
Abstract
Aim:
The purpose of the research was to study the influence of several genetic factors, especially the -1693 G>A polymorphism of the VKORC1 gene, on the risk of acute unprovoked lower extremity deep vein thrombosis (DVT).
Materials and Methods:
The study included 127 patients (median age 63 [53.2; 72] years; 61 [48%] women and 66 [52%] men) who were diagnosed with acute lower extremity DVT and 114 controls (median age 62 [53; 73] years; 64 [56.1%] women and 50 [43.9%] men) without DVT. We recorded data regarding the history of DVT and the presence of varicose veins. We determined the genotypes for factor V Leiden (FVL) mutation, prothrombin G20210A mutation, VKORC1 -1639 G>A mutation, and PAI-1 -675 4G/5G polymorphism.
Results and conclusion:
Varicose veins were found in 67 (52.8%) patients and 29 (25.4%) controls (P < .001). FVL was present in 29 (22.8%) patients and 10 (8.8%) controls (P = .005). The VKORC1 (-1693 G>A) GG genotype was found in 42 (33.1%) patients and 41 (36%) controls, the GA genotype in 71 (55.9%) patients and 47 (41.2%) controls, and AA genotype in 14 (11%) patients and 26 (22.8%) controls (P = .020). Multivariate analysis showed that the presence of varicose veins, FVL, and VKORC1 -1639 G>A was independently associated with the risk of DVT. The VKORC1 (-1693 G>A) AA genotype was associated with fewer cases of DVT (odds ratio = 0.435; 95% confidence interval 0.205-0.991; P = .031).
Introduction
Lower extremity deep vein thrombosis (DVT) is one of the most common diseases in the world. About 1 in 1000 adult individuals develops this disease annually. 1,2 The most frequent complications of DVT are pulmonary embolism and postthrombotic syndrome, which have increased morbidity and mortality rates.
There are many factors that contribute to the occurrence of DVT. Idiopathic DVT is diagnosed when there are no known risk factors, such as surgery, trauma, immobility, and pregnancy. 3 Risk factors that work together to the occurrence of DVT are either permanent or transient. Permanent risk factors associated with DVT are generally represented by hereditary thrombophilia: factor V Leiden (FVL) mutation, prothrombin G20210A mutation, antithrombin III deficiency, protein C, or protein S deficiency. 4 Other genetic factors, such as the C667T and A1298C polymorphisms of methylenetetrahydrofolate reductase gene and the plasminogen activator inhibitor (PAI-1) 4G/5G promoter polymorphism, are controversial, with studies and meta-analyses supporting their role as risk factors for venous or arterial thrombosis but also research showing their lack of influence on the occurrence of DVT. 5 –8 There are less common mutations that reduce the risk of DVT: factor XIII Val34Leu polymorphisms or polymorphisms in the gene of vitamin K epoxide reductase complex subunit 1 (VKORC1). 9,10
VKORC is an enzyme involved in the vitamin K cycle, reducing vitamin K to support the carboxylation and, after that, the activation of several vitamin K-dependent proteins, including coagulation factors (factors II, VII, IX, and X and proteins C and S). 11 The VKORC1 gene is polymorphic. Most of the VKORC1 gene single-nucleotide polymorphisms (SNPs) belong to 3 haplotypes: *2, *3, and *4. The VKORC1*2 haplotype is associated with lower dose of oral anticoagulant requirements. There are 5 relevant SNPs tagging the VKORC1*2 haplotype: -1639G>A, 1173C>T, 1542G>C, 2255T>C, and 3730G>A. As these SNPs are in strong linkage disequilibrium, genotyping for any of them is informative for the VKORC1*2 haplotype. 12,13 Wang et al showed that the VKORC1 -1639G>A SNP is functional, as it is responsible for a lower level of VKORC1 mRNA in human liver. 13 The role of VKORC gene polymorphisms has been studied extensively in relation to the impact on oral anticoagulant treatment with antivitamin K, as the target of these drugs is the C1 subunit of VKOR. Thus, the influence of the variant genotype of the VKORC1 -1693 G>A polymorphism was demonstrated on the therapeutic dose of acenocoumarol or warfarin. 14–16 Moreover, the involvement in the development of arterial and venous embolic events has also been studied. Studies have shown that patients with VKORC polymorphism mutant genotypes are at high risk of stroke and coronary heart disease. 17 Lacut et al showed the reduced presence of the TT genotype of the C117T polymorphism in the VKORC1 gene in patients with idiopathic DVT compared to controls. 10 There are studies that have not demonstrated the existence of a reduction in the risk of DVT in patients with VKORC variant genotype. 18
The purpose of the present study was to assess the influence of certain genetic factors, especially the -1693 G>A polymorphism of the VKORC1 gene, on the risk of acute unprovoked lower extremity DVT.
