We assessed the prevalence of elevated quantitative latex agglutination assay for D-dimer in patients in the emergency department in whom pulmonary embolism (PE) was excluded. D-dimer was normal (<230 ng/mL) in 435 (83%) of the 522 patients. D-dimer was normal in 88% of the patients with musculoskeletal or related chest pain, 74% with pleurisy or pleuritic chest pain, and 85% with upper respiratory tract infection. D-dimer was 230 to 500 ng/mL in 65 (75%) of the 87 in whom D-dimer was elevated. Clinical probability was low in 31 (48%) of the 65 patients with D-dimer levels of 230 to 500 ng/mL. D-dimer was 230 to 500 ng/mL and clinical probability was low in 31 (36%) of the 87 patients who had computed tomographic (CT) angiograms because of elevated D-dimer. Negative likelihood ratio for PE is sufficiently low that PE can be excluded with reasonable certainty in such patients. Tailoring cutoff value to 500 ng/mL in patients with low clinical probability would have reduced CT angiograms by 36%.
D-dimer, especially when combined with an objective clinical assessment, is useful for the exclusion of pulmonary embolism (PE), thereby eliminating the need for further testing.1 Many illnesses, trauma, and surgery may cause elevations in D-dimer, so an elevated D-dimer is not specific for PE.2–4 For this reason, D-dimer testing is most useful in the emergency department, because fewer emergency department patients than hospitalized patients have associated conditions that elevate D-dimer.2,5 Although illnesses or symptom complexes commonly seen in the emergency department that may include PE in the differential diagnosis may be accompanied by an elevated D-dimer, the usual extent of elevation has been sparsely described. Numerous computed tomographic (CT) pulmonary angiograms are obtained in the emergency department because of elevated levels of D-dimer in patients in whom PE is an unlikely diagnosis. Large numbers of patients, therefore, are exposed to ionizing radiation, which hopefully could be avoided. In the present investigation, we assess the levels of D-dimer in patients with illnesses or symptom complexes that included PE in the differential diagnosis, but in whom PE was excluded. Our intention is to obtain further data on false positive D-dimer elevations with commonly seen conditions in the emergency department, with the hope of applying this information to decrease the number of unnecessary CT pulmonary angiograms.
Methods
This is a retrospective cohort study of patients with suspected PE to determine the specificity of latex-derived, turbidometric immunoassay for D-dimer in the emergency department. Records were reviewed of all patients seen on the emergency service of a community hospital (St Mary Mercy Hospital, Livonia, Michigan) from January 1, 2011, to December 31, 2011, in whom a D-dimer was obtained and in whom a CT pulmonary angiogram was performed if the D-dimer was elevated. Interpretations of CT pulmonary angiograms were accepted without rereading for this investigation. Patients were excluded if the D-dimer was obtained because of suspected acute deep venous thrombosis (DVT). Patients were also excluded if the D-dimer was elevated, but no CT angiogram was obtained. We included only patients who had clinical features that raised a suspicion of PE. Patients were excluded if D-dimer was obtained as a routine for symptoms or illnesses that did not raise a suspicion of PE.
D-dimer was measured with a HemosIL latex-derived turbidometric immunoassay (Instrumentation Laboratory, Lexington, Massachusetts) using a Beckman/Instrumentation Lab-oratory Model: ACL 9000 (MYCO Instrumentation Source, Inc. Bonney Lake, WA). The cutoff value recommended by the manufacturer was 230 ng/mL. At this cutoff value, the manufacturer reported a sensitivity of 100% and specificity of 35.9% in a sample population of 78 patients confirmed as having venous thromboembolism (31 PE and 47 DVT) and 222 patients confirmed as negative (HemosIL D-dimer manual).
