
Abstract
Aim:
The pathophysiology of cardiac syndrome X (CSX) has not been clearly identified, although multiple abnormalities including microvascular spasm, endothelial dysfunction, and atherothrombosis have been reported. It is known that eosinophils play an important role in vasoconstruction and thrombosis. We aimed to compare the eosinophil counts in patients with CSX versus controls. Materials and
Methods:
This study included 50 patients with CSX (20 male, mean age 50.42 ± 9.6 years) and 30 control persons (10 male, mean age 49.16.11 ± 9.2 years). These participants underwent concurrent routine biochemical tests, and their eosinophil counts were obtained on whole blood count. These parameters were compared between groups.
Results:
Baseline characteristics of the study groups were comparable. Patients with CSX had a higher eosinophil count and mean platelet volume (MPV) value than the controls (339.4 ± 188 vs 132.7 ± 75 and 8.8 ± 0.2 vs 7.2 ± 0.1 fL; P < .001, respectively).
Conclusion:
As a result, our study revealed a relationship between eosinophil count and MPV in patients with CSX.
Introduction
The characteristic features of cardiac syndrome X (CSX) are angina with exertion, ST-segment depression on treadmill exercise testing or pathological thallium scan and normal coronary arteriography, and no spontaneous or inducible epicardial coronary artery spasm on ergonovine or acetylcholine provocation. 1
Although the exact mechanisms leading to CSX are not clear up to now, atherothrombosis, endothelial dysfunction, and vasospasm are suggested as the possible responsible factors. 2
It is known that eosinophils play an important role in endothelial dysfunction, vasoconstriction, inflammation, and thrombosis. 3,4 Eosinophils stimulate the activation and aggregation of platelets. Moreover, they ease the formation of thrombosis via inhibition of thrombomodulin. 5 –7
The powerful vasoconstrictor and procoagulant effects of eosinophils made us hypothesize that there might be a correlation between eosinophil concentration and CSX. As far as we know, there is no study performed until today about the association of blood eosinophil concentration with CSX. In our study, we compared eosinophil counts between patients with CSX and control groups.
Materials and Methods
The CSX group consisted of 50 patients (20 male, mean age 50.42 ± 9.6 years). The diagnosis of CSX was based on the presence of a typical exercise-induced angina pectoris associated with transient ischemic ST-segment depression (>1 mm) during the treadmill exercise with angiographically normal coronary arteries in the absence of coronary artery spasm (determined by hyperventilation maneuver). The control group consisted of 30 age- and sex-matched individuals (10 male, mean age 49.16 ± 9.2 years) with anginal chest pain but a normal coronary angiography, without any sign of inducible ischemia on treadmill exercise test.
Physical examination, medical history of patients, blood biochemistry, and transthoracic echocardiographic examination were evaluated in both groups to exclude systemic diseases. Patients with obstructive coronary artery disease, chronic renal failure, chronic liver disorders, chronic lung disease, moderate or severe valvular disease, diabetes mellitus, hypertension, congenital heart disease, left ventricular systolic dysfunction on echocardiography (ejection fraction < 50%), recent acute coronary syndrome, anemia, pregnancy, obstructive sleep apnea, hematological disorders, known malignancy, thyroid dysfunction, hypercholesterolemia, electrolyte imbalance, and drug history included antigout agent, anti-inflammatory agent (steroid or nonsteroid), antiaggregan or anticoagulant agents, antihistaminic, and any medication that can potentially interfere with the measurement of eosinophil counts were excluded from the study. Also patients who had a recent history of an acute infection and/or high body temperature (>38°C), an inflammatory, or an allergic disease are excluded from the study.
The patients having a systolic blood pressure ≥140 mm Hg and/or a diastolic blood pressure ≥90 mm Hg and those taking antihypertensive drugs were considered to be hypertensive.
Cardiac Catheterization
Coronary angiograms were performed with a femoral approach using the Judkins technique without the use of nitroglycerin, adenosine, or calcium channel blocker. All patients in the study population underwent elective coronary artery angiography using Siemens Axiom Artis DFC (Siemens Medical Solutions, Erlangen, Germany) following appropriate patient preparation. Coronary angiograms were judged with regard to smooth appearance, luminal wall irregularities, epicardial local or diffuse caliber reduction, and stenosis.
Coronary arteries were classified as normal based on the visual assessment of the absence of any luminal irregularities.
To exclude the possibility of coronary artery vasospasm, during coronary arteriography, the patients with normal coronary artery underwent a hyperventilation test that was performed by asking the patients to breathe quickly and deeply for 5 minutes.
Laboratory Tests
Biochemical parameters were analyzed spectrophotometrically on ArchitectC16000 autoanalyzer (Abbott, Abbott Laboratories, IL, USA) using enzymatic colorimetric assay.
For whole blood count (eosinophil count, hematocrit, hemoglobin, mean corpuscular volume, mean platelet volume [MPV], leukocytes, and platelets), the blood samples were collected in tubes with EDTA and analyzed on CELL-DYN 3700 (Abbott Diagnostics, Santa Clara, CA, USA) device using impedance and optic scatter method.
