
Abstract
The aim of this study was to evaluate the relationship between hematologic indices and the Global Registry of Acute Coronary Events (GRACE) score in patients with ST-segment elevation myocardial infarction (STEMI). A total of 800 patients who consecutively and retrospectively presented with STEMI within 12 hours of symptom onset. After accounting for exclusion criteria, a total of 379 patients remained in the study. We enrolled 379 patients with STEMI (mean age 61.7 ± 13.6 years; men 73%). Neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), red cell distribution width (RDW), and monocyte count were associated with increased worse GRACE risk score (P = .008, P = .012, P = .005, P = .022, respectively). In multivariate linear regression analysis, NLR, PLR, RDW, and monocyte count were found to be independent predictors of GRACE risk score. We demonstrate for the first time that PLR, RDW, and monocyte were associated with the GRACE score in patients with STEMI.
Keywords
Introduction
Atherosclerosis is the major cause of cardiovascular disease that still accounts for most of the mortality worldwide. 1,2 Inflammation plays a significant role in initiating atherosclerosis and facilitating its progression. 3 Inflammation characterizes all phases of atherothrombosis, and the presence of inflammation at the site of the atherosclerotic lesion has a critical pathophysiological role in plaque formation and acute rupture. 4,5 The rupture of a vulnerable atherosclerotic plaque and consecutive thrombus formation leads to occlusion of the affected coronary artery followed by necrosis of the subtended myocardial tissue. These events are clinically referred to as acute coronary syndrome (ACS), which includes ST-segment elevated myocardial infarction (STEMI), non-STEMI, and unstable angina pectoris (UAP). 5 White blood cell count (WBC-c) and its subgroups have been investigated as potential inflammatory markers that predict cardiovascular outcomes in patients with coronary artery disease (CAD). 6 –8 The neutrophil to lymphocyte ratio (NLR) is calculated from the WBC-c and is a novel prognostic marker in patients with cardiovascular disease. 9 Platelets are activated to induce thrombosis and acute coronary events through several receptors situated on the platelet surface, between them and receptors for thromboxane, platelet activating factor, histamine, and high affinity and low affinity immunoglobulin E receptors which are known as FC∊ RI and FC∊ RII. The inflammatory mediators that activate the above-mentioned specific receptors are released from eosinophils. That is why eosinophils are related to acute coronary thrombotic events and should be always taken into account. However, eosinophils are pleiotropic multifunctional leukocytes involved in initiation and propagation of inflammatory responses and thus have important roles in the pathogenesis of inflammatory diseases.7,8 Platelet activation is one of the main contributors to the development of ACSs. 10 Platelets are a source of inflammatory mediators. 11 Platelets have a major effect on the formation of atherothrombosis and therefore play an important role in the pathogenesis of ACS. 12 Lymphocytes have been shown to modulate the immunologic response at all stages of the atherosclerotic process. 13 The association between low lymphocyte count and major adverse cardiovascular outcomes was also shown in several studies. 14,15 Recently, the platelet to lymphocyte ratio (PLR) has been proposed to be a novel, prothrombotic and inflammatory marker. 16,17
Red cell distribution width (RDW) is a measurement of erythrocyte variability and size. 18 Recent studies have identified RDW as a predictor of cardiac mortality and systemic inflammation. 19
Monocytes play an important role in inflammation and thrombosis, performing vital functions such as phagocytosis, cytokine production, and tissue repair. 20
The Global Registry of Acute Coronary Events (GRACE) risk scores have a high diagnostic performance for adverse outcomes in ACS and are the preferred scoring system that current European Acute Coronary Syndrome guidelines recommend to apply on admission and at discharge in daily clinical practice. 21
White blood cells and its subtype values are easily measured during routine complete blood count analysis and may be used as cost-effective predictors of inflammation and cardiovascular complications. The relationship between NLR and STEMI has been shown in several studies, but there are little data available about the association of NLR levels with GRACE risk score. Moreover, there are no data available about the association of PLR, RDW, and monocyte count with GRACE score in STEMI. In this study, we aimed to investigate the association of the concomitant hematological indices such as NLR, PLR, RDW, and monocyte count with GRACE risk score in patients with STEMI who underwent primary percutaneous intervention (PCI).