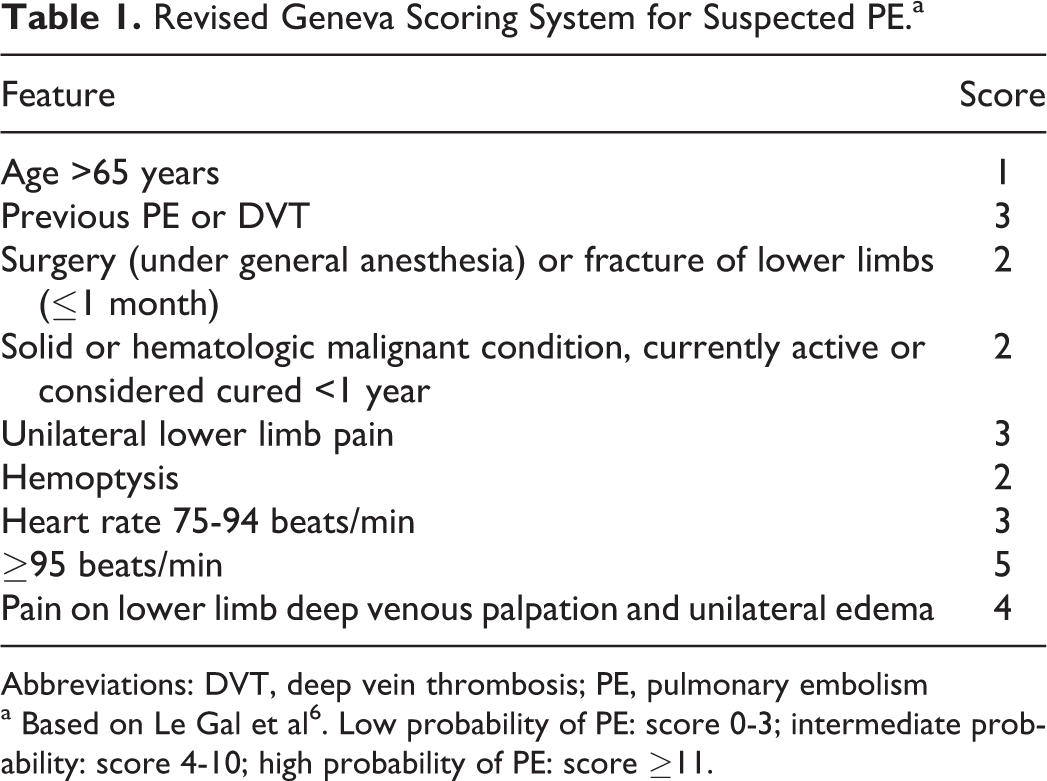
Clinical probability of PE was assessed from the medical records by the revised Geneva score6 (Table 1). We interpreted PE to be absent if the D-dimer level was <230 ng/mL, and clinical probability by the Geneva score was low or intermediate probability (score ≤10), or if the CT pulmonary angiogram was interpreted as not showing PE.
Revised Geneva Scoring System for Suspected PE.a
Feature
Score
Age >65 years
1
Previous PE or DVT
3
Surgery (under general anesthesia) or fracture of lower limbs (≤1 month)
2
Solid or hematologic malignant condition, currently active or considered cured <1 year
2
Unilateral lower limb pain
3
Hemoptysis
2
Heart rate 75-94 beats/min
3
≥95 beats/min
5
Pain on lower limb deep venous palpation and unilateral edema
4
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism
a Based on Le Gal et al6. Low probability of PE: score 0-3; intermediate probability: score 4-10; high probability of PE: score ≥11.
Statistical Analysis
A paired t test was used to assess the differences in D-dimer means within each age group using InStat version 3.0 GraphPad Software (San Diego, California). InStat version 3.0 GraphPad Software was also used to calculate the 95% confidence intervals (CIs). P < .05 was considered statistically significant. Specificity is defined as the ratio of number of patients with normal D-dimer to number of patients with PE absent.
