
Abstract
Aim: To investigate the relationship between mean platelet volume (MPV) and in-hospital deep venous thrombosis (DVT). Material and methods: 147 patients with the diagnosis of DVT and 149 control participants were included in the study. For all participants, clinical risk factors, smoking status, and other demographic data were recorded from hospital registries. The data of patients with DVT were compared with the control participants. Results: Mean MPV was significantly higher in patients with DVT than the control group (8.91 ± 1.86 vs 7.86 ± 0.9; P < .001). Body mass index, smoking frequency, hematocrit, and platelet count were significantly correlated with MPV. Independent predictors of in-hospital DVT were MPV (odds ratio [OR] = 1.5; 95% confidence interval [CI] = 1.2-1.87; P ≤ .001), body mass index (OR = 1.17; 95% CI = 1.04-1.34; P = .012), and smoking (OR = 1.83; 95% CI = 1.09-3.08; P = .023). Conclusion: Mean platelet volume was significantly higher in patients with DVT, and it is an independent predictor of in-hospital DVT.
Introduction
Venous thromboembolism, including deep venous thrombosis (DVT) and pulmonary embolism, is a common disease, with important complications, and may cause lethal outcome. 1 The annual incidence is approximately 1 to 3 per 1000 adults in developed countries.1,2 Surgery, hospitalization, immobilization, trauma, malignancy, pregnancy, use of contraceptives containing estrogens, and inherited thrombophilia have shown to be associated with DVT events.3,4
Platelets have a central role in the pathogenesis of thromboembolic disease. Platelet size has been shown to reflect platelet activity. Large platelets are metabolically and enzymatically more active than small platelets and produce more thromboxane A2, express more glycoproteins lb and llb/llla receptors. 5 Increased values of mean platelet volume (MPV) have been recognized as an independent risk factor for stroke. 6 Moreover, increased MPV was associated with poor clinical outcome in survivors of myocardial infarction 7 and with the severity of acute ischemic cerebrovascular events. 8 However, in a recent study, MPV is not associated with severity or outcome in patients with acute ischemic stroke. 9 Mean platelet volume is a useful and easy tool for indirect monitoring of platelet activity in different situations. Recently, increasing levels of MPV were identified as a predictor for venous thromboembolism of unprovoked origin. 10 All these data revealed that MPV may have a central role in both arterial and venous thrombosis. However, the relation between platelet indices and in-hospital DVT has not been studied before. Therefore, the aim of this study was to investigate the relation between MPV, platelet count, and in-hospital DVT.
Materials and Methods
Study Population
This observational, retrospective study was conducted in Dicle University Medicine Faculty Hospital. A total of 147 consecutive patients (65 men and 82 women) who had been hospitalized to the Dicle University and were diagnosed with DVT between February 2006 and December 2010 were enrolled. Inclusion criteria included the following: (1) hospitalized patients between the ages of 20 and 80; (2) the patients who had received appropriate DVT prophylaxis if necessary; and (3) being diagnosed as DVT with clinical findings and duplex ultrasonography or venography. Exclusion criteria were as follows: (1) presence of hematological malignancies; (2) use of oral anticoagulants; (3) use of oral contraceptives; (4) hospitalization with the diagnosis of DVT; and (4) presence of a history of previous DVT. One hundred forty-nine (81 men and 68 women) participants who had undergone routine checkup procedure in the family medicine department and who had no known diseases were recruited as the control group. For all participants, clinical risk factors, smoking status, and other demographic data were recorded from hospital registries. Provoking factors for DVT were as follows: surgery (26%), immobilization (33%), malignancy (21%), and acute medical condition (20%).
Body mass index (BMI; kg/m 2 ) was calculated from self-reported heights (m) and weights (kg). Deep vein thrombosis was diagnosed with the use of venous duplex ultrasonography in 90% of the patients. Venography and spiral computed tomography were used in the rest.
