
Abstract
In this prospective review of cancer screening in unselected patients with unprovoked venous thromboembolism (VTE) presenting to a large teaching hospital in the Republic of Ireland, we aimed to determine the effects of the implementation of the National Institute for Health and Care Excellence screening policy in a “real-world” population. Within our institution, 64 individuals presented with unprovoked VTE during the study period, of whom 47 underwent a screening computed tomography (CT) scan. Two cases of previously undiagnosed cancer were identified. However, in both cases, the clinical history provided by the affected individuals would have prompted a CT scan regardless of the recommendations of the screening policy. The screening CT scans identified 18 incidental lesions within the cohort, which required further diagnostic studies. None of the additional investigations completed to date have detected any lesion of clinical significance. These findings support the view that cancer screening with CT imaging in unselected individuals with unprovoked VTE is not justified or cost-effective.
Introduction
For decades, the complex interplay between cancer and blood coagulation has represented a major focus of clinical and scientific interest. 1 Cancer has been shown to promote coagulation activation, a process normally restricted to sites of vascular injury through various pathological mechanisms. 2 –4 Interestingly, emerging evidence also suggests that the products of coagulation activation, such as the serine proteases thrombin and activated coagulation factor X, may themselves support cancer dissemination through mechanisms that have yet to be fully elucidated. 1,2
Given the nature of the cross talk between malignant tumors and the hemostatic system, it is not surprising that coagulation activation is frequently implicated in cancer-related morbidity and mortality. 5,6 Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), frequently complicates the care of patients with cancer and represents a leading cause of cancer-associated death. 5,7,8 Moreover, it is well recognized that a symptomatic VTE is frequently the first manifestation of an otherwise occult malignant tumor and that a cancer diagnosis is often preceded (in some cases by months or years) by an otherwise idiopathic VTE event. A number of investigators have estimated that an occult malignancy is subsequently diagnosed in up to 10% of patients presenting with unprovoked thrombosis. 9 –11
In view of the potential for idiopathic VTE to herald the diagnosis of cancer, and given the clear benefits of early cancer detection, the development of effective cancer screening strategies for patients presenting with idiopathic VTE could potentially be of significant clinical benefit. Guidelines published by the UK National Institute for Health and Care Excellence (NICE) in 2012 (taking into account the limited evidence base at the time in this area) recommended a pragmatic approach to screening in this clinical scenario. Specifically, this guideline document recommended that patients with idiopathic VTE be offered a physical examination, basic blood tests (including full blood count [FBC], serum calcium, and liver function tests), urinalysis, and chest radiograph (CXR). In addition, NICE recommended that a computed tomography (CT) scan of the abdomen and pelvis be considered for all patients aged more than 40 years. 12
Although this approach was widely adopted into clinical practice, the resource implications of these recommendations are considerable. Computed tomography scanning is a costly investigation, and the availability of testing is limited in many health services, including within the Republic of Ireland. In addition, this imaging modality is not without risk and is known to impart a dose of ionizing radiation as well as potentially exposing patients to further invasive procedures or further imaging studies in the event of unexpected incidental findings being detected, such as asymptomatic benign lesions of limited clinical significance. 13
Moreover, the impact of extensive cancer screening with CT scanning on cancer-related mortality was unknown until recently, with the publication of the results of the Screening for Occult Malignancy in Patients with Idiopathic VTE (SOME) study. This randomized controlled trial comprised a cohort of over 800 patients with idiopathic VTE who were randomized to undergo either limited screening (physical examination, basic blood tests, CXR, and gender-specific testing if not carried out in the previous year, eg, mammography) or limited screening in addition to a comprehensive CT of the abdomen and pelvis. The investigators reported an overall incidence of cancer diagnosis of 3.9% within the cohort within 1 year of follow-up but, importantly, demonstrated no difference in the rates of cancer detection, time to cancer detection, or in the overall mortality between the 2 groups. These results suggest that extensive screening for malignancy with CT among patients with idiopathic VTE is not warranted. 14
The aim of the present study was to determine the number of occult malignancies detected as a result of the current screening policy among patients presenting with unprovoked VTE within our institution.