Results
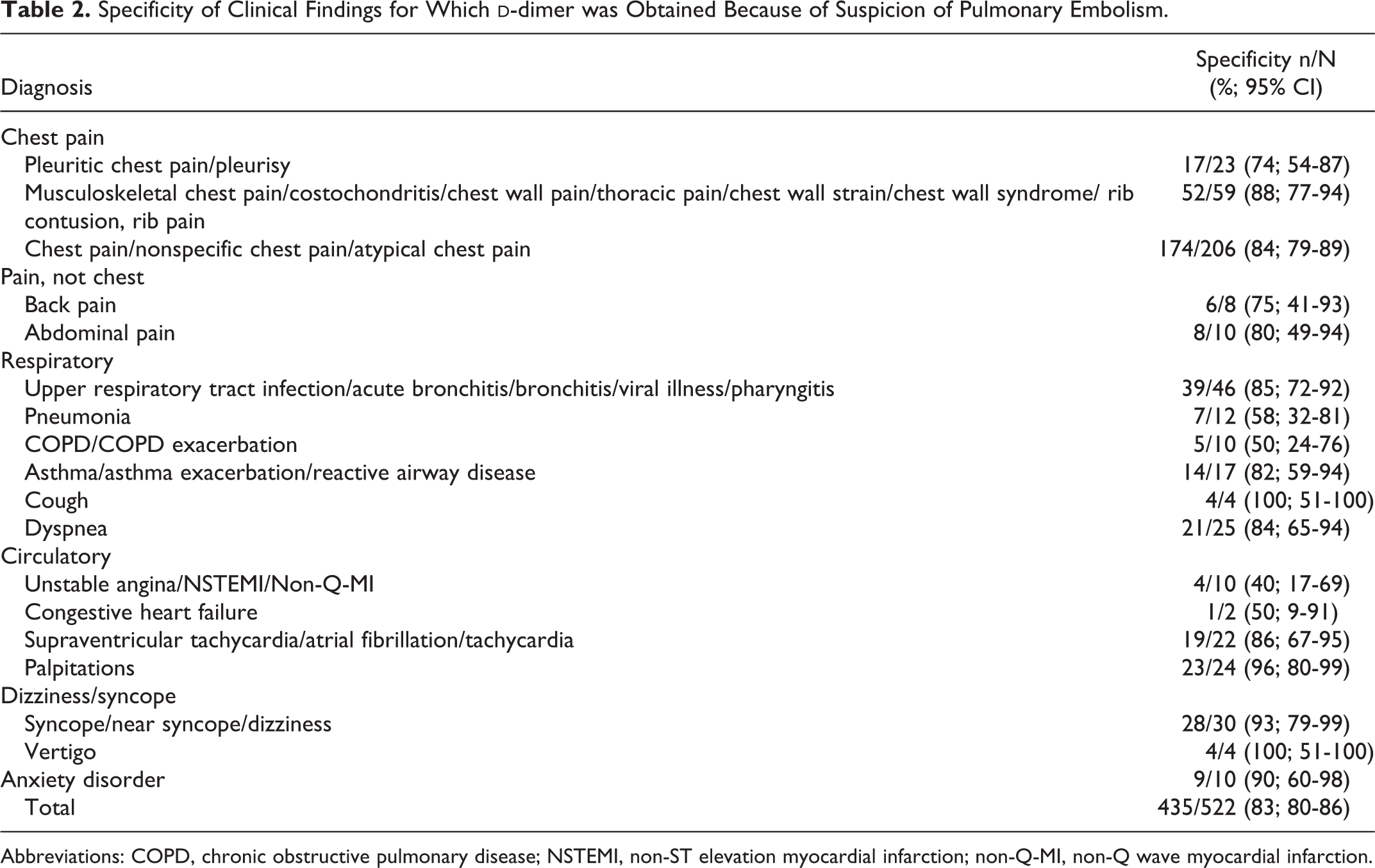
Measurements of D-dimer were obtained in 794 patients. Among these, 79 were excluded because D-dimer was obtained for suspected DVT rather than for PE, and 71 were excluded because D-dimer was elevated (≥230 ng/mL), but CT pulmonary angiography was not obtained. Among the remaining 644 eligible patients, 522 had clinical findings that raised a suspicion of PE (Table 2). All had either a normal D-dimer level (<230 ng/mL) in combination with a low or intermediate objective clinical probability based on a Geneva score ≤10 or a CT pulmonary angiogram that showed no PE.
