
Abstract
A 69-year-old woman presented to the emergency department with sudden onset of dyspnea. She reported bilateral total knee surgery 12 days prior for gonarthrosis. The patient was recommended low-molecular-weight heparin (LMWH) 0.4 cc (4 milliliter) twice a day. On evaluation, severe thrombocytopenia was detected. An echocardiogram was performed because of her dyspnea, which revealed right ventricular dilatation and hypokinesis. Due to suspicion of a pulmonary embolism (PE), a pulmonary computed tomography (CT) was performed, which revealed bilateral massive PE. This event occurred while the patient was receiving LMWH for prophylaxis of PE. Due to the presence of severe thrombocytopenia, fondaparinux and immunoglobulin were initiated. Her platelet levels improved significantly and she was discharged on warfarin.
Introduction
Heparin-induced thrombocytopenia (HIT) is an immune-mediated, potentially fatal disorder caused by the development of antibodies to platelet factor 4 (PF-4) and heparin. 1 Although it is about 10 times more common with unfractioned heparin than with low-molecular-weight heparin (LMWH), in this case a pulmonary embolism (PE) occured when the patient was prophylactically receiving LMWH after orthopedic surgery. Herein, we report HIT complicated by PE and treated the patient successfully with fondaparinux and immunoglobulin.
Case Report
A 69-year-old woman presented to the emergency department with sudden onset of dyspnea. She reported bilateral total knee surgery 12 days prior for gonarthrosis. After the operation, she was prescribed enoxaparine 0.4 cc twice daily. She had no previous history of diabetes mellitus, hypertension, usage of any medication, or smoking. On physical examination, she appeared to be in severe respiratory distress. Her functional capacity was New York Heart Association class III. She was cyanotic, with a regular heart rate of 114 beats/min, and a blood pressure of 80/60 mm Hg. Her respiratory rate was 35 breaths/min, with an oxygen saturation of 84% while she was breathing room air. Investigation was performed for lower limb deep venous thrombosis and revealed normal findings. All the other system examinations were normal.
Her hemoglobin level was 9.6 g/dL, hematocrite was 41.2%, white blood cell count (WBC) was 7780/mm3, and her platelet count was 14 000/µL. Biochemical investigation was within normal limits. Her arterial blood gas analysis taken without oxygen revealed a pH of 7.54, partial pressure of carbon dioxide (P
A spiral computed tomography (CT) was performed, which revealed a massive bilateral PE (Figure 1 ). Due to her hemodynamic instability, she was given thrombolytic therapy. However, due to severe thrombocytopenia and the unavailability of surgical embolectomy in our hospital, immunoglobulin G (IgG) at a dose of 1 g/kg per body weight for 3 consecutive days and fondaparinux (Arixtra, GlaxoSmithKline, United Kingdom) 2.5 mg/d were initiated because of our suspicion of HIT. Antibodies against heparin-PF-4 complexes, measured by enzyme immunoassay (enzyme-linked immunosorbent assay [ELISA]), were detected.