Methods
This study was an analysis of prospectively collected data pertaining to consecutive patients presenting to the emergency department (ED) of a large, city center, academic teaching hospital in Dublin City Center (Mater Misericordiae University Hospital [MMUH]) between March 26, 2014, and November 11, 2015, who were diagnosed with VTE. Patients presenting to the MMUH ED and diagnosed with a new VTE are managed according to a structured care pathway (under the governance of the multidisciplinary MMUH VTE Committee). For the purposes of this study, only patients presenting with PE or proximal lower limb DVT were included for review (cases with distal lower limb DVT or superficial thrombophlebitis were excluded). Within this cohort, the VTE event was considered to have been unprovoked if it occurred in the absence of a history of a specific risk factor known to be associated with an increased thrombotic risk. These risk factors included a history of a known active malignancy or other active medical illness associated with an increased thrombotic risk (eg, inflammatory bowel disease), pregnancy/estrogen therapy, and recent major surgery or prolonged periods of immobilization (within the preceding 3 months). At the time of this study, this pathway recommended a CXR, blood tests including FBC, liver profile, bone profile, and lactate dehydrogenase, and urinalysis for patients with unprovoked VTE in addition to the history and physical examination. Moreover, it was recommended that women greater than 40 years should undergo mammography and that men greater than 40 years should undergo prostate-specific antigen testing, prostate examination, or both. Finally, the pathway recommended consideration of CT of the abdomen and pelvis (CT-AP) (and thorax if CT pulmonary angiography was not performed to rule out a PE) in all patients with unprovoked VTE.
In this study, data were prospectively recorded at the time of diagnosis via the ED in a local hospital database. We determined whether a clear provoking factor for the VTE event existed. For patients without a VTE provoking factor, we determined the frequency of testing and the outcomes of cancer-specific CT-AP.
Results
A total of 92 997 patients presented to the MMUH ED during the study period. Of these, 170 were diagnosed with VTE; 106 (62.3%) were found to have had provoked VTE, with 64 (37.7%) found to be unprovoked. Other patient characteristics are outlined in Table 1. Of the 64 unprovoked cases, 47 (73.4%) underwent CT-AP (including a CT of the thorax in patients who had not previously undergone CT pulmonary angiography), the outcomes of which are described in Table 2.
Characteristics of Patients Presenting to the Emergency Department With a VTE.
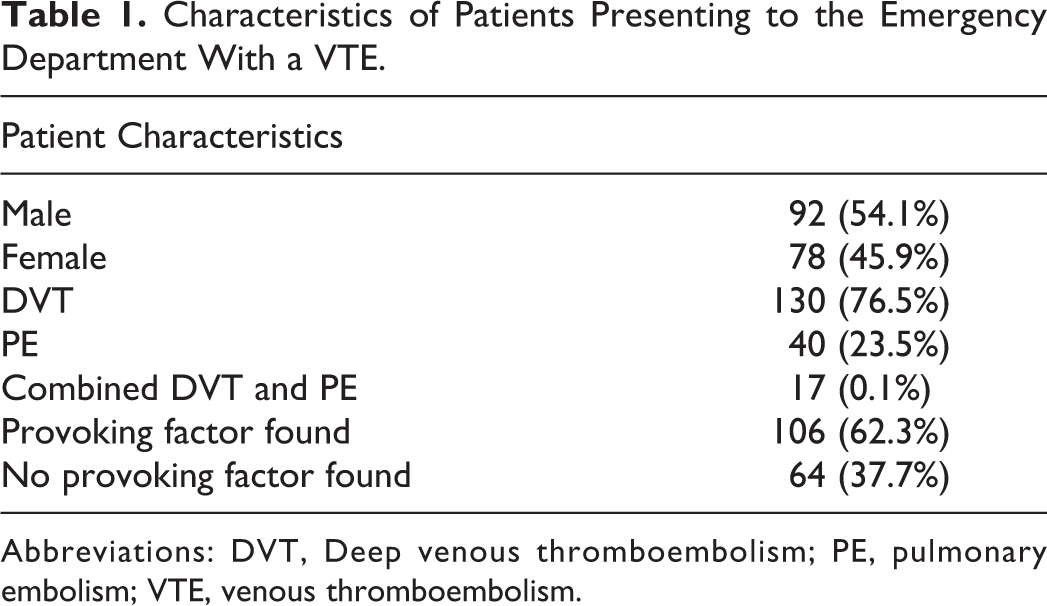
Abbreviations: DVT, Deep venous thromboembolism; PE, pulmonary embolism; VTE, venous thromboembolism.
Outcomes of CT of the Abdomen and Pelvis.