Material and Method
This was an observational, retrospective, analytical, case–control study. The study included 127 patients (61 [48%] women and 66 [52%] men) who were diagnosed with acute lower extremity DVT. The median age was 63 (53.2; 72) years. Acute DVT was diagnosed using duplex ultrasonography by means of an Aloka SSD-4000 (Hitachi-Aloka Medical, Ltd) device with a high-frequency linear transducer (7-10 MHz), according to the criteria in force. Participants with signs and symptoms suggestive of acute DVT and with a Wells score indicating a high probability of DVT underwent ultrasound examination. 19 The control group consisted of 114 participants (64 [56.1%] women and 50 [43.9%] men). The median age was 62 (53; 73) years. These participants were recruited on the first day of hospitalization, after the diagnosis of acute lower extremity DVT was excluded by duplex ultrasonography. Both the DVT group and the control group were composed of patients hospitalized in the internal medicine, cardiology, and geriatric wards of the Municipal Clinical Hospital of Cluj-Napoca between September 2009 and June 2011. All patients were included in the study after they had signed a consent form for enrollment in the study and genetic determinations. The study protocol was approved by the Ethics Committee of “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca.
Patients receiving oral or intravenous anticoagulant therapy at the time of enrollment were not included in the study. Participants with the following risk factors for acute DVT were also not included in the study: neoplasms, major surgery in the past 3 months, autoimmune diseases, any type of bed rest longer than 3 days, fractures of the lower limbs or of the pelvis in the past month, cast immobilization in the past 3 months, lower limb trauma, pregnancy, the use of oral contraceptives, and plane or car trips longer than 4 hours in the past month.
Demographic, clinical, and laboratory data were recorded for each patient. Data on the presence of comorbidities or different circumstances that could increase the risk of acute DVT (apart from the exclusion criteria) were also recorded: history of DVT or pulmonary embolism and varicose veins of the lower limbs. Body mass index was calculated for each patient.
Three-mL venous blood samples were collected from each patient in a vacutainer containing EDTA. The DNA was extracted from the blood sample at the Department of Genetics of “Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj-Napoca, using a DNA extraction kit (Wizard Genomic DNA Purification Kit; Promega, Madison, Wisconsin).
Genotyping for FVL mutation (g.1691 G>A; p.Arg506Gln) was done by adapting a PCR-RFLP (polymerase chain reaction-restriction fragment length polymorphism) protocol originally described by Bertina et al in 1994. 20 Genotyping for prothrombin G20210A mutation was done by adapting a PCR-RFLP protocol originally described by Ferraresi et al in 1997. 21 Genotyping for the VKORC1 -1639 G>A mutation was done using a PCR-RFLP assay, as described previously. Briefly, a 290-bp fragment was obtained by PCR using the following primers: forward 5′-GCCAGCAGGAGAGGGAAATA-3′ and reverse 5′-AGTTTGGACTACAGGTGCCT-3′. Enzyme digestion with MspI yielded 2 fragments in the case of the G allele while the A allele remained uncut. 22 Genotyping for the PAI-1 -675 4G/5G polymorphism was done by a PCR-RFLP assay, as previously described Brown et al. 23 Briefly, a 98-bp (for 4G allele) or 99-bp (for 5G allele) fragment was obtained by PCR, using the following primers: forward 5′-CACAGAGAGAGTCTGGCCACGT-3′ and reverse 5′-CCAACAGAGGACTCTTGGTCT-3′. Upon digestion with the BseLI restriction enzyme, the 5G allele was cut into 2 fragments, 77 and 22 bp, while the 4G allele remained uncut. 23
Statistical analysis was performed using the SPSS (version 21, Chicago, Illinois). Data were classified as nominal (categorical) or quantitative. Frequency and percentage were used to describe nominal variables. The Kolmogorov-Smirnov test was used to determine the normal distribution of continuous variables. The median and the 25th and 75th percentiles were used to describe quantitative variables. The Mann-Whitney U test was used to determine the differences between 2 independent groups of quantitative variables. The chi-square test or Fisher exact test were used to determine the difference in frequency between 2 groups of nominal variables. Deviations of allelic frequencies from Hardy-Weinberg equilibrium were calculated using the chi-square test. In the group with DVT, 3 patients were homozygous for the FVL mutation, and they were added to the heterozygous group as a result of statistical analysis requirements. Multivariate analysis was performed using binary logistic regression. Multivariate analysis included variables that showed statistical significance when using univariate analysis. The level of statistical significance was set at P < .05.