Methods
Study Population and Definitions
A total of 800 patients who consecutively and retrospectively presented with STEMIs and underwent primary PCI within 12 hours of symptom onset between January 2012 and January 2014 were included in the study. The STEMI was defined based on the criteria created by the American College of Cardiology and the European Society of Cardiology 22 : an increase in troponin I >1 ng/mL; a new ST-segment elevation as measured from the J-point in 2 or more contiguous leads from leads V1, V2, and V3 measuring at least 0.2 mV or at least 0.1 mV in the remaining leads during the first 12 hours after symptom onset.
Exclusion criteria of the study were patients with severe liver disease, autoimmune diseases, cancer, hematological disorders, severe valvular disease, inflammatory or infectious diseases, and a history of bleeding diathesis. Patients on the following medications were excluded from the study: corticosteroids, cytotoxic drugs, thrombolytic therapy, and glycoprotein IIb/IIIa inhibitors. If during the study the patient was not treated with primary PCI, did not follow-up for blood work, and had poor echocardiographic windows, then they were also eliminated from the investigation. After accounting for all of these exclusion criteria, a total of 379 patients remained in the study sample.
Demographic data and variables that determine the in-hospital death GRACE risk score points (that include age, creatinine, heart rate, systolic blood pressure, Killip class, cardiac arrest at admission, elevated cardiac markers, and ST-segment deviation) were recorded, 23 and calculation of the GRACE risk score was performed using a computer program (www.outcomes-umassmed.org/grace/acs_risk/acs_risk_content.html). The GRACE risk scores were stratified as low (<108 points), intermediate (108-140 points), and high (>140 points). For each patient, we estimated the risk of in-hospital mortality and coronary events according to GRACE risk score. All patients received a complete physical examination, assessment of coronary risk factors, and medical histories. Presenting clinical symptoms were also recorded. Patients were evaluated for heart failure prognosis according to Killip clinical examination guidelines. 24
Transthoracic 2-dimensional echocardiography was performed upon admission to determine left ventricular ejection fraction (LVEF; Vivid S6, GE Medical Systems, Horten, Norway). All patients underwent selective coronary angiography using the Judkin technique. Primary PCI was performed with the standard femoral approach using a 7F guiding catheter. Coronary vessel disease was defined as greater than 50% stenosis in one of the major coronary arteries. The Gensini scoring system was used to determine the severity of CAD. 25
Laboratory Analysis
On admission, venous blood was obtained from all patients. Hematological indices were measured as part of the automated complete blood count before starting any medication. The NLR was calculated as the ratio of the neutrophils and lymphocytes, both obtained from the same automated blood sample at admission. The PLR was measured by dividing the platelet count by the lymphocyte count. Hematologic indices were measured by an automated hematology analyzer system (Abbott Cell-Dyn 3700; Abbott Laboratory, Abbott Park, Illinois, USA). Absolute cell counts were utilized to perform subsequent analyses.
Statistical Analysis
Statistical analyses were performed using the SPSS software version 18.0 (SPSS Inc, Chicago, Illinois). Categorical variables were summarized as percentages and compared with Pearson chi-square test. Continuous variables were presented as mean ± standard deviation and tested for normal distribution by the Kolmogorov-Smirnov test. Comparison analyses between groups were made using Kruskal-Wallis test and 1-way analysis of variance test where appropriate. Spearman test was used for correlation analysis between hematologic indices and GRACE risk score, gender, LVEF, red blood cell, hemoglobin, RDW, monocyte count, NLR, PLR, and WBC and GRACE point was analyzed using a multivariate linear regression model. Multivariate linear regression analysis was used to assess independent predictors of GRACE risk score and the results were expressed as the odds ratio (OR) with the corresponding 95% confidence interval (95% CI). A P value lower than .05 was considered significant.
The study protocol was reviewed and approved by the Ethics Committee in accordance with the Declaration of Helsinki.
Results
The study population consisted of 379 consecutive patients with STEMI. In all, 72.8% of the patients were male, and the mean age of patients was 61.67 ± 13.59 years. In all, 135 (35.6%) patients had hypertension, 95 (25.1%) patients had diabetes, 19 (5.0%) patients had hyperlipidemia, and 213 (56.2%) patients were smokers. According to the GRACE risk score, 32 (8.4%) patients had low GRACE risk scores, 117 (30.9%) patients had intermediate GRACE risk scores, and 229 (60.7%) patients had high GRACE risk scores.