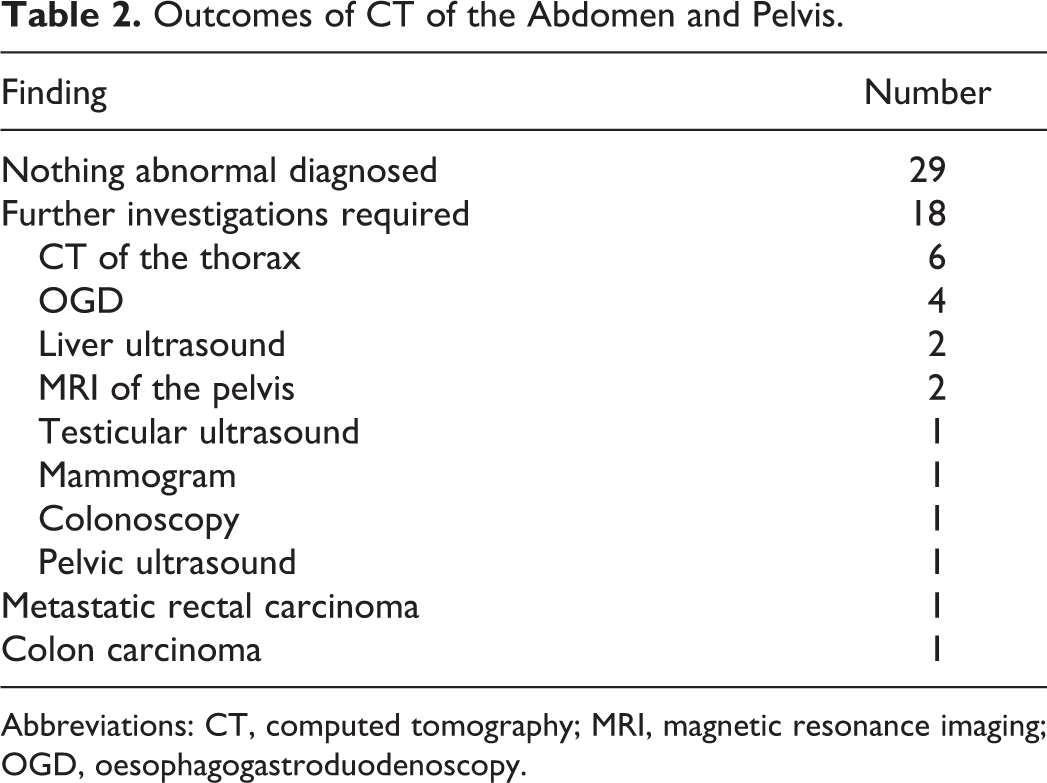
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; OGD, oesophagogastroduodenoscopy.
Of note, 17 of the patients with unprovoked VTE had not undergone CT scanning at the time of data collection. The reasons included limited availability of this investigation, with resultant long waiting lists, and failure of patients to attend scheduled investigations.
A total of 18 further investigations were required to further characterize findings detected on the initial screening CT scans. Pulmonary nodules were detected in 12.8% of patients, all of whom required a surveillance CT thorax. Enteric endoscopy was required in 5 patients for further investigation of CT findings suggestive of possible bowel wall thickening, liver ultrasounds were recommended for 2 patients to further investigate liver lesions, 2 magnetic resonance imaging of the pelvis for further investigation of adnexal thickening were required, a mammogram was recommended for a patient who fell outside the age range for guideline-mandated screening mammography, and a testicular ultrasound was recommended in 1 case. Twelve of these 18 additional investigations had been performed by the time of data collection, none of which had led to the detection of any lesion of clinical significance.
The initial CT scan identified a May-Thurner anatomical variant in 1 individual, and in 2 patients, a malignant tumor was detected. However, in the case of the first individual diagnosed with cancer (recurrent colorectal cancer), his history of carcinoma would have prompted a CT scan in the setting of unprovoked VTE regardless of the screening guideline recommendations. Similarly, the second patient diagnosed with colorectal carcinoma reported symptoms, which were suggestive of an underlying bowel neoplasm (including unexplained weight loss and abdominal pain) at the time of his presentation with unprovoked VTE, and as such, a CT scan of the abdomen would also have been carried out in this case regardless of the screening policy for asymptomatic individuals. In other words, even if there was not already a local policy, recommending extensive CT scanning for patients with unprovoked VTE in place in our institution at the time, a CT scan of the abdomen would still have been performed on both individuals subsequently diagnosed with cancer in our cohort based on their clinical presentation.
