CI: 1.23-10.67, P = .019; Table 3).
Multivariate Logistic Regression Analyses In-Hospital Cardiac Events.
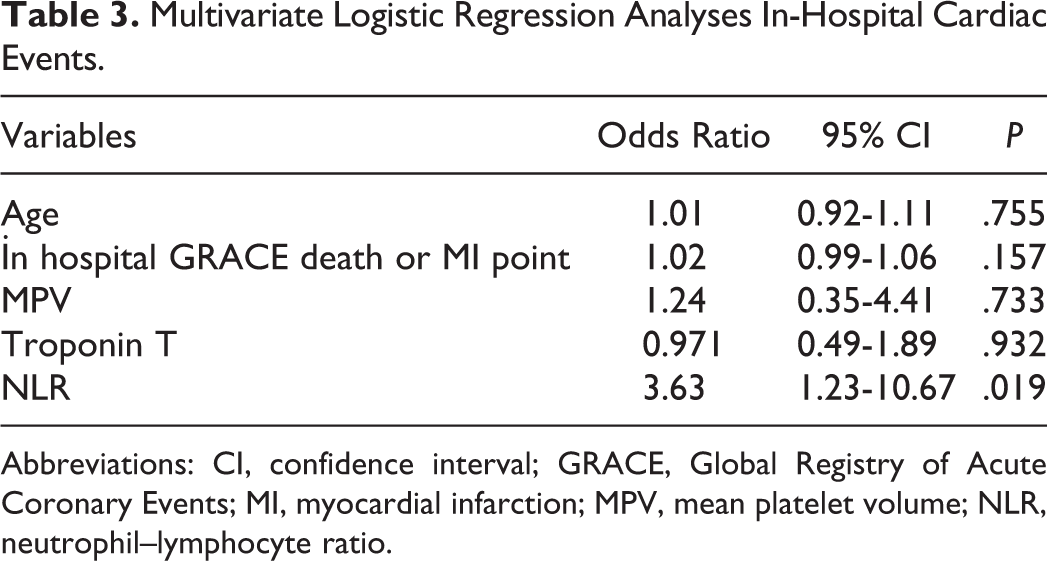
Abbreviations: CI, confidence interval; GRACE, Global Registry of Acute Coronary Events; MI, myocardial infarction; MPV, mean platelet volume; NLR, neutrophil–lymphocyte ratio.
Discussion
Neutrophil-to-lymphocyte ratio has recently emerged as a potential new biomarker, which singles out individuals at risk of future cardiovascular events in patients with STEMI. In our study, we showed that NLR was significantly associated with adverse in-hospital outcomes, independent of GRACE risk score. It is also the first study to correlate the levels of NLR with the GRACE risk score. Our results were in accordance with several previous studies that NLR was a predictor of negative outcome. 10,19,20 In contrast with the results of our study, theirs did not demonstrate a relation with GRACE risk score, which is the most useful tool proposed by clinical guidelines for stratification of patients with acute MI.