Demographic and biochemical characteristics of patients in GRACE risk score groups are shown in Table 1. Determination of the GRACE risk score parameters is shown in Table 2. All patients of Killip class III-IV and who had cardiac arrest on admission are in the high GRACE risk score patients group. Peak troponin, creatinine level, and age were the high GRACE risk score patients group.
Demographic and Biochemical Characteristics of Patients in GRACE Risk Score Groups.
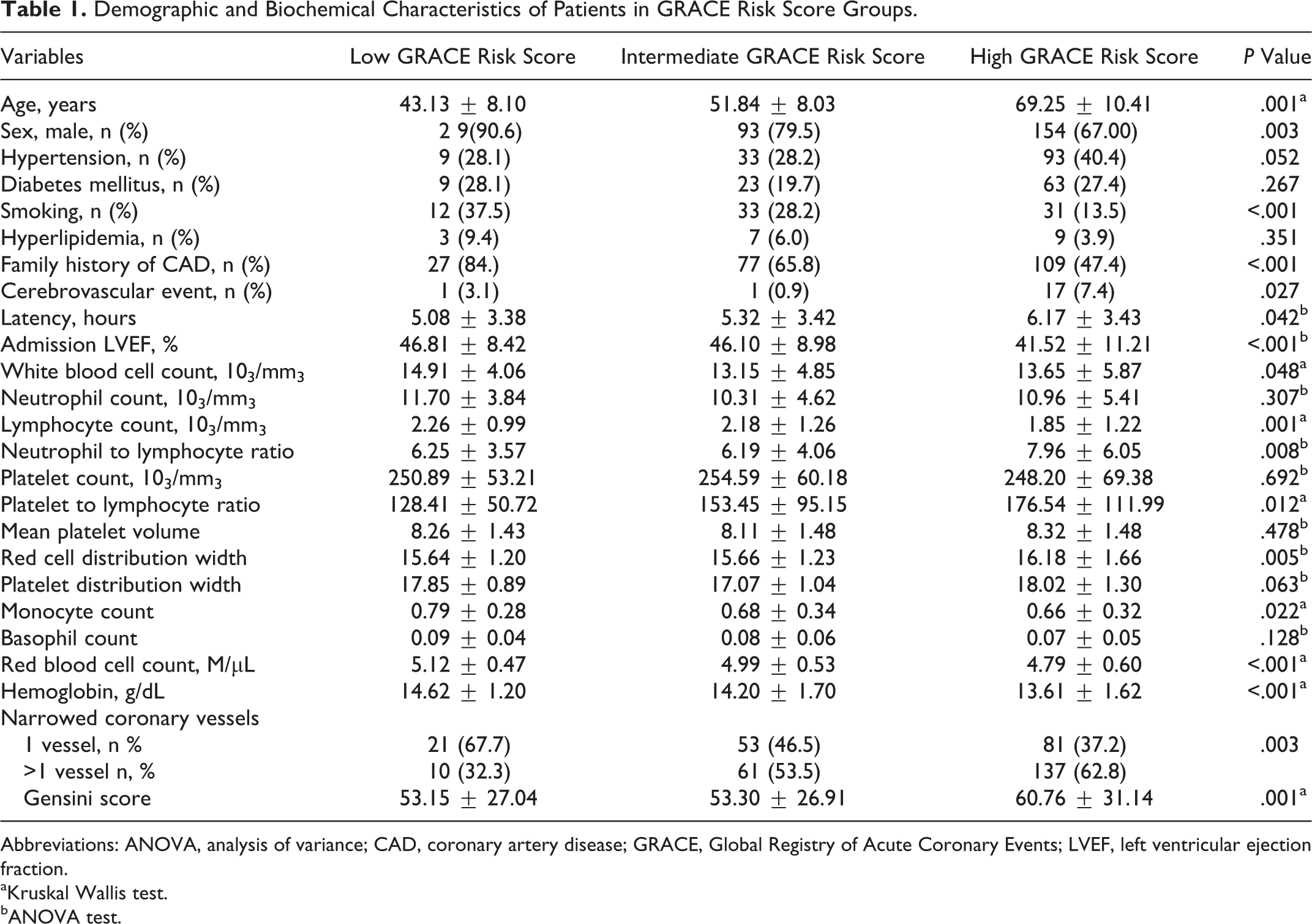
Abbreviations: ANOVA, analysis of variance; CAD, coronary artery disease; GRACE, Global Registry of Acute Coronary Events; LVEF, left ventricular ejection fraction.
aKruskal Wallis test.
bANOVA test.
