
Abstract
Deep venous thrombosis (DVT) in children is more often associated with underlying pathological conditions than with hereditary thrombophilia. The present study is a retrospective analysis of thrombophilia in 285 pediatric patients with venous thrombosis at different sites. Four common thrombophilia markers, that is protein C, protein S, antithrombin III, and factor V Leiden (FVL) mutation, were analyzed. Thrombosis in hepatic and portal veins was more common in pediatric patients (73%) when compared to other sites (27%). Overall, hereditary thrombophilia accounted for 15.5% of the patients with venous thrombosis. The FVL mutation, which was the major causative factor in Budd–Chiari syndrome and portal vein thrombosis cases in the adult group, was not a major contributing factor in pediatric group, that is, 1.8% of the patients. In conclusion, the risk factors for venous thrombosis vary in different age groups.
Introduction
Symptomatic venous thrombosis is infrequent in children and are usually secondary to underlying neoplasms, congenital heart diseases, systemic lupus erythematosus, renal failure, infective diseases or are triggered by central venous lines, major trauma, or surgery. 1 –5 The annual incidence of venous thromboembolism (VTE) is 0.07 to 0.14 per 10 000 children in the general population, 2 while the prevalence of thrombophilia markers in children has been found to vary from 3% to 78%, 6 the wide range is largely due to variation in sample size and ethnicity of the population studied.
Unlike in adults, the role played by congenital prothrombotic abnormalities in development of VTE complications in pediatric patients still has to be clarified. There have been no studies on the prevalence of thrombophilia in pediatric population in our country with respect to both genetic and acquired causes. Various factors like socioeconomic conditions, hygiene, and lifestyle in the Asian subcontinent influence the acquired causes of thrombosis. Furthermore, there is no clarity on utility of thrombophilia marker tests in both adult and pediatric deep venous thrombosis (DVT) population in our country. Our objective was to find the causes of thrombosis in our pediatric DVT population including the utility of thrombophilia testing.
Materials and Methods
Study Population
A total of 285 patients (males 165; females 120, mean age 7.3 ± 6 years) were retrospectively analyzed in the present study. The patients were referred from various outdoor patient clinics of city hospitals as well as hospitals around the country during 2005 to 2010. Only those patients who had objectively confirmed thrombosis were included in the study. The imaging investigations included ultrasonography, computed tomography/magnetic resonance imaging, and Doppler studies. The consent of the ethics committee was obtained from the institutional board and informed consent was obtained from the patients. Detailed clinical history was obtained from the case sheets that were reviewed by one of the authors (K.G.).
Estimation of Thrombophilia Markers
Venous blood sample of 5 cm3 was drawn in 3.2% sodium citrate vacutainers and centrifuged at 4000 rpm for 15 minutes at 4°C. The plasma samples were stored at −70°C till further analysis. The pellet was stored at −20°C for molecular analysis. The samples were collected 3 months after the acute phase period of thrombotic event. All the blood samples were collected at least 14 days after stoppage of warfarin or prior to starting anticoagulation. The markers studied were protein C (PC), protein S (PS), and antithrombin (AT) III using enzyme-linked immunosorbent assay and chromogenic assays (Diagnostica Stago, Asnieres, France) and factor V Leiden (FVL) using molecular techniques. The normal ranges for PC, PS, and AT assays were 70% to 140%. All samples showing borderline PC, PS, and AT values (66%-74%) were repeated and only those samples that were consistent were considered as deficient.
Results
Table 1 shows the sites of thrombosis in our pediatric patients with DVT. The thrombosis in hepatoportal system accounted for significant number in our pediatric DVT group (73%) followed by cerebral venous thrombosis (14%). There was no significant difference in the 2 sexes with regard to the specificity of the sites. In all, 30 of 165 males and 17 of 120 females had some precipitating cause for thrombosis, details of which are presented in Table 2.
Sites of Thrombosis in Pediatric Patients Analyzed in the Present Study.
