
Abstract
The predictive value of leukocyte counts has been reported in patients with acute myocardial infarction (AMI). We aimed to evaluate the predictive value of the total leukocyte count and neutrophil–lymphocyte (N/L) ratio for mortality due to AMI. A total of 522 patients with acute ST-elevated MI were included in the study. The study population was divided into tertiles based on admission N/L ratio values. High (n = 174) and low N/L (n = 348) ratio groups were defined as patients having values in the third tertile (>5.77) and lower 2 tertiles (≤5.77), respectively. The high N/L ratio group had a significantly higher incidence of in-hospital cardiovascular mortality (13.8% vs 4.6%, P < .001). An N/L ratio >5.77 was found to be an independent predictor of in-hospital cardiovascular mortality (hazard ratio: 3.78, 95% confidence interval: 1.71-8.30, P = .001). A high N/L ratio is a strong and independent predictor of in-hospital cardiovascular mortality of AMI with ST elevation.
Keywords
Introduction
Experimental models of atherosclerosis have demonstrated signs of inflammation in the first stages of lipid accumulation in the artery wall. Blood leukocytes, which mediate host defenses and inflammation, localize to the earliest lesions of atherosclerosis in both experimental animals and humans. Inflammatory processes promote initiation and evolution of atheroma and contribute decisively to acute thrombotic complications of atheroma. 1 The circulating white blood cell (WBC) count is a biomarker with potential utility in cardiovascular risk prediction, 2 because the relationship between the WBC count and the risk of symptomatic or fatal coronary heart disease (CHD) has been found in observational epidemiologic studies.3–11 Further studies have linked an elevated leukocyte count to increased short-term and long-term risks for ischemic events and death in patients with acute coronary syndromes. 12–15 In a previous study with a small number of patients with AMI, we demonstrated that the neutrophil–lymphocyte (N/L) ratio was higher in patients with complications in AMI. 16 In the present study, we aimed to investigate the prognostic value of the N/L ratio for in-hospital mortality in AMI with ST elevation.
Patients and Methods
Study Population
Records of patients with AMI who were admitted to the coronary care unit of Canakkale State Hospital between January 2009 and December 2010 were evaluated retrospectively. A total of 525 patients who were diagnosed with AMI having ST elevation were enrolled in this study. Three patients with intracranial hemorrhage were excluded because of the thrombolytic treatment. A diagnosis of AMI with ST elevation was defined as >30 minutes of continuous typical chest pain and ST-segment elevation ≥2 mm in 2 contiguous electrocardiography leads within 12 hours of the symptom onset or within up to 18 hours if there was evidence of continuing ischemia or hemodynamic instability. The patients’ demographic information, cardiovascular history, and risk factors (smoking, hypercholesterolemia, hypertension [HT], and diabetes mellitus [DM]) were obtained from the medical records. Patients who had been treated with antihypertensive drugs or those whose baseline blood pressure exceeded 140/90 mm Hg were diagnosed with HT. Diabetes mellitus was defined as fasting blood sugar more than 126 mg/dL or the use of antidiabetic medications. Hyperlipidemia was defined as a total cholesterol level >200 mg/dL and/or low-density cholesterol level >160 mg/dL. The admission glomerular filtration rate (GFR) was estimated by the simplified Modification of Diet in Renal Disease equation. 17 Renal failure was defined as a GFR <60 mL/min/m2.
Cardiovascular events during the in-hospital period were investigated from the patient records. Ventricular tachycardia or ventricular fibrillation were defined at least 24 hours after the beginning of the symptoms, advanced heart failure was defined as Killip classification ≥3, and mechanical complications were defined as ventricular septal rupture, free wall rupture, or mitral chordal rupture. Reinfarction was described as the elevation in serum creatine kinase-MB enzyme levels by 2 times the upper limit of normal and ST-segment reelevations. Cardiovascular death was defined as death due to AMI, heart failure, or arrhythmia. The mean follow-up period was 5.7 days.
Analysis of Blood Samples
Complete blood counts and biochemical values were evaluated retrospectively from blood samples obtained by antecubital vein puncture upon admission to the emergency department. Total and differential leukocyte counts were determined with the Beckman Coulter LH 780 (Beckman Coulter Ireland Inc. Mervue, Galway, Ireland) device in the hematology laboratory of Canakkale State Hospital. Other biochemical measurements and electrolyte levels were determined by standard laboratory methods.