Determine of the GRACE Risk Score Parameters.
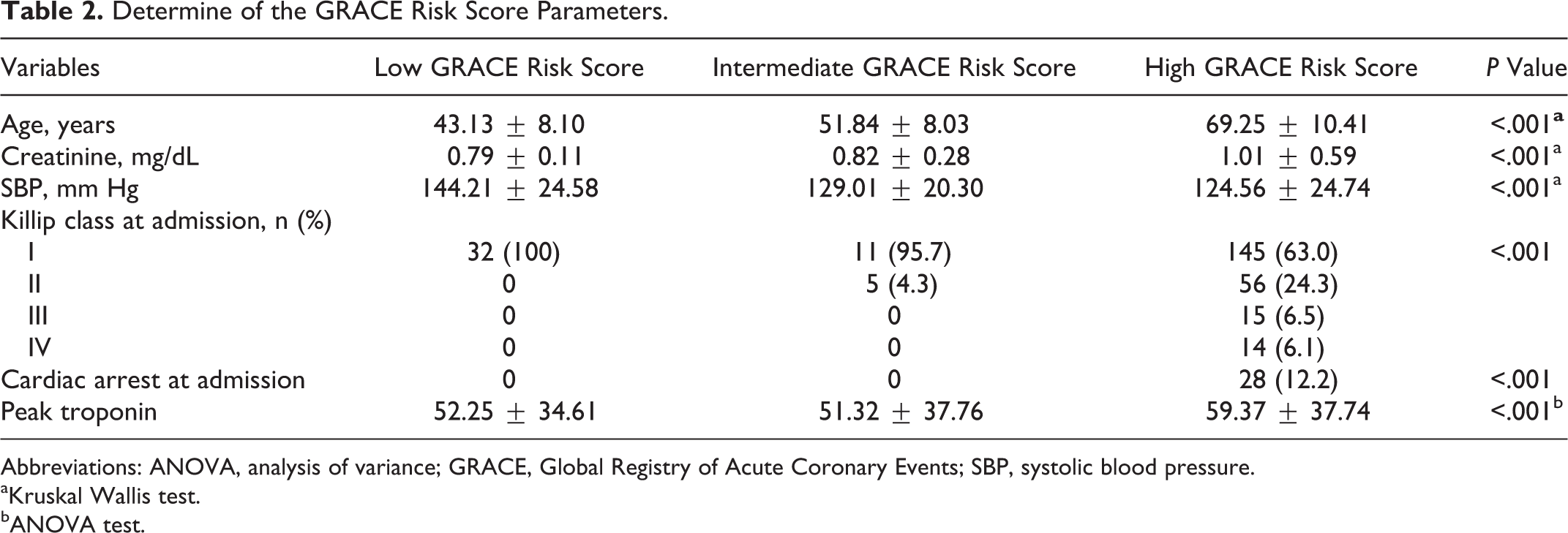
Abbreviations: ANOVA, analysis of variance; GRACE, Global Registry of Acute Coronary Events; SBP, systolic blood pressure.
aKruskal Wallis test.
bANOVA test.
Spearman correlation analysis revealed significant associations between higher GRACE risk scores and NLR (r = .172; P < .001), PLR (r = .110, P = .033), and RDW (r = .173, P = .001; Figure 1). Multivariate linear regression analysis revealed that high measures of NLR and PLR were independent predictors of the GRACE risk score. Higher NLR values were associated with GRACE risk score (b = 1.200, 95% CI = 0.034-2.367, P < .001), higher PLR (b = 0.073, 95% CI 0.132-0.014, P = .016), RDW (OR b = 2.167; 95% CI = 0.170-4.164, P = .034), WBC (b = 0.989, 95% CI = 0.277-1.702, P = .007), and monocyte count (b = −10.722, 95% CI = −20.678 to −0.766, p = .035). A multivariate linear regression analysis for the relationship between GRACE score and other variables is shown in Table 3.