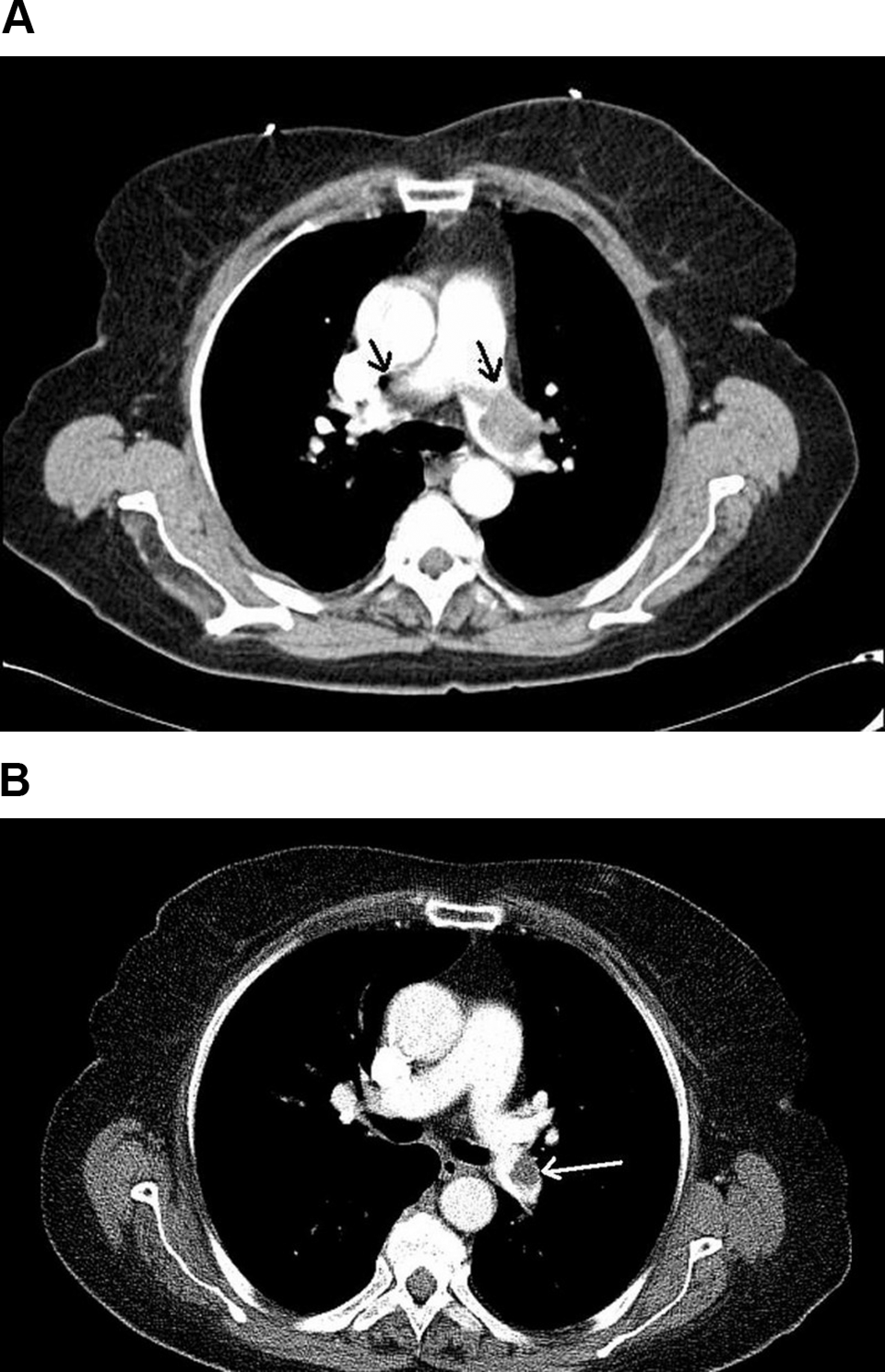
A. Transverse CT image shows bilateral thrombus images (arrows) in the pulmonary arteries. B. Control CT image shows a perfussion defect only in the left pulmonary artery (arrow). CT indicates computed tomography.
In a few days, she showed significant improvement with normalization of her platelet count (124 000/µL; Figure 2 ). A control pulmonary CT was performed after 2 weeks and showed marked improvement in the thrombus, and the perfussion defect was detected only in the left pulmonary artery (Figure 1B). The patient was discharged under treatment with warfarin.