Complete blood count samples which were drawn into vacutainer tubes containing 0.04 mL of the 7.5% K3 salt of EDTA were analyzed within 1 hour after sampling with a commercially available analyzer (CELL-DYN 3700; Abbott Diagnostics, Abbott Park, Illinois). The Institutional Review Board of the Dicle University Faculty of Medicine approved the study, a waiver of consent was granted and patient identity was protected. The local ethics committee has also approved the study.
Statistical Analyses
All values are given as mean ± standard deviation. SPSS V.15 was used for analysis. The Kolmogorov-Smirnov test was applied for a normal distribution. The unpaired Student t test was used for group comparisons. Categorical data were compared with the chi-square test. Logistic regression analysis was applied to identify which variables had an independent relationship with in-hospital DVT. A P value of <.05 was considered significant.
Results
Characteristics and demographic findings of the study population were shown in Table 1 . All parameters had a normal distribution. Mean MPV was significantly higher in patients with DVT than the control group (8.91 ± 1.86 vs 7.86 ± 0.9; P < .001). Body mass index and smoking frequency were higher in patients with DVT, whereas hematocrit and platelet count were significantly lower.
Demographic and Clinical Features in Patients With DVT and Control Group
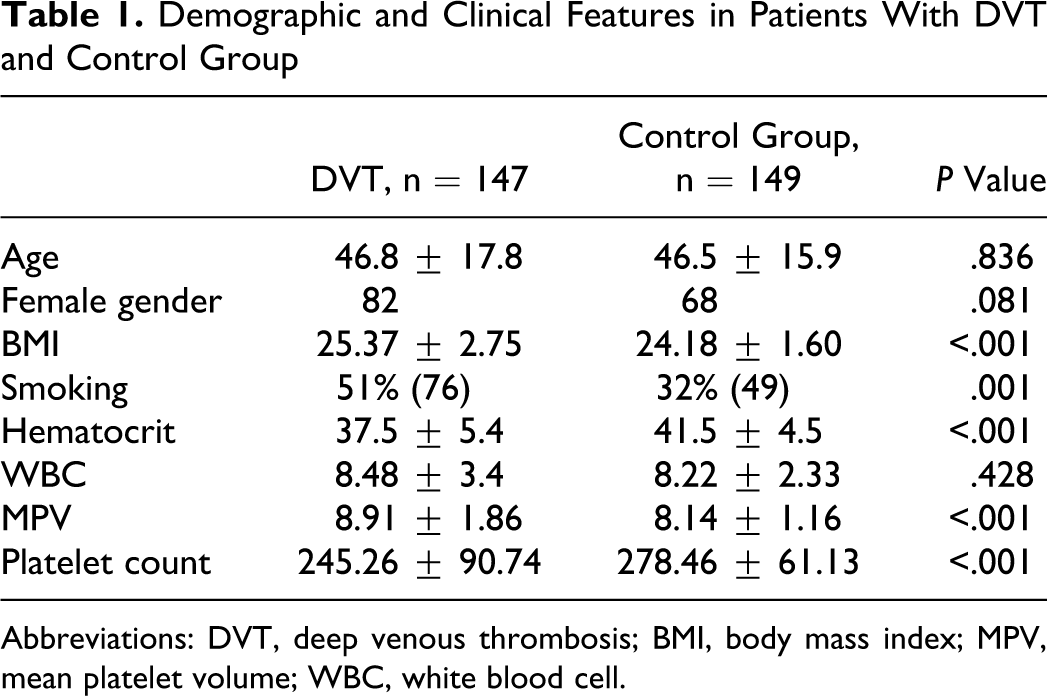
Abbreviations: DVT, deep venous thrombosis; BMI, body mass index; MPV, mean platelet volume; WBC, white blood cell.
Body mass index, smoking frequency, hematocrit, and platelet count were significantly correlated with MPV (Table 2 ).