Statistical Analysis
The SPSS 16.0 statistical program (SPSS Inc, Chicago, Illinois) was used for statistical study. All values are expressed as mean ± standard deviation. Mean values of continuous variables were compared between the groups using the Student t test or Mann-Whitney U test, according to whether normally distributed or not, as tested by the Kolmogorov-Smirnov test. A P value of less than .05 was considered significant.
Results
By evaluating the basic clinical and demographic characteristics, it was found that there was no statistically significant difference between the 2 groups in terms of age, gender distribution, body mass index, smoking status, and biochemical parameters (Table 1).
Comparison of Basic Clinical and Biochemical Features of Patients and Controls.
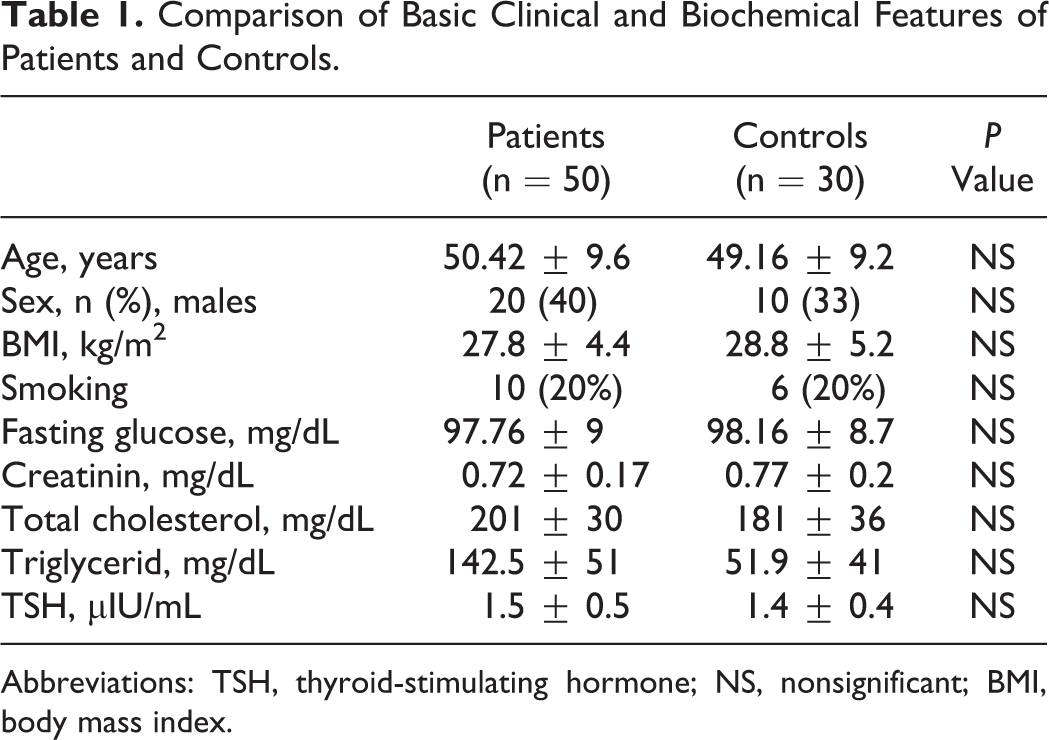
Abbreviations: TSH, thyroid-stimulating hormone; NS, nonsignificant; BMI, body mass index.
In the group of patients with CSX, blood eosinophil count, and MPV value, which were tested simultaneously in blood samples, were significantly higher than that in the control group (P < .001). There was no statistically significant difference between the 2 groups with regard to leukocyte count, platelet count, hemoglobin, and hematochrit level (Table 2).
Comparison of Whole Blood Count Features in Patients and Controls.
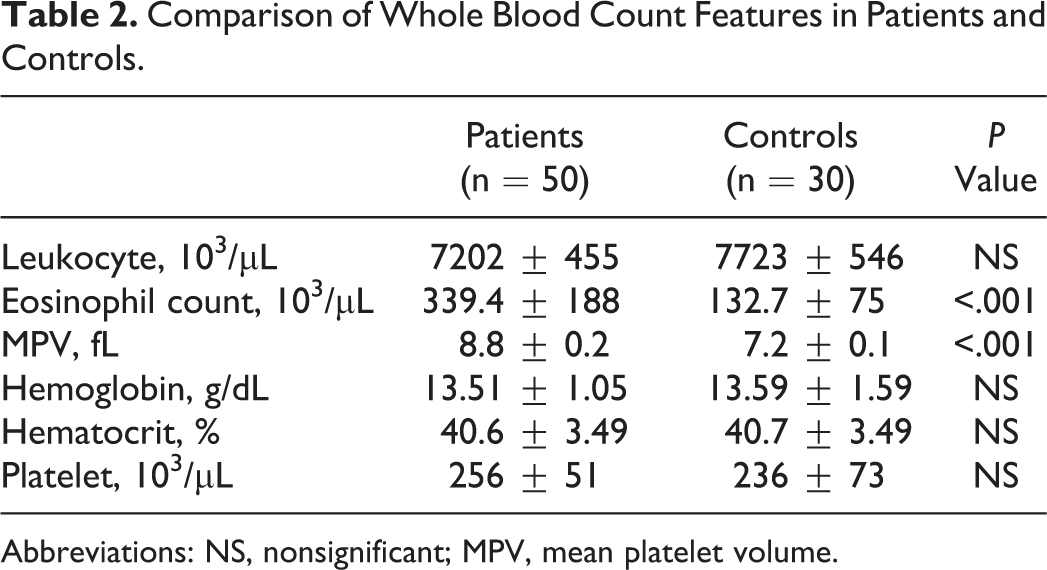
Abbreviations: NS, nonsignificant; MPV, mean platelet volume.