Specificity of Clinical Findings for Which D-dimer was Obtained Because of Suspicion of Pulmonary Embolism.
Age of the included patients was 43 ± 18 years (mean ± standard deviation). In all, 93 (18%) of the 522 were aged 60 years or older. Age was skewed from a normal distribution toward a younger population. Among patients of all ages, 68% were female. Race was recorded in 459 patients, among whom 79% were white and 19% were black.
Among patients with conditions that raised a suspicion of PE, D-dimer was <230 ng/mL in 435 (83%) of 522. The most frequent clinical finding for which D-dimer was obtained because of a suspicion of PE was chest pain in 39% of the included patients (Table 2). Chest pain may have been listed as musculoskeletal chest pain, costochondritis, chest wall pain, thoracic pain, chest wall strain, chest wall syndrome, rib contusion, or rib pain. Among patients with chest pain, 88% had a D-dimer <230 ng/mL (Table 2). Among those with pleurisy or pleuritic chest pain, D-dimer was normal in 74%. With upper respiratory tract infection, D-dimer was normal in 85%, but with pneumonia it was normal in 58%. Those with chronic obstructive pulmonary disease (COPD) and those with acute coronary syndrome, although few in number, showed normal D-dimer in 50% and 40%, respectively (Table 2).
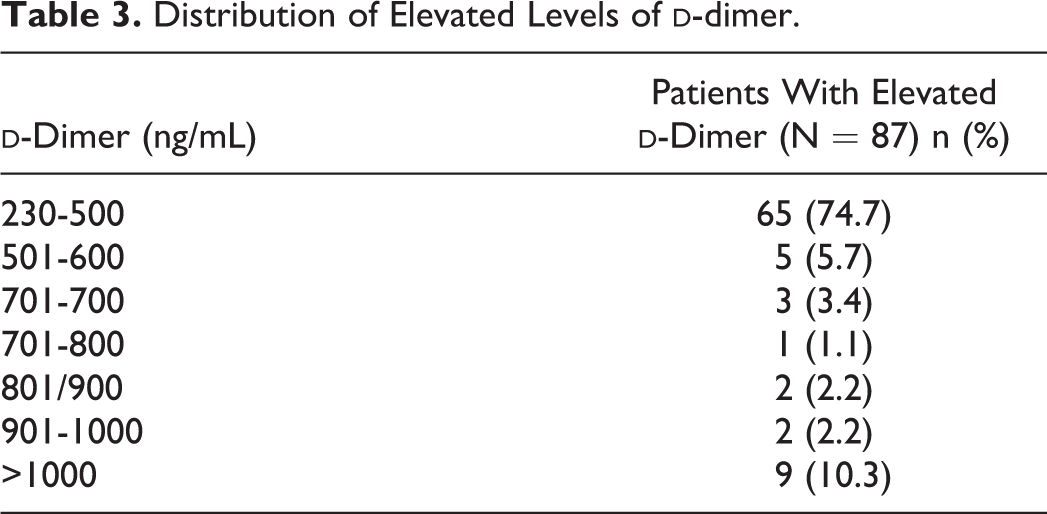
D-dimer was between 230 and 500 ng/mL in 65 (12%) of the 522 patients who had clinical findings that raised a suspicion of PE. Among patients in whom D-dimer was elevated beyond the recommended cutoff of 230 ng/mL, it was between 230 and 500 ng/mL in 65 (75%) of the 87 patients (Table 3). Clinical probability of PE was low (0-3 by Geneva scoring system) in 31 (48%) of the 65, with D-dimer elevation between 230 and 500 ng/mL. Consequently, 31 (36%) of the 87 patients who had CT pulmonary angiograms because of an elevated D-dimer had D-dimer of 230 to 500 ng/mL and low clinical probability. D-dimer was higher in patients aged 60 years or older than in younger patients (P < .0001; Figure 1).