Statistical Analysis
The study population was divided into tertiles based on admission N/L ratio values. A high N/L ratio group (n = 174) was defined as having values in the third tertile (>5.77), and a low N/L ratio group (n = 348) was defined as having values in the lower 2 tertiles (≤5.77).
Quantitative variables were expressed as the mean value ± standard deviation, and qualitative variables were expressed as percentages (%). All measurements were evaluated with the Kolmogorov-Smirnov test and were found to be nonnormally distributed. A comparison of parametric values between the 2 groups was performed using the Mann-Whitney U test. Categorical variables were compared by the likelihood ratio chi-square test or Fisher exact test. A backward stepwise multivariate logistic regression analysis that included variables with P < .1 was performed to identify independent predictors of in-hospital cardiovascular mortality. Age ≥70, female gender, DM, HT, renal failure (GFR <60 mL/min/m2), time of chest pain, CHD history, not receiving clopidogrel during the in-hospital period, failed thrombolytic treatment, and N/L ratio >5.77 were entered into the model. A P value <.05 was considered statistically significant. All statistical studies were carried out with the SPSS program (version 15.0, SPSS, Chicago, Illinois).
Results
A total of 522 patients (417 men and 105 women) were enrolled in the present study. No differences were found between the groups regarding sex, thrombolytic and other treatments, tobacco use, HT, hyperlipidemia, DM, family history, and CHD history. Table 1 demonstrates the clinical characteristics of the groups. The patients in the high N/L ratio group were older (63.9 ± 11.8 vs 61.9 ± 11.9, P = .037). Lower triglyceride levels and higher high-density lipoprotein levels were found in the high N/L ratio group. Additionally, baseline total leukocyte count and neutrophil levels were significantly higher in the high N/L ratio group than in the low N/L ratio group (13 787 ± 4324/mm3 vs 10 718 ± 4121/mm3, P < .001; 11 754 ± 3704/mm3 vs 6949 ± 2517/mm3, P < .001), whereas the baseline lymphocyte level was significantly lower in the low N/L ratio group than in the high N/L ratio group (1280 ± 472/mm3 vs 2720 ± 1245/mm3, P < .001; Table 2).
Patient’s Clinical Data, Risk Factors, and Treatments.
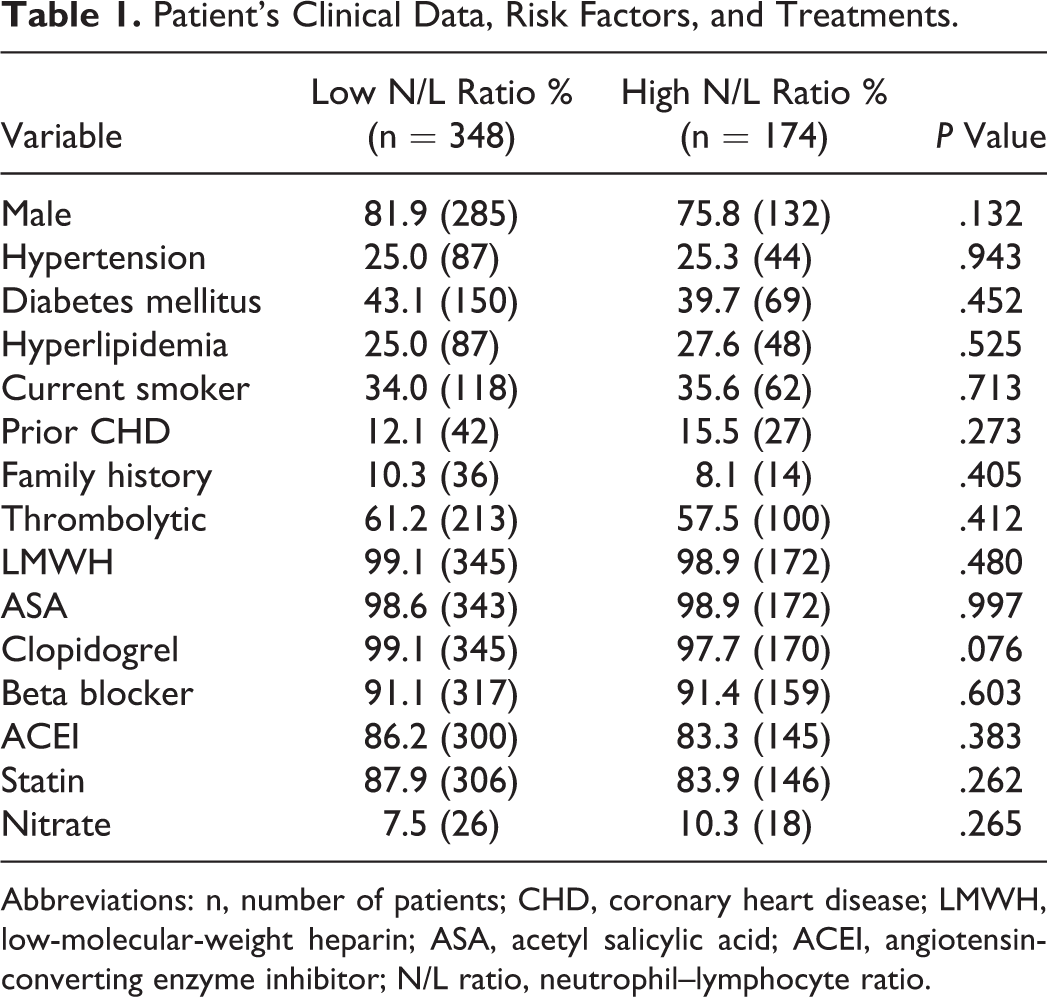
Abbreviations: n, number of patients; CHD, coronary heart disease; LMWH, low-molecular-weight heparin; ASA, acetyl salicylic acid; ACEI, angiotensin-converting enzyme inhibitor; N/L ratio, neutrophil–lymphocyte ratio.
Patient’s Laboratory Findings.
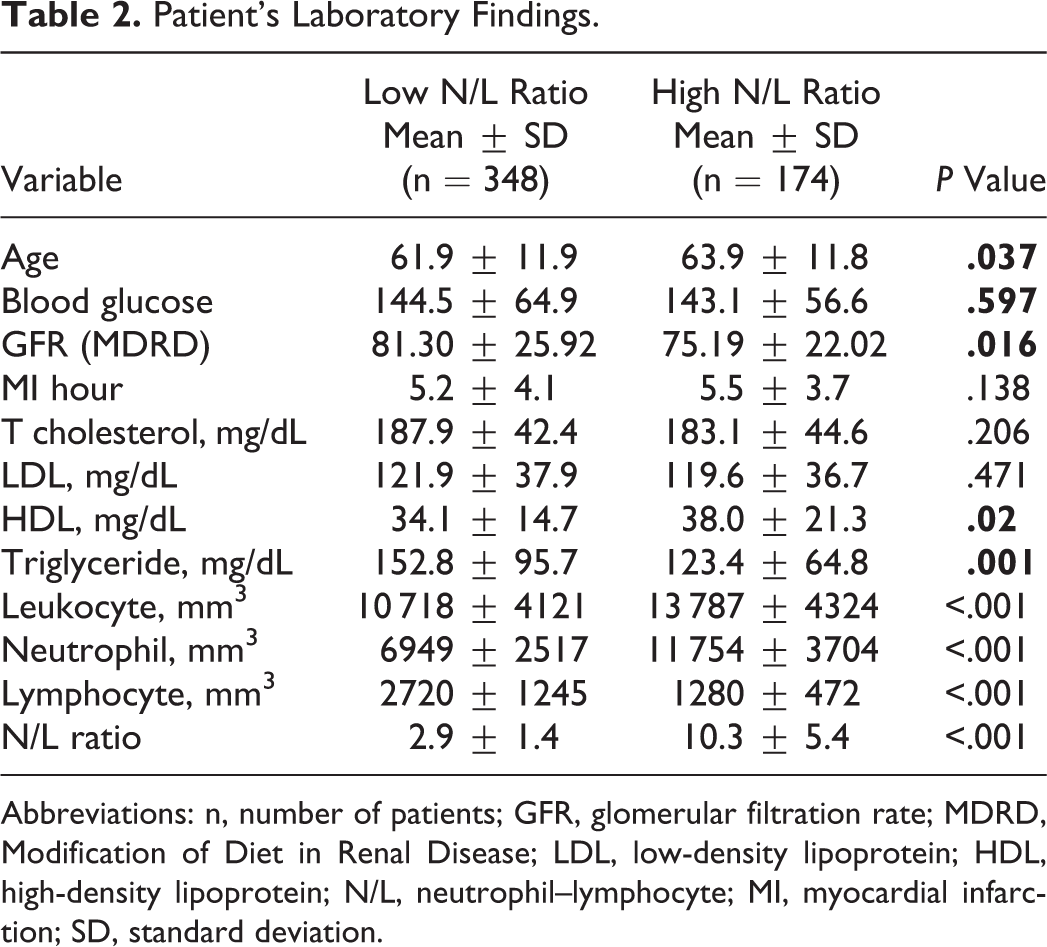
Abbreviations: n, number of patients; GFR, glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein; N/L, neutrophil–lymphocyte; MI, myocardial infarction; SD, standard deviation.