Coronary atherosclerosis is the main cause of STEMI. Multiple pathophysiological factors influence this atherosclerotic process, and one of the most important factor is inflammation. 2,21 Inflammatory process that underlines atherosclerosis has a critical role in plaque destabilization and appearence of a thrombus superimposed on the erosion of an atherosclerotic plaque is the mechanism that cause MI. 22
Previous studies showed that WBC count and its subtypes are indicator of systemic inflammation and have an important role in modulating the inflammatory response in the atherosclerotic process. 6,23 In the acute period, leukocyctosis usually accompanies STEMI in proportion to the magnitude of the necrotic process, elevated glucocorticoid levels, and possibly inflammation in the coronary arteries. The magnitude of elevation in the leukocyte count associates with in-hospital mortality after STEMI, and leukocyte subtypes modulate the inflammatory response in this process. 16,20 In particular, neutrophils are the first leukocytes to be found in the dameged myocardial area. Activation of neutrophils produce large amount of inflammatory mediators that have important microcirculatory effects and regulate the inflammatory response to tissue injury. 16 Furthermore, in the previous studies, increased neutrophil count has been independently related to large infarct size, mechanical complication, and mortality in patients with acute MI. 24,25 In an animal study, neutrophil invasion to atherosclerotic plaque has been visualized directly in vivo. 26 It was previously suggested that neutrophils might be associated with the formation of aggregates between platelets and leukocytes in the intravascular lumen, hence even play a pivotal role in determining the infarct extension areas and might facilitate plaque rupture through the release of proteolytic enzymes, arachidonic acid derivatives, and superoxide radicals. Therefore, increased neutrophil count may not only reflect the aggravated inflammation but also play a pathogenic role in the atherosclerotic plaque instability. 27,28 In the acute setting of coronary events, lymphocytopenia is a common finding during the stress response secondary to increased corticosteroids levels. 29 Furthermore, lymphopenia and decreased CD4 counts with inverted CD4–CD8 ratio are correlated with low ejection fraction, high degree of myocardial necrosis, and mortality in patients with acute MI. 30
The NLR is a combination of 2 independent markers of inflammation, neutrophils as a marker of the ongoing nonspecific inflammation and lymphocytes as a marker of the regulatory pathway. 10,31 Unlike many other inflammatory markers and bioassays, NLR is an inexpensive and readily available marker that provides an additional level of risk scores in predicting in-hospital and long-term outcomes. 16
Due to understanding of the important relationship between inflammatory status and adverse outcomes in patients with stable coronary artery disease; several studies focused on NLR and its association with adverse outcomes in patients with ACSs. 9,31,32 Akpek et al demonstrated that preprocedural NLR is an independent predictor of no reflow in patients with STEMI. Neutrophilia can aggravate myocardial ischemia by neutrophil-mediated microvascular plugging and can extend the infarct area. 20 Nunez et al followed patients with STEMI for 4.2 years and evaluated the predictive value of NLR in long-term mortality and found that an increased NLR is associated with an increased risk of long-term mortality. 10 Moreover, Shen et al concluded that NLR is independently associated with long-term mortality in STEMI. 16 In both of these single-center studies; the NLR was measured at admission and following days up to 3 or 4 days. We measured the NLR at admission before starting any medication because leukocyte count and its subytpes (neutrophils and lymphocytes) could be affected by infectious disorders, anxiety, and medication.
The GRACE risk score is a more accurate risk score than other risk scores in stratfying patients according to the probability of adverse outcomes during ACSs. The GRACE risk scores include variables such as hemodynamic status, killip class, cardiac markers, and ST-segment deviation but not inflammatory markers. Correia et al demonstrated that assessment of inflammation improves risk prediction and provides additional prognostic information to the GRACE risk score. 33
Similar to previous studies, our current study has confirmed the relationship between NLR and STEMI. However, there have been no reports on association between NLR and GRACE risk score. In the present study, we showed that NLR was significantly associated with in-hospital adverse cardiac events independent of GRACE risk score. Also, we demonstrated that NLR and GRACE risk score showed a significant positive correlation. Based on our knowlodge, this is the first study to correlate NLR with GRACE risk score.
Study Limitations
The limitations of the present study are as follows. (1) This was a retrospective and single-center study that included a relatively small number of patients. Further studies with a larger sample size may be needed. (2) Only 1 measurement of admission full blood count and calculation of NLR were included in the analysis. (3) We could not compare NLR with other inflammatory markers, such as C-reactive protein, fibrinogen, or myeloperoxidase, because they were not routinely obtained in our study population.
Conclusion
The GRACE risk score is routinely used for stratification of patients with ACS. Our study showed that NLR may provide additional prognostic value in patients with STEMI and increased NLR is associated with in-hospital cardiac events. The determination of NLR for risk stratification of patients with STEMI during hospitalization period may be useful. We think that these significant findings of our analysis can guide for the further clinical practice. However, these findings must be confirmed on a study with larger number of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.