D-dimer levels according to age in patients in whom pulmonary embolism was excluded. Values are shown as mean ± 95% confidence interval.
Distribution of Elevated Levels of D-dimer.
D-dimer (ng/mL)
Patients With Elevated D-dimer (N = 87) n (%)
230-500
65 (74.7)
501-600
5 (5.7)
701-700
3 (3.4)
701-800
1 (1.1)
801/900
2 (2.2)
901-1000
2 (2.2)
>1000
9 (10.3)
Discussion
D-dimer measured by a quantitative latex agglutination assay was normal (<230 ng/mL) in 83% of the patients in whom PE was considered in the emergency department of a community hospital. Most elevations of D-dimer were between 230 and 500 ng/mL. D-dimer was 230 to 500 ng/mL and clinical probability was low in 31 (36%) of the 87 patients who had CT pulmonary angiograms because of an elevated D-dimer. Tailoring the cutoff value to 500 ng/mL in those with a low probability clinical assessment would reduce the number of CT pulmonary angiograms required.
The specificity of 83% that we observed was higher than that usually reported. Systematic review showed a specificity for PE of 44% by quantitative latex agglutination assays at a similar cutoff value of 250 ng/mL.4The higher specificity that we observed may relate to the high proportion of patients in our population who had nonspecific chest pain, musculoskeletal chest pain, upper respiratory infection, and syncope or near syncope. We showed that such patients usually have normal D-dimer. Patients with conditions known to have elevated D-dimer tests, which would result in a low specificity for PE, include those with neoplasms,2 trauma,3 recent surgery,3 and pregnancy.7 Such patients were not in the population of emergency department patients that we evaluated.
Most patients with elevated D-dimer by quantitative latex agglutination assay showed levels between 230 and 500 ng/mL, which is in the range of normal for rapid enzyme-linked immunosorbent assay (ELISA).4 The proportion of patients with PE increases according to the level of D-dimer.8,9D-dimer concentrations are highest in patients with PE in the pulmonary trunk10 and with perfusion scan defects involving >50% of the lung.11 Only 2% of the patients with D-dimer <500 ng/mL measured by rapid ELISA or quantitative latex agglutination assay had PE.8
There is sparse published information on the specificity of D-dimer with conditions that raise a suspicion of PE. Kabrhel et al3 showed 39% of false positive D-dimer in asthma patients in the emergency department, but we showed fewer, that is, 18%. They showed false positive D-dimer in 61% with COPD, and we showed 50% false positive in a small number of patients.