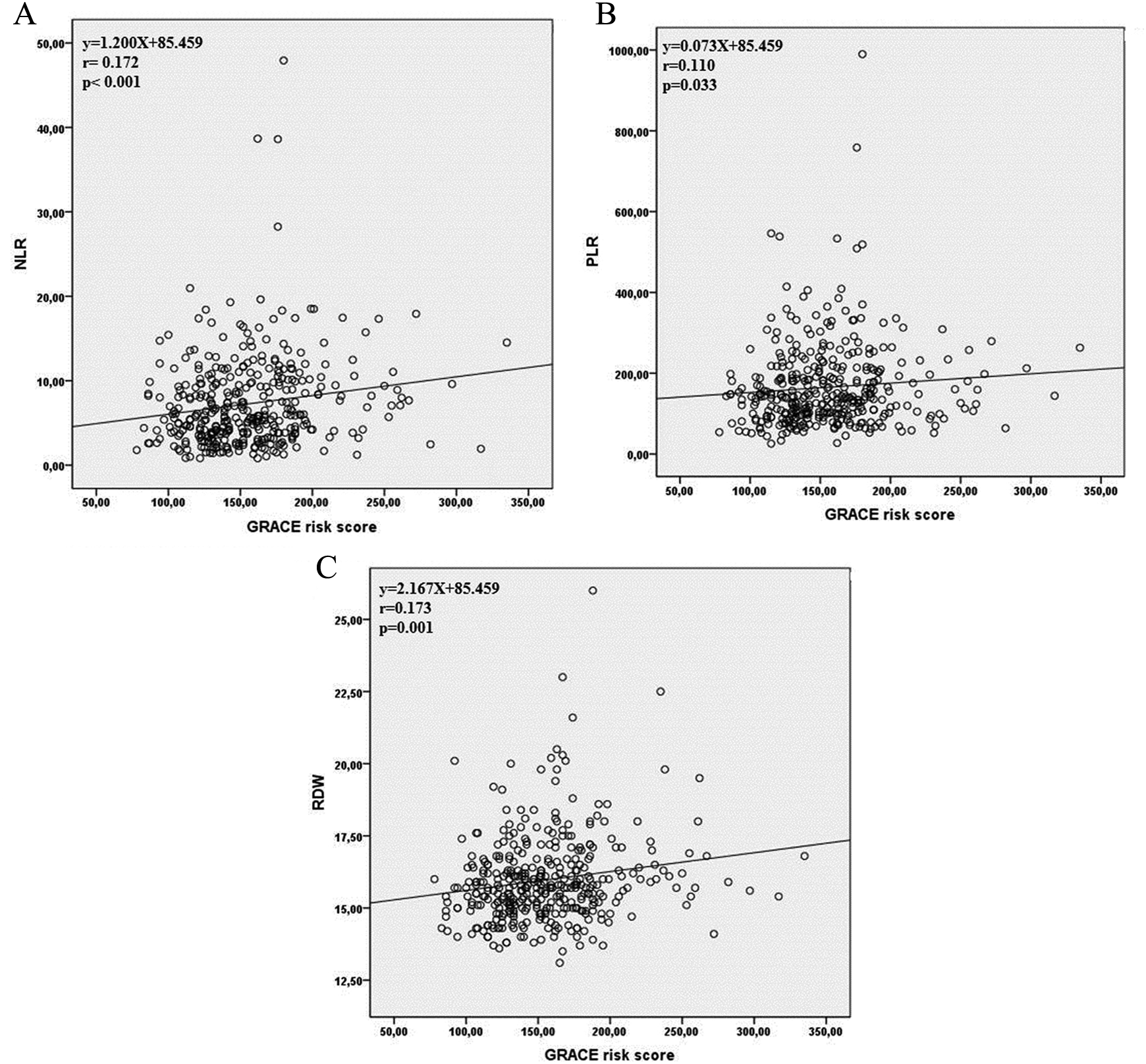
A, Correlation between NLR and GRACE risk score. B, Correlation between PLR and GRACE risk score. C, Correlation between RDW and GRACE risk score. NLR indicates neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; RDW, red cell distribution width; GRACE, Global Registry of Acute Coronary Events.