The high N/L ratio group had a significantly higher incidence of in-hospital cardiovascular mortality than the low N/L ratio group (13.8% vs 4.6%, P < .001). Advanced heart failure class >2 was more frequent in patients with high N/L ratio values (12.6% vs 4.9%, P = .001). Other cardiovascular events were not statistically significantly different between the 2 groups (Table 3).
In-Hospital Cardiovascular Events.
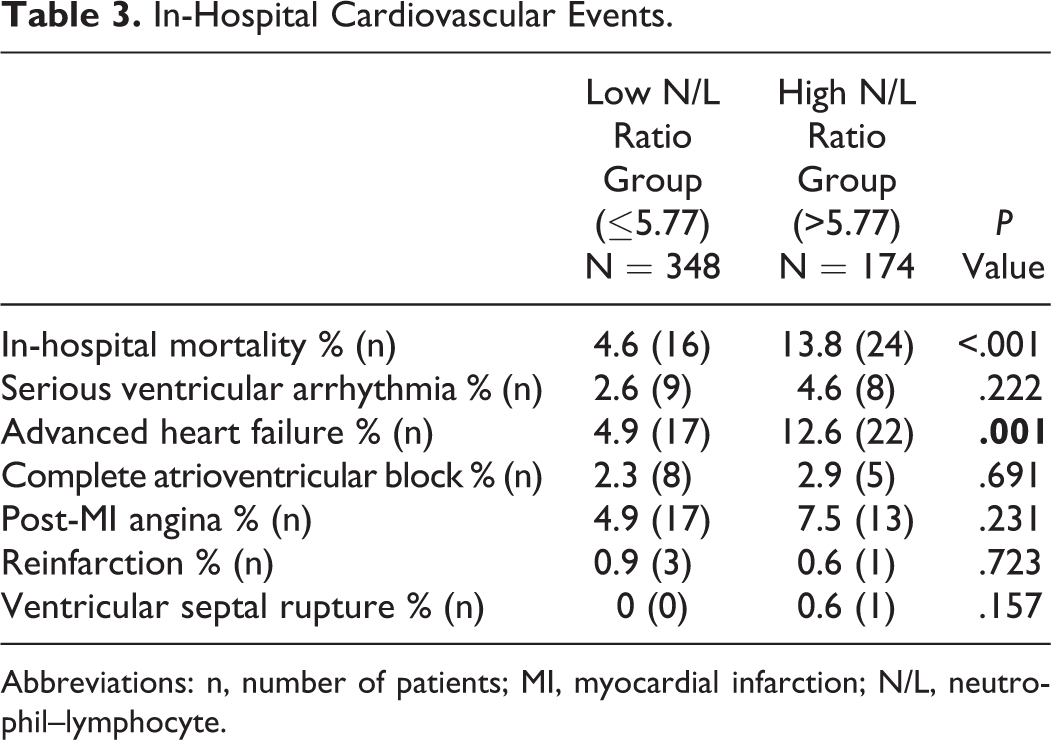
Abbreviations: n, number of patients; MI, myocardial infarction; N/L, neutrophil–lymphocyte.
Independent predictors of in-hospital cardiovascular mortality were determined by a backward stepwise multivariate logistic regression. The HT, DM, CHD history, chest pain duration more than 6 hours, female gender, not receiving clopidogrel during the in-hospital period, failed thrombolytic treatment, renal failure, age ≥70 years, and N/L ratio >5.77 were found to be associated with increased in-hospital cardiovascular mortality in a linear logistic regression analysis (Table 4). An N/L ratio >5.77 was found to be an independent predictor of in-hospital cardiovascular mortality in multivariate analyses (hazard ratio: 3.78, 95% confidence interval: 1.71-8.30, P = .001). Table 5 shows other independent predictors of cardiovascular mortality. In a receiver–operating characteristic curve analyses, an N/L ratio value of 5.77 was determined as an effective cutoff point in AMI with ST-segment elevation of in-hospital mortality, with a sensitivity of 60% and a specificity of 69% (area under the curve = 0.67, 95% confidence interval 0.57-0.76; Figure 1).