Discussion
In our study, we have found significant differences in eosinophil count and MPV between patients with CSX and control group.
The pathophysiology of CSX has not been clearly identified yet, although multiple abnormalities including abnormal coronary flow reserve, inflammation, abnormal autonomic control, abnormal cardiac sensitivity, microvascular spasm, endothelial dysfunction, oxidative stress, and atherothrombosis, have been reported. 8
Previous studies have demonstrated that high-sensitivity C-reactive protein (hs-CRP) and white blood cell (WBC) count were higher in patients with CSX than in control participants. The increased levels of hs-CRP and WBC count may suggest that these markers may be used in clinical practice for the assessment of the inflammatory status of CSX. 9 –11
As far as we know, there is no study available in the literature about the association between CSX and eosinophil count.
Eosinophils activate coagulation system and platelets, and they also cause vasopasm such as coronary artery spasm. Umemoto et al reported that peripheral eosinophil counts were significantly higher in patients with severe coronary spasm than that in nonspasm patients. They also speculated that eosinophil count could predict vasospastic angina pectoris. 12 Erdoğan et al reported a significantly higher eosinophil counts in patients with angina pectoris than that in controls. 13 Additionally, eosinophils play a role in myocarditis and heart failure. 14
The present study showed that blood eosinophil count and MPV value are higher in patients with CSX than that in the controls.
In our study, we have found significant differences in MPV between patients with CSX and control group. Also, our findings are consistent with those of Çay et al. 15 Additionally, when 2 groups were compared in our study, the eosinophil count of the patients having CSX was significantly higher than that in controls.
Eosinophils are equipped with several granule-associated molecules that play a role in the occurrence of thrombosis and vascular injury. Eosinophils generate an increased tendency to thrombosis through leukocyte, platelet stimulation, and release of tissue factor. 16 –19 All these effects contribute to procoagulation through preventing the activation of thrombin and formation of endorsing fibrin. Eosinophils store and release tissue factor as well as other cationic proteins. Major basic protein, eosinophilic cationic protein, activates platelets and promotes thrombus formation by inhibiting thrombomodulin in hypereosinophilic syndromes and allergic diseases. 20,21 Sakai et al demonstrated that large thrombus has greater eosinophil counts both in thrombi and in peripheral blood. They also speculated that thrombus growth might be facilitated in patients with higher eosinophil counts in the peripheral blood. 22
Eosinophils cause pulmonary and systemic vasoconstriction via the peroxidase–hydrogen peroxide–halide system. Activated eosinophils and secreted eosinophil granule proteins were most evident within the necrotic and later stage thrombotic lesions and were found mainly within the areas of acute tissue damage in the endocardium and in the walls of small blood vessels. These findings suggest that eosinophil granule proteins are involved in vascular injury, and eosinophils may also affect cardiovascular system through inflammatory cell infiltration. 12,23
Recent studies showed that eosinophils were associated with stent thrombosis, stent restenosis, and acute coronary syndromes. Furthermore, it was reported that elevated serum eosinophil concentration might be responsible for cardiac mural thrombus and embolic events. 24 –26 Also Keçeoğlu et al speculated that higher eosinophil count is related to left atrial thrombus in patients with atrial fibrillation. 27
The powerful vasoconstrictor and procoagulant effects of eosinophils made us hypothesize that there might be a correlation between eosinophil concentration and CSX. In the literature, there is no study investigating the association between CSX and eosinophils. Our study is of importance with regard to this matter, we investigated the effect of eosinophil concentration in patients with CSX.
The most important limitation of our study is the limited number of patients. Another limitation was the possibility of any underlying coronary artery spasm in patients with CSX, which was excluded using a hyperventilation test, although the ergonovine test would have been the ideal test in this contest. Another specific test were not performed in controls to exclude any evidence of myocardial ischemia. Further studies are required to determine the relation between eosinophil count and CSX.
In conclusion, our results may contribute to etiopathogenesis of CSX and pathophysiological mechanisms of increased prevalence of cardiovascular morbidity and mortality risk in these patients. Increased concentration of eosinophil in patients with CSX might be due to vasoconstriction and thrombosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.