Correlation Analysis of Mean Platelet Volume and Clinical Variables
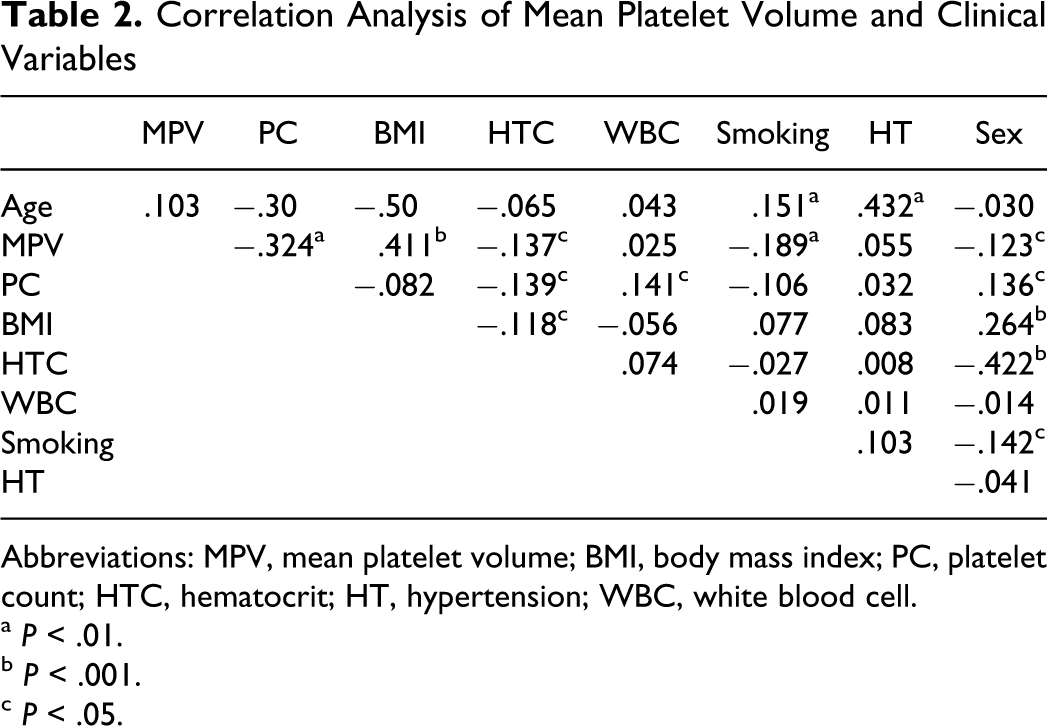
Abbreviations: MPV, mean platelet volume; BMI, body mass index; PC, platelet count; HTC, hematocrit; HT, hypertension; WBC, white blood cell. a P < .01. b P < .001. c P < .05.
Independent predictors of in-hospital DVT were analyzed with logistic regression analysis (Table 3 ). The analysis showed that MPV (odds ratio [OR] = 1.5; 95% confidence interval [CI] = 1.2-1.87; P ≤ .001), BMI (OR = 1.17; 95% CI = 1.04-1.34; P = .012), and smoking (OR = 1.83; 95% CI = 1.09-3.08; P = .023) were independent predictors of in-hospital DVT.
Independent Predictors of In-Hospital Deep Vein Thrombosis by Logistic Regression Analysis
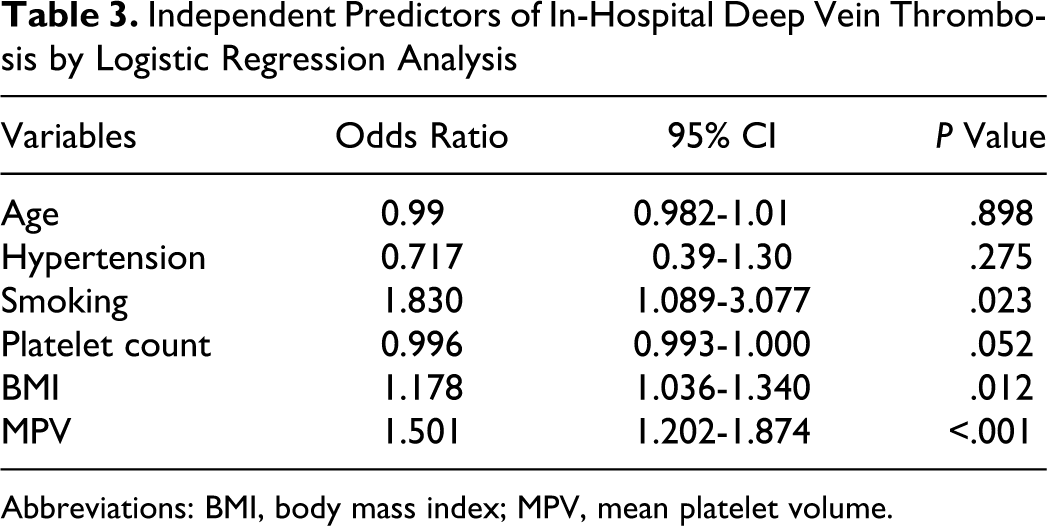
Abbreviations: BMI, body mass index; MPV, mean platelet volume.