Discussion
The mechanisms by which cancer mediates enhanced activation of coagulation are varied and have yet to be fully elucidated. 2 Several investigators have demonstrated evidence of aberrant expression of tissue factor (TF) and procoagulant proteases on the surface of cancer cells as well as enhanced expression of circulating TF-bearing microparticles and have postulated that these observations may contribute in part to the thrombotic phenotype associated with active malignancy. 15,16 Similarly, the enhanced plasma levels of procoagulant factors such as coagulation factor VIII and fibrinogen as well as diminished sensitivity to the anticoagulant activity of activated protein C have also been reported in the setting of certain cancers and appear to contribute to the associated thrombotic risk. 17,18 In recent years, several additional novel mechanisms through which active cancer may induce a hypercoagulable state have been postulated, including a number of studies that have demonstrated enhanced release of neutrophil extracellular traps (web-like complexes of DNA, histones, and antimicrobial proteins, which have been shown to exhibit procoagulant properties) in association with malignancy. 19 Although all the potential molecular mechanisms underlying the enhanced coagulation activation in cancer have yet to be fully characterized, the implications of cancer-mediated hypercoagulability are very well established, with VTE representing a common source of morbidity in cancer and a leading cause of cancer-associated death. 7
The detection of occult malignancy following a diagnosis of an otherwise unprovoked VTE is a well-recognized manifestation of this interplay between cancer and coagulation. 9 Consequently, when patients present with idiopathic VTE, the possibility of an underlying occult malignancy must be considered, and a detailed history and clinical examination must be performed in order to guide further investigations directed at detecting a malignant tumor. However, the role of more extensive screening in the absence of specific symptoms or signs suggestive of an occult cancer is less clear. Although current clinical practice guidelines suggest considering CT scanning of the abdomen and pelvis in all patients over the age of 40 years, recent data reported in the SOME trial suggest that such an approach is not warranted. 12,14 Similarly, a recent, large multicentre randomized study investigating the role of an extensive screening strategy incorporating the use of a comprehensive positron emission tomography–CT scan in detecting occult malignancy following an episode of unprovoked VTE did not demonstrate an increased rate of cancer detection. 20
In the present study, we report further data in support of the findings of the SOME trial. Within our single-center cohort of consecutive patients presenting with idiopathic VTE, the screening pathway recommended by the 2012 NICE guideline did not lead to the increased identification of occult malignancy. Although 2 of the 47 patients who underwent screening were found to have a malignant tumor, the clinical history provided by both individuals would have prompted CT scanning regardless of the recommendations of the current hospital guideline, and so the detection of these lesions cannot be attributed to this screening pathway. Furthermore, of the 2 tumors detected on routine screening, 1 was widely metastatic, and the detection of occult malignancy at this advanced stage on CT screening would not be predicted to improve outcomes and so undermines the spirit of “screening,” which is intended to find disease at an early, treatable stage. In addition to the 47 CT scans performed for the purposes of cancer screening among this cohort, a further 13 diagnostic imaging studies and 5 endoscopic investigations were required for further characterization of findings detected on initial screening CT. To date, none of these additional diagnostic tests have led to the identification of any lesion, benign or malignant, that could have implications for the health of the individual being tested, and yet they clearly represent a significant burden on health-care resources. The fact that 6 of the additional screening scans had not yet been performed at the time of data analysis reflects the magnitude of this burden.
The low yield from extensive cancer screening in unselected patients presenting with unprovoked VTE has been the subject of a number of other recent studies. In an Italian single-center trial where 195 patients with unprovoked VTE were randomized to undergo either limited screening or extensive CT screening (incorporating scans of the thorax, abdomen, and pelvis), no differences in rates of cancer detection or in overall survival were detected. 21 Similarly, in a UK-based retrospective single-center study incorporating results from 62 CT scans carried out in the setting of unprovoked VTE, only 1 incidental cancer was detected (early urothelial carcinoma of the bladder), but 28 of these scans identified other incidental findings, which necessitated extensive follow-up investigations. 22,23 In another similar study consisting of results from 23 CT scans undertaken for the purposes of cancer screening, no cancers were detected but 5 individuals required further investigations based on the initial CT results. 23
Interestingly, a recent post hoc analysis of outcomes in specific subgroups of patients studied in the SOME trial suggests that age greater than 60 years, a previous diagnosis of provoked VTE, or a smoking history may be associated with an increased risk of occult malignancy in patients presenting with unprovoked VTE. 24 An individualized approach to screening where patients undergo specific screening investigations based on risk factors such as those identified in the SOME trial post hoc analysis as well as ensuring that appropriate age- and gender-specific screening has been carried out may prove to be a more effective approach. 25 Moreover, consideration should also be given to possibly pursuing screening investigations, which are more cost-effective than extensive radiological imaging studies in the first instance and which would not be associated with potential adverse effects such as ionizing radiation exposure (including simple screening tests for fecal occult blood in patients at risk of colorectal cancer). 25
The results of the present study (while limited by its small sample size and incomplete data relating to some of the screening investigations), in addition to these other previous reports of outcomes following extensive CT screening programs in the setting of unprovoked VTE, support the findings of the recent SOME trial and suggest that extensive imaging studies represent a significant burden to health-care resources and do not appear to improve clinical outcomes. In light of these findings, a more pragmatic approach to cancer screening is needed whereby clinicians remain cognizant of the clear association between unprovoked VTE and occult malignancy but also recognize that extensive screening of unselected patients is unlikely to be justified or cost-effective.
Footnotes
Authors’ Note
This article was presented at the Royal Academy of Medicine in Ireland Section of Interns Study Day on January 30, 2016, at the Royal College of Physicians of Ireland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.