Independent Predictors for In-Hospital GRACE Death by Multivariate Linear Regression Analysis.
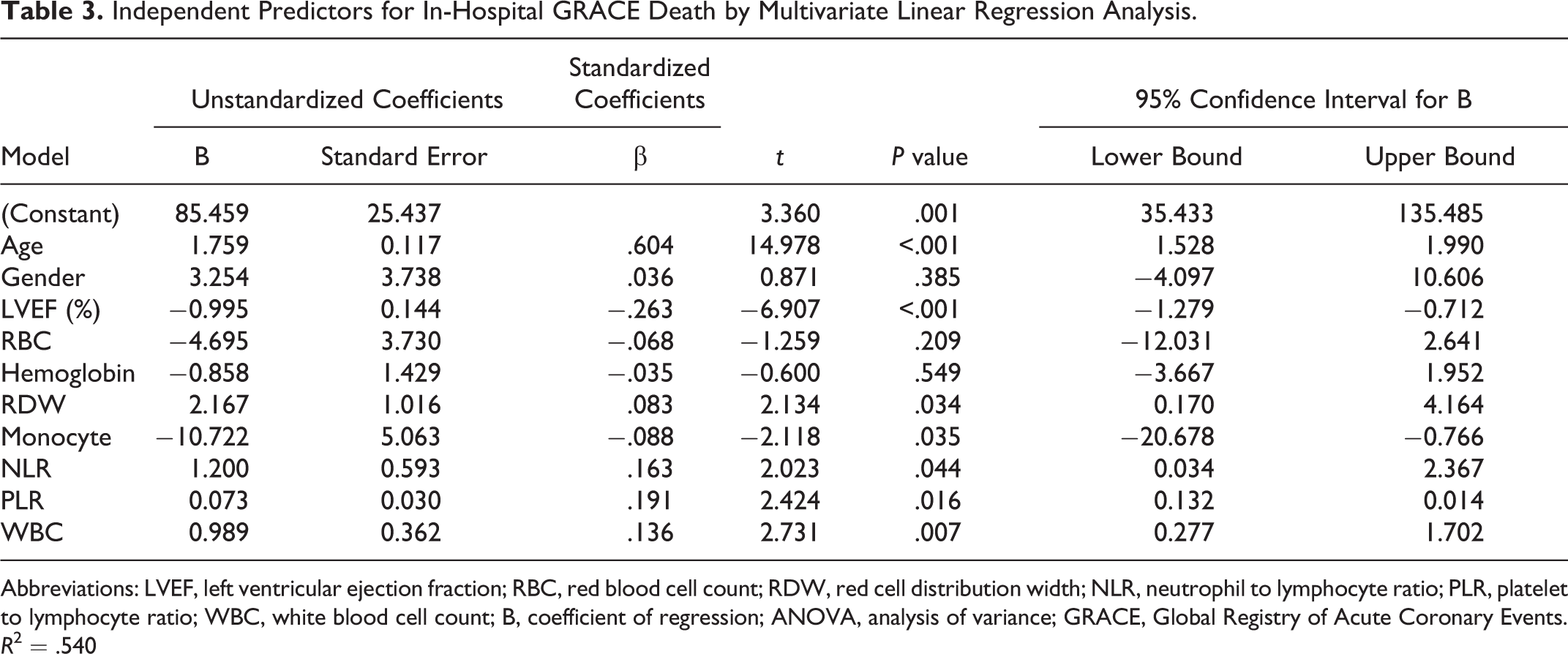
Abbreviations: LVEF, left ventricular ejection fraction; RBC, red blood cell count; RDW, red cell distribution width; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; WBC, white blood cell count; B, coefficient of regression; ANOVA, analysis of variance; GRACE, Global Registry of Acute Coronary Events. R 2 = .540
Discussion
Coronary atherosclerosis is the main cause of STEMI. Multiple pathophysiological factors influence this atherosclerotic process, and one of the most important factors is inflammation. 4,26 The inflammatory process that underlines atherosclerosis has a critical role in plaque destabilization and appearance of a thrombus superimposed on the erosion of an atherosclerotic plaque; this is the mechanism that can cause myocardial infarction (MI). 27
The GRACE risk scores include variables such as hemodynamic status, Killip class, cardiac markers, and others but do not include inflammatory markers. The GRACE score has been recognized as a validated predictor of adverse cardiovascular disease events in patients with cardiovascular disease (CVD). 28
Platelets are produced by megakaryocytopoiesis 29 and play an important role in the pathogenesis of ACS. 12 Platelet to lymphocyte ratio has been proposed to be a novel, prothrombotic and inflammatory marker. 16,17 Neutrophil to lymphocyte ratio is a novel prognostic inflammatory marker. 9 A strong correlation between RDW with inflammatory markers, C-reactive protein, and sedimentation rate has also been observed. 19 Monocytes play important roles in cardiovascular disease, and their actions can be both beneficial (angiogenesis or cardiovascular repair) and detrimental (excessive inflammatory response). However, hematologic indices such as NLR, PLR, RDW, and monocyte count are not included into the GRACE scoring system. Correia et al 30 demonstrated that assessment of inflammation improves risk prediction and provides additional prognostic information to the GRACE score. However, there have been no reports on the association between PLR, RDW, monocyte, and GRACE risk score in patients with STEMI. In the present study, we showed that hematologic indices such as WBC-c, NLR, PLR, RDW, and monocytes were significantly associated with GRACE risk score. Also, we demonstrated that WBC, NLR, PLR, RDW, and monocytes were independent predictors of worse GRACE risk score. Based on our knowledge, this is the first study to correlate concomitant hematologic indices such as WBC, NLR, PLR, RDW, and monocytes with GRACE score in patients with STEMI.