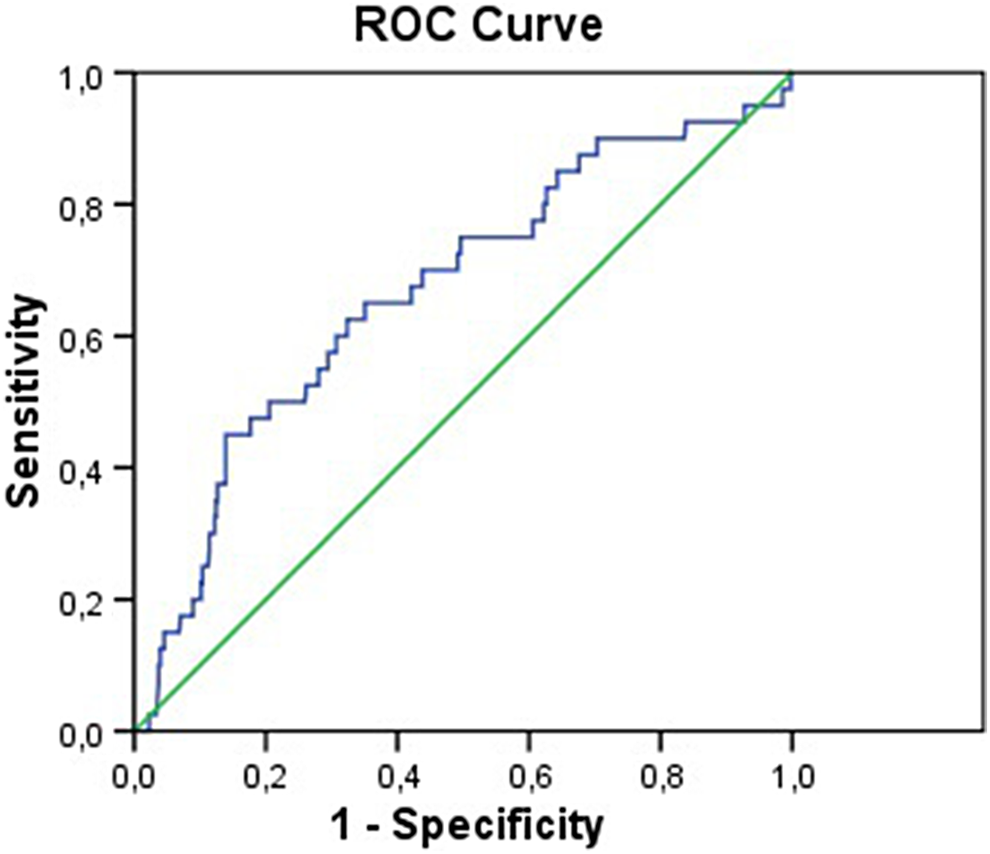
Receiver–operating characteristic curve for the neutrophil–lymphocyte ratio.
Univariate Analyses for Risk Factors of In-Hospital Cardiovascular Events.