Results
Clinical and laboratory data recorded in both groups can be observed in Table 1. The Hardy-Weinberg equilibrium was observed in both the control group and the group with DVT when FVL mutation (P = .624; P = .427), prothrombin mutation (P = .735; P = .714), and VKORC1 -1693 G>A polymorphism (P = .085; P = .050) detection were performed.
Characteristics of Patients With DVT and Controls.
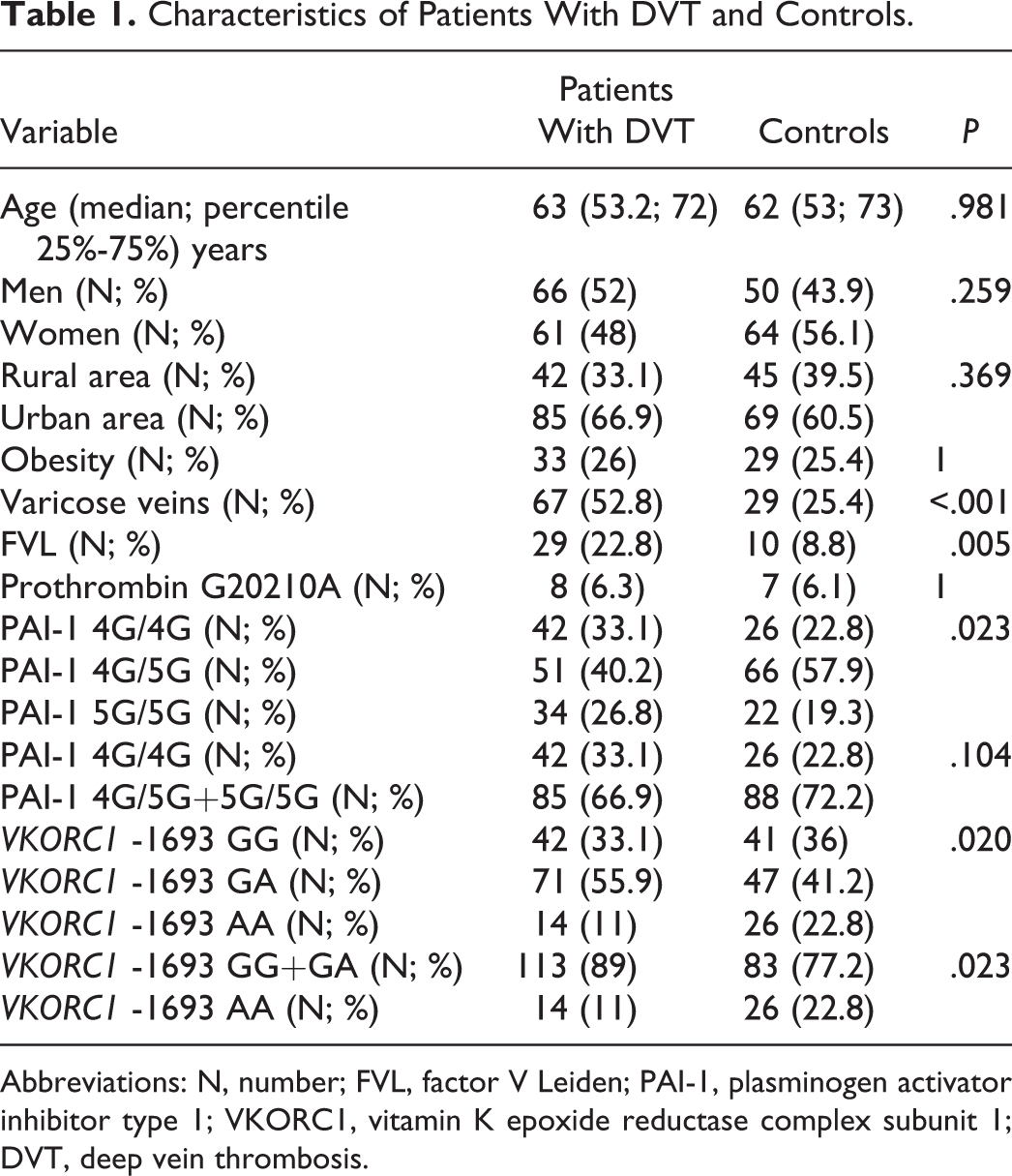
Abbreviations: N, number; FVL, factor V Leiden; PAI-1, plasminogen activator inhibitor type 1; VKORC1, vitamin K epoxide reductase complex subunit 1; DVT, deep vein thrombosis.