Platelet to Lymphocyte Ratio and GRACE Risk Score
Platelets play a central role in the development of ACS, 31 which is caused by complex interactions between leukocytes and platelets causing the production of reactive oxygen species contributing to ischemic endothelial damage. 32 Proliferating megakaryocytes and relative thrombocytosis are consequences of an ongoing inflammatory response that contributes to a prothrombotic state in ACS. Prior studies have demonstrated that a low lymphocyte count in patients with acute MIs and chronic CAD gives information about worse prognosis. 33 Platelet to lymphocyte ratio is derived from the number of platelets and lymphocytes and it is accepted as a new inflammatory marker. 17,34,35 However, the advantage of PLR is that it reflects both coagulation and inflammatory pathways and may be superior to individual platelet or lymphocyte counts. More recent studies have stated that higher platelet and lower lymphocyte counts may play a major role in adverse cardiovascular outcomes. Azab et al reported that higher PLR values were associated with increased long-term mortality in non-STEMI patients. 34 Sunbul et al found that the PLR was a significant predictor of nondipper status in patients with hypertension. 36 Gary et al revealed that increased PLR is significantly associated with patients at high for critical limb ischemia. 37 Yildiz et al show that high preprocedural PLR and NLR levels are significant and independent predictors of no reflow in patients undergoing primary PCI. 38 Açar et al investigated the relationship between the PLR and the coronary collateral circulation (CCC) in 294 patients with stable angina pectoris and chronic total occlusion. They demonstrated that the PLR values were higher in patients with poor CCC than in those with good CCC. Furthermore, it was found that PLR is an independent predictor of poor CCC. 39 In addition to the prognostic significance, the PLR has also been demonstrated in patients with various cancers. 40 In a relatively recent study in patients with small cell carcinoma of the esophagus, PLR was proven to be superior to NLR in terms of relapse-free survival and overall survival. 41 However, to the best of our knowledge, the relationship between the PLR and the GRACE risk score in patients with STEMI undergoing primary PCI has not been investigated before. Our results demonstrate for the first time that the GRACE score and PLR at baseline are significantly correlated. Moreover, PLR was determined to be an independent predictor of worse GRACE risk score.