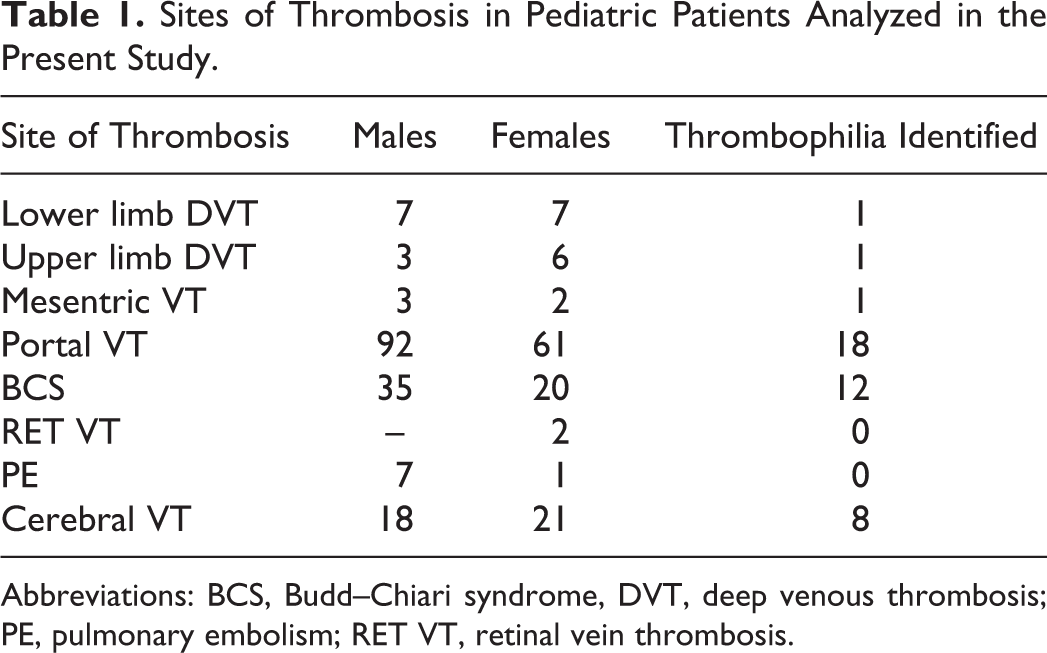
Abbreviations: BCS, Budd–Chiari syndrome, DVT, deep venous thrombosis; PE, pulmonary embolism; RET VT, retinal vein thrombosis.
Acquired Causes of Thrombosis.
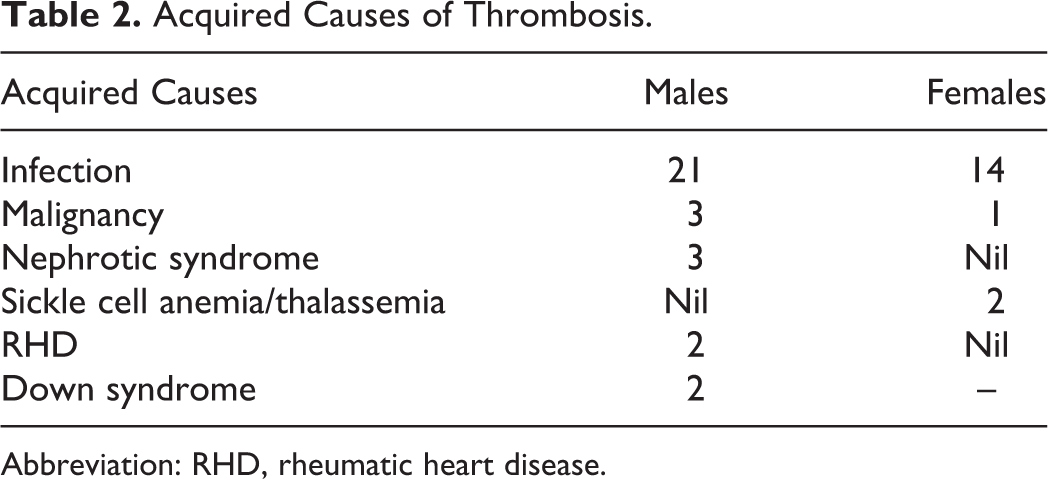
Abbreviation: RHD, rheumatic heart disease.
Distribution of different acquired factors in male and female patients is presented in Table 2. The overall prevalence of inherited thrombophilia markers was found to be 15.47%; PC deficiency was the commonest while AT deficiency was rare in the present series (Table 3). Infections accounted for 13% in our patient group, primarily tuberculosis and malaria. Overall, acquired factors of thrombosis accounted for 18.11% of the patient population.
Inherited Causes of Thrombosis.
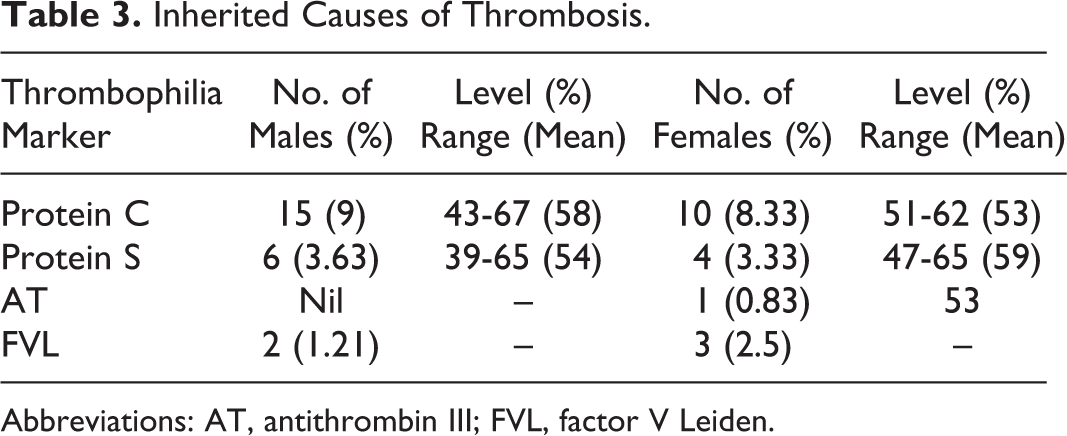
Abbreviations: AT, antithrombin III; FVL, factor V Leiden.