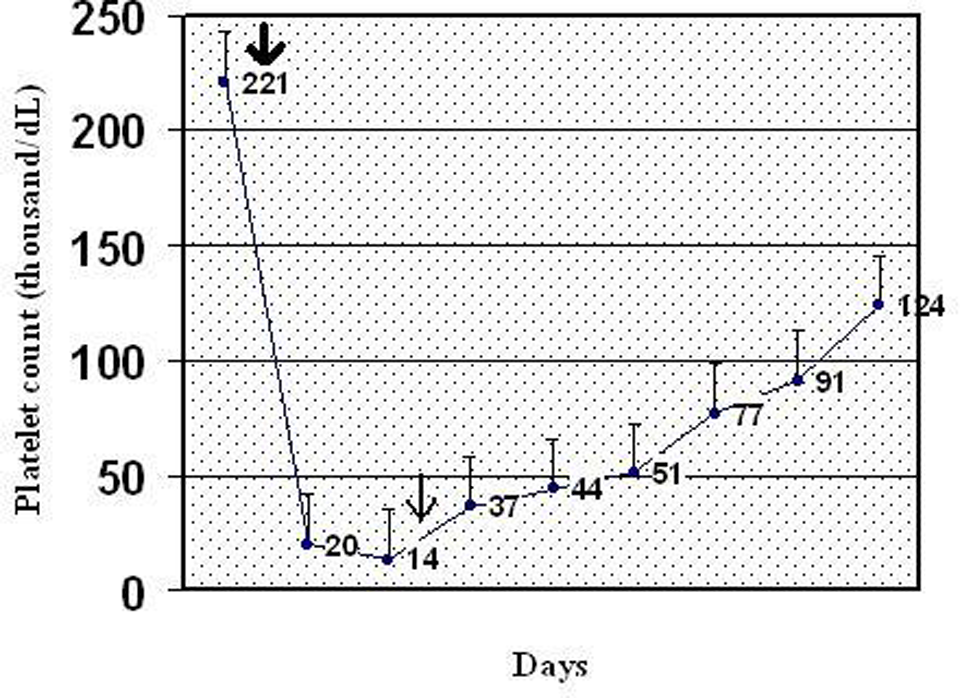
Medication history. Thick arrow indicates platelet count before surgical intervention (total knee surgery) and fondaparinux + IgG was initiated (thin arrow). IgG indicates immunoglobulin G.
Discussion
The development of thrombocytopenia in a patient receiving heparin or LMWH requires careful and prompt assesment of HIT. Two types of HIT were classified: HIT I and HIT II. HIT I is a benign, transient, and nonimmune type, and its symptoms are very slight. However, HIT II is immune-mediated thrombocytopenia, which is caused by the development of antibodies to PF-4 and characterized by the presence of venous and arterial thrombosis. Thrombosis is a life-threatening condition with a high mortality rate of 30% to 40%. 2
This case higlights the importance of thromboembolic events under heparin treatment defined as heparin-induced thrombocytopenic thrombocitosis. Early recognition and management of these life-threatening circumstances are crucial responses when symptoms are present. Treatment of thromboembolic events including PE as a cause of HIT includes discontinuation of all heparins and initiation of an alternative anticoagulant. 3 The suggested prophylactic dose of LMWH for orthopedic surgery is 0.4mg/d, but in this case 0.4 mg twice a day was given because of our hospital policy. Alternate agents that have been used effectively in HIT include lepirudin, danaproid, argatroban, bivaluridin (Food and Drug Administration approved for patients with HIT only during percutaneous coronary interventions), and fondaparinux. 4 Althogh fondaparinux-induced thrombocitopenia has been reported in 2 patients, 5,6 it has not been approved for treatment of HIT in the United States, 3 and we used this agent in our patient because of its availability in Turkey. The patient’s thrombocypenia improved significantly with this therapy. We assume that more data supporting the efficacy of fondaparinux in the treatment of HIT is needed.
The distinctive and outstanding feature of this case was the patient’s unstable hemodynamic status on admission. Currently, the treatment guidelines strongly recommend the use of thrombolytic treatment in patients with acute massive PE associated with cardiogenic shock, or overt hemodynamic instability. 7 However, we could not initiate thrombolytic therapy because of thrombocytopenia. It is well documented in the literature that patients who do not respond or are not eligible for thrombolytic therapy should be referred to rescue surgical embolectomy, 8 but due to the unavailability of surgical embolectomy intervention in our hospital, we made a decision to follow the patient closely in the coronary care unit.
A probable presentation of HIT complicated by PE as demonstrated in the literature is rare. 9 –16
High doses of intravenous IgG therapy for the treatment of HIT were reported previously. 17 Betrosian et al demonstrated HIT complicated by PE treated successfully with recombinant hirudin and Ig therapy. 11 However, IgG combined with fondaparinux has not been reported previously.
In conclusion, we present a case of HIT complicated by acute massive PE, which was treated successfully with fondaparinux and Ig. Although this condition is very common, unfortunately most are misdiagnosed in clinical practice. Physicians need to diagnose and treat this life-threatening condition promptly.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.