G allele frequency of the VKORC1 -1693G>A polymorphism in the group of patients with DVT was 0.61, while A allele frequency was 0.39. In the control group, G allele frequency was 0.56 and A allele frequency was 0.44. There was no statistically significant difference between groups in the distribution of alleles.
The VKORC1 -1693 G>A AA genotype was simultaneously found with FVL in 2 (1.6%) patients with DVT and in 2 (1.7%) controls, while neither the AA genotype nor the FVL was present in 86 (67.7%) participants in the group with DVT and in 80 (70.1%) controls. The difference was not statistically significant (P = .902). In participants with FVL and without the AA genotype (27 [21.3%] patients and 8 [7%] controls), the odds ratio (OR) for DVT was 3.577 (95% confidence interval [CI] 1.552-8.245), compared to participants with neither the AA genotype nor FVL (P = .003). In participants with the AA genotype and without FVL (12 [9.4%] patients and 24 [21.1%] controls), OR for DVT was 0.391 (95% CI 0.186-0.825), compared to those with neither the AA genotype nor the FVL (P = .014).
Binary logistic regression was used to determine the independent association between variables and DVT (Table 2). The diagnosis of DVT was the dependent variable and the following were introduced as independent variables: varicose veins, FVL, the PAI-1 -675 4G/5G polymorphism, and the VKORC1 -1693G>A polymorphism. GG + GA genotypes were chosen as reference for the VKORC1 -1693G>A polymorphism, and 4G/5G+5G/5G genotypes were chosen as reference for the PAI-1 -675 4G/5G polymorphism. The presence of varicose veins and FVL increased independently the risk of DVT. The VKORC1 -1693 G>A AA genotype was associated with fewer cases of DVT.
Factors Independently Associated With Acute Lower Extremity DVT.
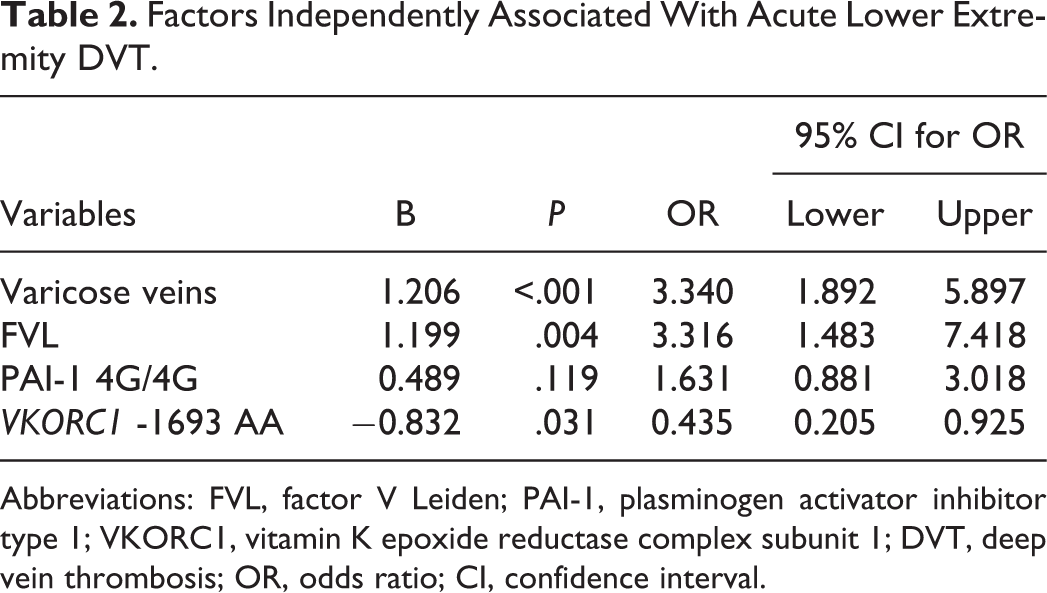
Abbreviations: FVL, factor V Leiden; PAI-1, plasminogen activator inhibitor type 1; VKORC1, vitamin K epoxide reductase complex subunit 1; DVT, deep vein thrombosis; OR, odds ratio; CI, confidence interval.