In small number of patients we showed that 42% with pneumonia had an elevated D-dimer. Plasma D-dimer levels increase with severity of community-acquired pneumonia.12
Nonspecific chest pain was shown by others, as we showed, to be the most frequent discharge diagnosis in emergency department patients in whom PE was ruled out.13,14 Among 1070 patients in whom PE was ruled out, Bagattini et al13 showed 31% had a discharge diagnosis of nonspecific chest pain. In our study when we included pleuritic pain, 44% had nonspecific chest pain. They showed pleuritis in 7.5% as the discharge diagnosis, and we showed it in 4.2%. Bagattini et al13 showed pneumonia in 6.0% and we showed it in 2.0%. In general, the frequencies of various conditions in which PE was suspected were similar to the frequencies that we observed.13 We showed, as others, that the proportion of patients with abnormal D-dimer increases with age.3 Normal D-dimer levels are uncommon in patients older than 80 years of age.15,16
D-dimer assays differ in sensitivity and specificity among patients with suspected PE.4 In patients with suspected PE, the values of sensitivity for the ELISA and quantitative rapid ELISA were significantly superior to those for quantitative latex agglutination, semiquantitative latex agglutination, and whole blood agglutination assays.4 The conventional ELISA is considered a reference standard for determination of D-dimer concentration.4 The conventional ELISA is not practical for use in the diagnosis of PE, because it is laboratory intensive.4 Availability in most centers is limited. The quantitative rapid ELISA uses an antibody to D-dimer that is fluorescent labeled. An automated immunoanalyzer provides a numerical result. Results can be obtained in approximately 35 minutes. The semiquantitative rapid ELISA employs an antibody to D-dimer that is tagged to a color-producing agent. Plasma D-dimer concentration is quantified from the degree of color intensity produced. The qualitative rapid ELISA involves the detection of D-dimer by an anti-D-dimer monoclonal antibody coupled with alkaline phosphatase. Activity is revealed by the addition of a substrate that causes a color change. The intensity of the color is read visually by comparison with a positive and negative control. Results of the semiquantitative rapid ELISA and qualitative rapid ELISA are typically obtained within 10 minutes or less.4 Quantitative latex agglutination assays use monoclonal antibodies to D-dimer that are coated onto latex particles. In the presence of D-dimer, the particles aggregate to form larger aggregates and results in the decreased light scattering. Quantification of the D-dimer concentration is done with an analyzer that detects agglutination and precipitation turbidimetrically. Results are obtained in 7 to 15 minutes.4 Semiquantitative latex agglutination assays rely on the use of monoclonal antibodies to D-dimer that are coated onto latex particles. Macroscopic agglutinations are seen when elevated D-dimer levels are present in the plasma. Results are obtained in 3 to 4 minutes. The most frequently studied whole blood assay uses a freshly collected drop of capillary or venous whole blood mixed with a conjugate of monoclonal antibody to D-dimer. The latter is linked to a monoclonal antibody to human red blood cells. Visible agglutination of red cells takes place in the presence of elevated D-dimer levels. Interpreter experience is important due to the difficulty in discriminating between weak positive and normal results. Results are available in 2 minutes.4
The clinical utility of the D-dimer assays is limited by the nonspecificity of a positive result because of factors such as inflammation, trauma, and surgery. The clinical utility of D-dimer assays may be higher in outpatients as a result of a lower frequency of disorders, leading to an elevated measurement. Among patients hospitalized on a general internal medicine ward, D-dimer plasma concentration using ELISA exceeded the cutoff of 500 ng/mL in many illnesses, including pulmonary infection, neoplasia, coronary, and cerebrovascular disorder.2D-dimer levels also may be elevated in patients after trauma and surgery.3D-dimer levels may be elevated in patients with a history of DVT or PE.17 In pregnancy, D-dimer levels increase with the gestational period.7 However, during the early weeks of pregnancy (<20 weeks), D-dimer remains a useful test.7D-dimer levels are commonly elevated in patients older than 80 years of age.15,16 In these populations, measurement of D-dimer may not be useful.18
Negative likelihood ratios <0.1 generate large and conclusive changes, and negative likely ratios of 0.1 to 0.2 generate moderate shifts19 when the probability of PE is assessed with D-dimer in combination with pretest clinical probability. Likelihood ratios for a negative test are calculated as (1 − sensitivity)/specificity.19,20 The ELISA and quantitative rapid ELISA have negative likelihood ratios that would usually generate conclusive changes from pretest to posttest probability and provide high certainty for excluding PE.4 The negative likelihood ratio of the quantitative latex agglutination assay, 0.24, was not as low as the quantitative rapid ELISA assay, 0.13, when using a cutoff value of 500 ng/mL.4 Combining a negative rapid ELISA result with a low or moderate clinical probability for PE rules out PE.4 The non-ELISA assays at a cutoff value of 500 ng/mL, when combined with a low clinical probability for PE, but not moderate clinical probability, also provide a reasonable certainty of ruling out PE.4,21–23
At a cutoff of 250 ng/mL, the negative likelihood ratio of quantitative latex agglutination test is 0.14.4 This is similar to the negative likelihood ratio of quantitative rapid ELISA at a cutoff of 500 ng/mL, which is 0.13.4 This value of negative likelihood ratio would permit exclusion of PE with a negative D-dimer and intermediate as well as low clinical probability. Using the manufacturer's data with a cutoff of 230 ng/mL, the negative likelihood ratio would be even lower, thereby permitting exclusion of PE with a low or intermediate clinical probability of PE.