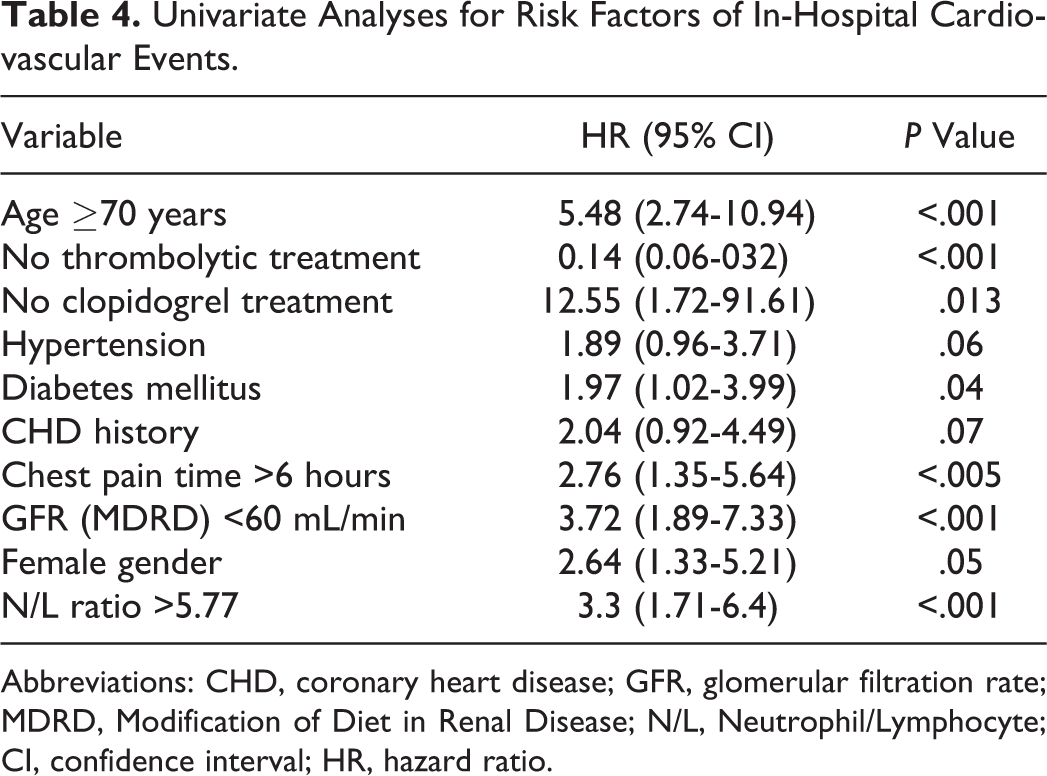
Abbreviations: CHD, coronary heart disease; GFR, glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; N/L, Neutrophil/Lymphocyte; CI, confidence interval; HR, hazard ratio.
Independent Predictors of In-Hospital Cardiovascular Mortality.
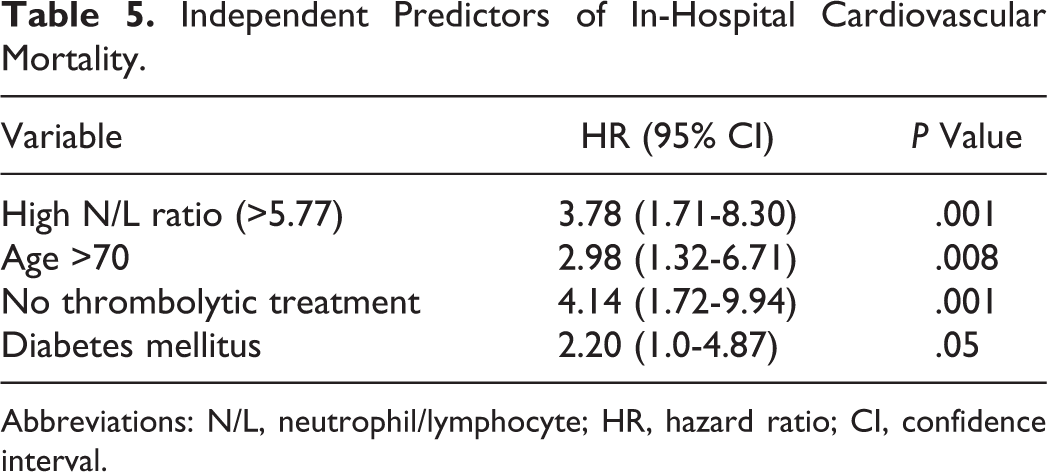
Abbreviations: N/L, neutrophil/lymphocyte; HR, hazard ratio; CI, confidence interval.
Discussion
The present study suggests a relationship between high leukocyte levels and high N/L ratio with in-hospital mortality in AMI with ST-segment elevation. Additional analyses revealed that a high N/L ratio value was associated with increased advanced heart failure in patients with AMI.