Discussions
Risk factors for DVT are a complex topic that has been extensively studied. The fact that one of the most feared complication of DVT, pulmonary embolism, is the number one cause of preventable hospital mortality gives utmost importance to this field of research. The decrease in the number of deaths due to pulmonary embolism in recent years demonstrates the importance of knowing the risk factors for DVT and establishing proper therapeutic measures for its prevention. 24 The most important genetic factors that work together and are involved in the occurrence of unprovoked DVT were first identified 20 years ago. 20,21 Mutations that reduce the risk of DVT are less known and their role is controversial.
Our study demonstrated the association between certain mutations and polymorphisms and the risk of acute DVT of the lower limbs: FVL, VKORC1 -1693 G>A, and PAI-1 -675 4G/5G polymorphisms. Another risk factor was the presence of varicose veins.
The VKORC1 (-1693 G>A) AA genotype was associated with a reduced risk of acute lower extremity DVT in both univariate analysis and independent of other genetic factors. Thus, in patients with this genotype, there was a 56.5% risk reduction. The different effect on the levels of vitamin K-dependent anticoagulant proteins (proteins C, S, and Z) and on certain procoagulant factors (factors II, VII, IX, and X) might explain the change in risk in patients where this variant genotype is found. Lacut et al have studied the influence of the VKORC1 1173 C>T polymorphism on the risk of DVT, and their conclusion was that the TT variant was associated with a reduced number of cases of DVT (OR = 0.62). 10 VKORC1 -1693 G>A and 1173 C>T polymorphisms are in complete linkage disequilibrium, therefore studies are comparable. C and T allele frequencies (0.6 and 0.4, respectively) in the group of patients with DVT in EDITH study were similar to G and A allele frequencies in patients with DVT in our study (0.61 and 0.39, respectively). In our study, G and A allele frequencies in the control group were significantly different (0.56 and 0.44, respectively) than those in the control group in EDITH study (0.63 and 0.37, respectively). Moreover, the AA genotype was more common in controls in our study than in those in the study carried out by Lacut et al (22.8% vs 16.2%). 10 This is a possible explanation for the difference in OR for the mutant genotype between the 2 studies. It is likely that when including more patients and controls in a study, this difference might diminish. Hindorff et al have demonstrated the existence of a relationship between VKORC polymorphisms and acute DVT. This study only included women who were slightly older than those in our study (68 years vs 63 years) and with significant cardiovascular comorbidities. 18 These differences in features may partly explain the contradictory results. Neither did Visser et al determine any impact of VKORC polymorphisms on the risk of acute DVT, although controls with the mutant genotype showed lower levels of procoagulant factors (factors II and VII) than those with DVT. 25
Factor V Leiden was an important risk factor for the occurrence of acute lower extremity DVT, with an odds ratio of 3.316. These results are consistent with those obtained in studies carried out in contemporary medical literature. Another study performed on the Romanian population demonstrated the increased incidence of idiopathic DVT in patients where FVL is present. 27 Prothrombin G20210A mutation was not associated with DVT in our study. No other study carried out on the Romanian population was able to determine a relationship between factor II mutation and acute DVT. 27 The PAI-1 -675 4G/5G polymorphism was associated with an increased frequency of DVT in patients with the 4G/4G genotype in univariate analysis, while multivariate analysis obtained a value close to statistical significance (P = .119). The meta-analysis conducted by Wang et al demonstrated the impact of the PAI-1 4G/5G polymorphism on the occurrence of unprovoked DVT but did not show any impact on the other type with significant risk factors. 26
The presence of varicose veins was a significant risk factor for DVT in our study. Other research works have also identified the impact of varicose veins on the risk of DVT. 28,29 Our study had several limitations: the number of patients limited by the inclusion criteria and the impossibility to determine the levels of vitamin K-dependent protein.
Conclusions
The study demonstrated the possible association between the VKORC1 -1693 polymorphism and acute lower extremity DVT. The presence of several important risk factors for the occurrence of acute DVT, such as FVL or varicose veins, did not influence this association.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was published under the frame of European Social Fund, Human Resources Development Operational Programme 2007-2013, project no. POSDRU/159/1.5/S/138776.