Discussion
The present study showed that MPV is an independent predictor of in-hospital DVT. Deep vein thrombosis is an important problem especially in hospitalized patients. It leads to lethal complications such as pulmonary embolism. In a recent study, it was shown that high MPV increases the risk of unprovoked venous thromboembolism independently. 10 Our study further adds an insight into the potential role of higher MPV in DVT established during hospital stay.
Concordant with the previous studies, present results showed that there was a negative correlation between MPV and platelet count.11 -13 The human organism tends to keep constant the platelet mass, which is the mathematical product of platelet count and platelet volume. As a result, reductions in the platelet count are compensated by increasing the MPV.12,13 Other correlates of MPV were also well established. Kario et al showed that MPV value was significantly higher in smokers in patients with and without atherosclerosis. 14 Furthermore, MPV values decreased at the normal levels after 1 to 3 months of smoking cessation. Coban et al also demonstrated that MPV levels of the obese patients are significantly higher than nonobese patients, independent of other cardiovascular risk factors. 15 There was a positive correlation between MPV and BMI. On the other hand, Varol et al have found higher MPV values in patients with hypertension (HT) compared to their normotensive counterparts. 16 These data were also concordant with our findings.
Our results showed that BMI and smoking are associated with in-hospital DVT. Previous studies have shown that risk of venous thromboembolism increases with BMI, female gender, and the presence of HT and smoking. In the National Hospital Discharge Survey Study, the risk of DVT was higher in obese females compared to male patients (2.72- vs 2.02-fold). 17 In another case–control study, obesity was found as a risk factor for venous thromboembolism. 18 In a recent prospective study, BMI, smoking, female gender, and high diastolic blood pressure (>100 mm Hg) were related to increased thrombotic risk. 19 However, MPV was not analyzed as a risk factor for thromboembolism in these studies. On the other hand, platelet count was investigated in depth. In the LITE study, in which 19 293 patients were followed for a mean of 7.8 years prospectively, elevated platelet count was not associated with increased risk of VTE. 20 However, Simanek et al showed that platelet count was related with increased venous thromboembolism in patients with cancer. 21 Monreal et al also showed that low platelet count was associated with increased pulmonary embolism. 22 In the present study, we could not show any relation between in-hospital DVT and platelet count.
Results of this study suggested that increased MPV independently predicts DVT established during hospital stay. However, several important points should be highlighted. Clinical validity of MPV is closely related with the time. Platelets swell in EDTA, with an increase of 7.9% within 30 minutes and an overall increase of 13.4% over 24 hours, but the majority of this increase occurs in the first 6 hours. 23 Citrate and EDTA were compared for the point of highest stability. It was shown that platelets swell until 120 minutes in EDTA and until 60 minutes in citrate and an optimal measuring time of 60 minutes after venipuncture was recommended. 24
Limitations of the Study
The study was retrospective and was conducted on a limited number of patients. Mean platelet volume measurement may yield slightly different results according to the type of automated analyzer used.25,26 Therefore, the results of the current study need to be confirmed in other studies using different automated analyzers. Control group was not sex matched. In conclusion, MPV was significantly higher in patients with DVT, and it is an independent predictor of in-hospital DVT.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.