The circulating WBC count is a biomarker of potential current utility for cardiovascular risk prediction because of the relationship between WBC count and the risk of symptomatic or fatal CHD. 2 Neutrophils may cause plaque rupture through the release of proteolytic enzymes, superoxide radicals, and arachidonic acid derivates and exacerbate inflammatory condition. Zazula et al 18 reported a cutoff N/L ratio of 5.7, with 35% sensitivity and 91% specificity for a different diagnosis in unstable angina pectoris with noncardiac chest pain. Akin et al 19 reported that higher N/L ratio is associated with severity of coronary artery disease. Furthermore, previous studies linked an elevated leukocyte count with increased short-term and long-term risks of ischemic events and death in patients with acute coronary syndromes. 12–15
It has long been known that myocardial injury is followed by neutrophilia, which is the early appearance of neutrophils within the infarct zone with heavy infiltration by 1 to 3 days, infarct healing, and replacement of fibrosis. It was suggested that enhanced intrinsic reparative processes after MI could be obtained with the use of intracoronary transfer of autologous bone marrow, which is rich in hematopoietic and mesenchymal precursor cells. 20 , 21 On the other hand, neutrophilia might also represent a poor adaptation process in AMI, because the occurrence of circulating leukocyte–platelet aggregates might contribute to vascular plugging and infarct enlargement. 13,22–24
The predictive value of the WBC count has been reported in patients with AMI. Elevated baseline WBC counts are associated with higher short-term mortality. 12–25 Lymphocytes infiltrating the ischemic and reperfused myocardium express interleukin 10 and might play a significant role in healing by modulating the mononuclear cell phenotype and inducing tissue inhibitor of metalloproteinase 1 expression, which plays a dominant role in chronic inflammation. 26 Relative neutrophilia together with lymphopenia is associated with increased cardiovascular risk. 25 Barron et al 12 reported that with increased leukocyte levels, infarct-related artery opening was lower at 60 and 90 minutes after thrombolytic treatment, microvascular perfusion was impaired in patients with ST-segment elevated myocardial infarction (STEMI), and a high leukocyte level is associated with thrombolytic resistance. Núñez et al 27 reported that the maximum value of the N/L ratio is a useful marker to predict subsequent long-term mortality in patients admitted for STEMI, with a discriminative ability that is superior to the maximum total WBC value. Additionally, an elevated preprocedural N/L ratio in patients undergoing percutaneous coronary intervention (PCI) is associated with an increased risk of short- and long-term mortality. 28 , 29 Akpek et al 30 reported that in-hospital mortality and no reflow were increased in patients with STEMI in the presence of an N/L ratio >3.3. Park et al 31 reported that an N/L ratio more than 5.44 have almost 4-fold risk of death during long-term follow-up period in patients with STEMI undergoing primary PCI. Likewise, Shen et al 32 found that the N/L ratio is a strong independent predictor of long-term mortality, median follow-up of 5.2 years after STEMI treated with PCI. In the present study, an N/L value exceeding 5.77 was found to be an independent predictor of in-hospital mortality in patients with myocardial infarction who were given a thrombolytic treatment.
In the Studies of Left Ventricular Dysfunction (SOLVD) trial, the neutrophil count was significantly associated with cardiovascular death, while an inverse relationship was observed between the lymphocyte count and mortality in patients with ischemic and non-ischemic left ventricular systolic dysfunction. 33 In our study, advanced heart failure was more frequent in the high N/L ratio group than in the low N/L ratio group. A similar finding was obtained in the European Prospective Investigation into Cancer (EPIC) study, where an elevated preprocedural neutrophil count was associated with an increased risk of 3 years mortality in patients undergoing high-risk angioplasty. 34 These studies suggest a relationship between the N/L ratio and short-term and long-term mortality in STEMI. Our results extend previous findings by showing that the N/L ratio is a marker of in-hospital mortality in patients with ST-segment elevated AMI. As a conclusion, patients with STEMI and a high N/L ratio might have a higher mortality rate because of thrombolytic resistance and might have a higher incidence of advanced heart failure; therefore, these patients should receive preferential primary or rescue PCI. The present study has some limitations. First, this was a retrospective study. Patient long-term survival and cardiac conditions could not be assessed, because the patient records were not known. Clopidogrel might cause neutropenia, and previous clopidogrel medication could affect the results, but our data were inadequate to assess clopidogrel use. Finally, the coronary angiography results of the patients were not known.
Conclusion
A high N/L ratio is a strong and independent predictor of in-hospital cardiovascular mortality of AMI with ST-segment elevation. Total and differential leukocyte count analyses are routine applications and are simple and inexpensive methods for evaluating patients with AMI. The AMI is the most important cause of mortality and morbidity worldwide. The majority of deaths occur in the first hours of the in-hospital period of AMI. Hence, the N/L ratio together with other inflammatory markers and clinical findings might be helpful to determine high-risk patients and treatment strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.