Analysis of thrombophilia markers with respect to sites of thrombosis showed a varied prevalence for different sites, that is 2 (8.7%) of 23 for limb DVT, 18 (11.8%) of 153 for portal vein thrombosis (PVT), 12 (21.8%) of 55 for Budd–Chiari syndrome (BCS), and 8 of (20.5%) 39 for cerebral venous thrombosis.
Discussion
Deep venous thrombosis is an infrequent event in children but results in significant morbidity and mortality. The etiological causes are multifactorial, thus posing a challenge to the physicians because there is no definitive data available. The precipitating factors for DVT in Asian countries vary significantly from Western countries due to lifestyle and socioeconomic conditions. The clinical utility of thrombophilia testing has become increasingly debated, both in adults and in children. 7 ,8
One of the most striking features of the present series is a large number of BCS and PVT, while in the Western literature, BCS is not predominant in the pediatric DVT group and whenever present is associated with umbilical catheterization, sepsis, or severe enterocolitis. 9 –12 There are no reports from India on thrombophilia profile in pediatric BCS cases, but the only study involving 517 children below 14 years with portal hypertension had only 1% of BCS cases. 13 The high number of BCS cases in the present series may be due to referral bias.
Certain anticoagulant molecules like PC reach their normal levels around 10 years which could precipitate thrombosis in these patients. Incidentally, the prevalence of PC deficiency was found to be highest among the genetic markers studied and also in the hepatoportal group. Our findings concur with a similar study by Pinto et al. 14 Protein S deficiency was lower when compared to the adult DVT cases, while FVL mutation was contrastingly of very low prevalence in the hepatic and portal venous thrombosis group. 15 ,16 The insignificant role of FVL mutation was surprising because it accounted for 26.4% of our adult BCS population. 16 Overall, genetic causes accounted for just 15.47% in our pediatric group.
When analyzed separately, both PVT and BCS cases showed a higher prevalence of thrombophilia markers, that is, 12% and 23%, respectively. The low prevalence of FVL mutation in pediatric DVT cases is surprising, that is, 1.8% when compared to our adult series up to 26% in BCS and 6% in PVT cases. Similar studies with higher prevalence of thrombophilia in BCS and PVT have also been reported from other parts of the country. For instance, a study from Mumbai has shown that 4 (25%) of 16 children with a median age of 22 months and diagnosed as BCS were positive for any of the heritable or acquired thrombophilia markers studied. 17 Similarly, a study from Egypt showed 62.5% of the patients with PVT were positive for thrombophilia of which FVL was the commonest, that is 30%. 18 A study of 31 patients with extra hepatic portal venous thrombosis from Italy showed an overall frequency of thrombophilic abnormalities in 32% of the patients. 19 Of the 39 patients with cerebral venous thrombosis, 8 (27%) were positive for thrombophilia which is well within the reported range, that is, 20% to 50% by Mackay and Monagle. 20
Infections accounted for a large number in our patient population. Tuberculosis and malaria are very endemic in a tropical country like India. This leads to various complications in the coagulation cascade which predisposes the affected individuals to thrombosis. 21 ,22 Important risk factors in Western countries are the presence of central venous catheters, malignancy, and chemotherapy. Central venous catheters have also been reported to be an important cause of thrombosis in the pediatric group. 23 None of our patients had any indwelling catheter; malignancy and chemotherapy accounted only for a small fraction (1.4%) of patients. In a similar retrospective study from South India in 36 patients with BCS and other groups of splanchnic venous thrombosis which included both pediatric and adult patients, none of them were associated with catheterization. 24 In large majority of patients, there was no other associated clinical condition precipitating thrombosis in the present series.
A review by Raffini and Thornburg 7 describes a wide range in the prevalence of thrombophilia in pediatric DVT group, that is, as low as 13% 1 in Canada to as high as 78% 6 in Germany. In the present series, the prevalence of thrombophilia is 15.5% which is closer to Canadian data. We did not study factor VIII levels which were reported to be elevated in idiopathic PVT cases in our country. 25 JAK2 mutation was reported to be 13% in both patients with BCS and patients with PVT recently by our group. 26
In conclusion, the present study shows that thrombophilia is significantly associated with thrombosis in pediatric patients. Besides inherited causes, secondary factors, mainly infection, also play a significant role in precipitating the DVT in the pediatric patients. The commonest thrombophilia marker in adult DVT, that is FVL mutation, was not a major cause of thrombosis in pediatric DVT group. Another important feature is the absence of pulmonary embolism and catheter-associated thrombosis in this series. The major deficit of the present study is, however, lack of data on acquired thrombophilia including antiphospholipid antibodies in these patients. Neonates form an important subgroup with high incidence of thrombosis which however could not be included due to the referral bias in the present series.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.