Strength of this investigation is that it shows levels of D-dimer for individual illnesses or clinical features that may raise a suspicion of PE. Although the specificity of D-dimer has been investigated extensively, there are sparse data on specificity for individual illnesses or symptom complexes in the differential diagnosis of PE. There is a particular need to evaluate specificity of D-dimer with latex agglutination assay using a cutoff of 230 ng/mL. This cutoff is well below the cutoff used for ELISA (500 ng/mL), which has been tested more extensively. A weakness is that we have small number of patients with several illnesses that raise a suspicion of PE. Another weakness is that the investigation was retrospective. This prevented us from obtaining information on severity of the disease and its relation to the specificity of D-dimer. We did not evaluate renal function. Patients with impaired renal function have higher levels of D-dimer than those with normal renal function and more often have an abnormal level of D-dimer.14
A high proportion of patients with a positive D-dimer test, but without PE, has resulted in a cost-efficacy imbalance in the diagnostic strategies based on D-dimer testing.24 It has been questioned whether implementing a costly diagnostic workup in a population with a low prevalence of PE is reasonable.24 There is a need to evaluate which patients with an elevated D-dimer test should undergo a diagnostic workup.24 There may be a place for tailoring cutoff values according to the clinical probability of PE and/or individual patient characteristics.25,26 In patients with suspected PE who have a D-dimer level <500 ng/mL by quantitative latex agglutination assay and a low clinical probability of PE, the negative likelihood ratio is sufficiently low to exclude PE with reasonable certainty4 and spare patients the radiation of CT pulmonary angiography.
In conclusion, D-dimer with quantitative latex agglutination assay at a cutoff of 230 ng/mL was normal in 83% of the patients in the emergency department with conditions that raised a suspicion of PE. When D-dimer was elevated, the values were usually between 230 and 500 ng/mL. Patients with a low clinical probability of PE and D-dimer by quantitative latex agglutination assay between 230 and 500 ng/mL do not need to undergo CT pulmonary angiography, because it was previously shown that the negative likelihood ratio is sufficiently low to exclude PE in such patients with reasonable certainty. Tailoring the cutoff value to 500 ng/mL in patients with a low probability clinical assessment would have reduced the number of CT pulmonary angiograms by over one-third.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
1.
SteinPDWoodardPKWegJG. Diagnostic pathways in acute pulmonary embolism: recommendations of the PIOPED II investigators. Am J Med. 2006;119(12):1048–1055.
2.
RaimondiPBongardOde MoerloosePReberGWaldvogelFBounameauxH. D-dimer plasma concentration in various clinical conditions: implication for the use of this test in the diagnostic approach of venous thromboembolism. Thromb Res. 1993;69(1):125–130.
3.
KabrhelCMark CourtneyDCamargoCAJr. Factors associated with positive D-dimer results in patients evaluated for pulmonary embolism. Acad Emerg Med. 2010;17(6):589–597.
4.
SteinPDHullRDPatelKC. D-dimer for the exclusion of deep venous thrombosis and acute pulmonary embolism: a systematic review. Ann Intern Med. 2004;140(8):589–602.
5.
SchrecengostJELeGalloRDBoydJC. Comparison of diagnostic accuracies in outpatients and hospitalized patients of d-dimer testing for the evaluation of suspected pulmonary embolism. Clin Chem. 2003;49(9):1483–1490.