Red Cell Distribution Width and GRACE Risk Score
Red cell distribution width is a measurement of variability and size of erythrocytes. 18 Increased RDW has been reported to be associated with negative clinical outcomes in patients with heart failure, MI, and stable CAD, independent of hemoglobin values. 42–44 Uyarel et al 45 demonstrated that higher admission RDW levels in patients undergoing PCI for STEMI were associated with increased risk of in-hospital and long-term cardiovascular mortality. Polat et al 46 investigated the relationship between RDW and GRACE risk score in 193 small patients with UAP/non-STEMI. They demonstrated that high RDW was an independent predictor of high GRACE score, and it is associated with in-hospital mortality in UAP/non-STEMI. However, the relation between the RDW and the GRACE score in patients with STEMI has not been investigated. Our results demonstrate for the first time in patients with STEMI that the GRACE score and RDW at baseline are significantly correlated. Moreover, RDW was an independent positive predictor of worse GRACE risk score in patients with STEMI.
Monocyte Count and GRACE Risk Score
Monocyte aggregation with platelets is accompanied by monocyte activation, resulting in increased cytokine production, expression of cell adhesion molecules, and the release of matrix metalloproteinases. 47 Even in the absence of platelet interaction, monocytes play an important role in inflammation and thrombosis, performing vital functions such as phagocytosis, cytokine production, and tissue repair 20 as well as being a major source of blood tissue factor. 48 Also, a recent study demonstrated increased monocyte numbers in patients with stable systolic heart failure. 49 Wrigley et al showed that significant upregulation of monocyte–platelet aggregates occurs in patients with ischemic heart failure. 50 Monocytes play important roles in cardiovascular disease, and functional status in cardiac disorders is still poorly understood. The specific role of monocytes in hospital mortality is largely unknown. Moreover, the relationship between monocyte count and GRACE risk score in patients with STEMI has not been investigated before. Our results demonstrate for the first time that the GRACE risk score and monocyte count are related. In this study, monocyte levels are decreased in patients with increased GRACE risk score. Moreover, monocyte count was an independent negative predictor of GRACE risk score.
Neutrophil to Lymphocyte Ratio and GRACE Risk Score
White blood cell count and its subtypes may indicate inflammation associated with CVD. 51 In patients with ACS, neutrophils become functionally activated and mediate the destabilization of atherosclerotic plaques. 52 Recent studies have shown that high neutrophil counts are associated with poorer angiographic outcomes, larger infarct sizes, and worse prognosis in patients with STEMI. 53 –55 Several studies have demonstrated that NLR is a marker of cardiovascular disease prognosis. 56,57 Previous studies focused on NLR and its association with adverse outcomes in patients with ACSs. 58,59 Akpek et al demonstrated that preprocedural NLR is an independent predictor of no reflow in patients with STEMI. 53 Núñez et al 54 followed patients with STEMI and evaluated the predictive value of NLR in long-term mortality and found that an increased NLR is associated with an increased risk of long-term mortality. In both of these studies the NLR was measured at admission and 3 to 4 days for follow-up. We measured the hematologic indices at admission before starting any medication because WBC-c, its subtypes, and platelets could be affected by infectious disorders, anxiety, and medication. To our knowledge, only 1 study by Oncel et al has investigated the relationship between NLR and GRACE risk score. 60 They investigated the relationship between NLR and GRACE score in 101 patients with STEMI. They showed that NLR was a positive predictor of GRACE score. In our study, we also found that high NLR was significantly increased with GRACE risk score. In sum, we showed that patients having STEMI with GRACE score had significantly high NLR, PLR, RDW, and monocyte count. This suggests that PLR, NLR, RDW, and monocytes may be indicators of GRACE risk score in patients with STEMI.
Study Limitations
The limitations of the present study were a retrospective design and single-center experience. We could not compare NLR, PLR, and RDW with other inflammatory markers, such as C-reactive protein, fibrinogen, or myeloperoxidase because they were not routinely obtained in our study population. However, a major limitation of the study is that our results do not give an idea about the relationship between hematologic parameters and clinical outcome.
Conclusion
The GRACE risk score is routinely used for stratification of patients with ACS. Our study showed that hematological indices such as NLR, PLR, RDW, and monocyte count may provide additional prognostic value in patients with STEMI. The determination of these hematologic indices for risk stratification of patients with STEMI during the hospitalization period may be useful. We think that these significant findings of our analysis can guide further clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.