6.
Le GalGRighiniMRoyP-M. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006;144(3):165–171.
7.
ChablozPReberGBoehlenF. TAFI antigen and D-dimer levels during normal pregnancy and at delivery. Br J Haematol. 2001;115(1):150–152.
8.
TickLWNijkeuterMKramerMH; Christopher Study Investigators. High D-dimer levels increase the likelihood of pulmonary embolism. J Intern Med. 2008;264(2):195–200.
9.
ChopraNDoddamreddyPGrewalHKumarPC. An elevated D-dimer value: a burden on our patients and hospitals. Int J Gen Med. 2012;5:87–92.
10.
de MonyeWSansonBJBullerHR. The performance of two rapid quantitative D-dimer assays in 287 patients with clinically suspected pulmonary embolism. Thromb Res. 2002;107(6):283–286.
11.
GalleCPapazyanJPMironMJSlosmanDBounameauxHPerrierA. Prediction of pulmonary embolism extent by clinical findings, D-dimer level and deep vein thrombosis shown by ultrasound. Thromb Haemost. 2001;86(5):1156–1160.
12.
GüneyselOPirmitSKarakurtS. Plasma d-dimer levels increase with the severity of community acquired pneumonia. Tuberk Toraks. 2004;52(4):341–347.
13.
BagattiniSBBounameauxHPernegerTPerrierA. Suspicion of pulmonary embolism in outpatients: nonspecific chest pain is the most frequent alternative diagnosis. J Intern Med. 2004;256(2):153–160.
14.
Karami-DjurabiRKlokFAKooimanJVelthuisSINijkeuterMHuismanMV. D-dimer testing in patients with suspected pulmonary embolism and impaired renal function. Am J Med. 2009;122(11):1050–1053.
15.
RighiniMGoehringCBounameauxHPerrierA. Effects of age on the performance of common diagnostic tests for pulmonary embolism. Am J Med. 2000;109(5):357–361.
16.
BarroCBossonJLPernodG. Plasma D-dimer testing improves teh management of thromboembolic disease in hospitalized patients. Thromb Res. 1999;95(5):263–269.
17.
Le GalGRighiniMRoyPM. Value of D-dimer testing for the exclusion of pulmonary embolism in patients with previous venous thromboembolism. Arch Intern Med. 2006;166(2):176–180.
18.
SteinPDSostmanHDBounameauxH. Challenges in the diagnosis of acute pulmonary embolism. Am J Med. 2008;121(7):565–571.
19.
JaeschkeRGuyattGHSackettDL. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group. JAMA. 1994;271(9):703–707.
20.
SoxHC. Commentary. Ann Intern Med. 2004;140:602.
21.
TickLWTonEvan VoorthuizenT. Practical diagnostic management of patients with clinically suspected deep vein thrombosis by clinical probability test, compression ultrasonography, and D-dimer test. Am J Med. 2002;113(8):630–635.
22.
KearonCGinsbergJSDouketisJ. Management of suspected deep venous thrombosis in outpatients by using clinical assessment and D-dimer testing. Ann Intern Med. 2001;135(2):108–111
23.
WellsPSAndersonDRRodgerM. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003;349(13):1227–1235.
24.
Le GalGBounameauxH. Diagnosing pulmonary embolism: running after the decreasing prevalence of cases among suspected patients. J Thromb Haemost. 2004;2(8):1244–1246.
25.
RavivBIsraelitSH. Shifting up cutoff value of d-dimer in the evaluation of pulmonary embolism: a viable option? Possible risks and benefits. Emerg Med Int. 2012;2012:517375.
26.
LinkinsLABatesSMGinsbergJSKearonC. Use of different D-dimer levels to exclude venous thromboembolism depending on clinical probability. J Thromb Haemost. 2004;2(8):1256–1260.