
Abstract
Objectives:
We examined the association between neutrophil to lymphocyte ratio (NLR) and the complexity of coronary artery disease assessed by SYNTAX score (SS).
Methods:
The study population included patients with chest pain who had undergone coronary angiography for stable angina pectoris. Patients were classified depending on whether the SS was 0 or SS > 0.
Results:
Left ventricular ejection fraction, estimated glomerular filtration rate, and NLR were found to be the independent predictors of high SS in multivariate analysis. The area under the receiver–operating curve of NLR was 0.72 (0.65-0.80, P < .001) for predicting high SS. The optimal cutoff value of NLR to predict high SS was 2.7 (sensitivity of 72% and a specificity of 61%). There was a significant correlation between NLR ratio and continuous SS (r = .552, P < .001).
Conclusion:
The NLR is a readily measurable systemic inflammatory marker and is associated with both the presence and the complexity of coronary artery disease.
Introduction
Although coronary artery disease (CAD) has been known to start with cell proliferation associated with endothelial damage, recent studies on atherosclerotic plaques show that it has a more complex pathophysiology wherein inflammatory process plays an important role in the onset and progression of the disease. 1 –3 It is a well-known fact that raised levels of inflammatory markers are associated with increasing rates of cardiac event in patients with CAD. 4 In addition, increased cardiovascular risk is related to white blood cell (WBC) count and its subtypes. Neutrophil to lymphocyte ratio (NLR) is a systemic inflammation marker that is correlated with mortality and cardiac events in many cardiovascular diseases such as stable CAD, unstable CAD, and acute decompensated heart failure. 5 –7
The SYNTAX score (SS) is an angiographic lesion-based scoring system originally invented to evaluate the complexity of CAD. 8 It is able to aid revascularization decisions and predict mortality and morbidity in patients with CAD. 9 Although predictive value of NLR in patients with stable CAD and ST-elevation myocardial infarction (STEMI) is well known, the relationship between NLR and the severity of CAD in patients with stable CAD has not been clearly determined.
In this study, we aimed to assess relationship between the severity of coronary atherosclerosis assessed by SS and NLR in patients with stable CAD.
Materials and Methods
The study population consisted of 649 consecutive patients who underwent coronary angiography for suspected or known coronary atherosclerosis between March 2010 and September 2010. All patients recruited in this study underwent coronary angiography for the presence of chest pain with objective signs of ischemia (treadmill exercise or myocardial single-photon emission computed tomography). Exclusion criteria were SS = 0 (n = 212), previous coronary artery bypass grafting(n = 66), percutaneous coronary intervention(n = 87), acute coronary syndrome (n = 201), clinically significant valvular heart disease (n = 28), significant congestive heart failure (n = 19), hematological disease (n = 5), cancer (n = 4), severe renal or liver disease (n = 19), ongoing infection or chronic inflammatory disease (n = 7), and autoimmune disease (n = 1). Finally, the study population consisted of 186 patients. All participants gave an informed consent and the study was approved by the local ethics committee.
Evaluations were visually performed by 2 experienced angiographers. Patients’ laboratory and clinical characteristics, such as age, sex, diabetes mellitus (DM), hypertension (HTN), hypercholesterolemia, smoking, family history of cardiovascular disease, height, and weight, were accessed through the medical records. In cases of inconsistencies, the patients were contacted through telephone. By dividing weight in kilograms by height in squared meters (kg/m2), the body mass index (BMI) was calculated.
Transthoracic echocardiography was performed in patients before they were discharged using a system V (Vingmed; GE, Horten, Norway) with a 2.5-MHz phased-array transducer. Recordings were taken in patients positioned in the left lateral decubitus position. The left ventricular ejection fraction (LVEF) was measured using modified Simpson rule.
Syntax Score
Syntax score is an angiographic tool used in grading the complexity of CAD. Each coronary lesion with a diameter stenosis ≥50%, in vessels ≥1.5 mm must be scored. The online latest updated version (2.1) was used in the calculation of the SSs (www.syntaxscore.com). 10 Syntax score, both numeric values of the score and tertiles (≤22, >22-≤32, >32) of the score were used.
Laboratory Data
In our hospital, the blood samples were collected from the antecubital vein by an atraumatic puncture prior to the coronary angiography and were sent to the laboratory for analysis within 1 hour after collection. Routinely, venous blood is collected in a tube containing K3 EDTA for measurement of hematologic indices in all patients undergoing the coronary angiography. Hemoglobin, total WBC, neutrophils, lymphocytes, and monocytes were determined using an automated blood cell counter by a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc Mervue, Galway, Ireland). Total low-density lipoprotein and high-density lipoprotein cholesterol, triglycerides, and fasting glucose were measured using the Abbott Architect C16000 auto analyzer (Abbott laboratories, Abbott park, IL, USA).
Definitions
Stable angina was defined as discomfort in the chest, jaw, shoulder, back, or arms, typically elicited by exertion or emotional stress, and relieved by rest or nitroglycerin. The HTN was defined as systolic blood pressure > 140 mm Hg and/or a diastolic blood pressure > 90 mm Hg, or use of antihypertensive medications. The diagnosis of DM was based on previous history of diabetes treated with or without medical therapy. Hypercholesterolemia was described as total cholesterol ≥ 200 mg/dL. The BMI was calculated by dividing the weight (kg) of an individual by the square of his or her height. A BMI value ≥ 30 kg/m2 was defined as obese. Current smokers were defined as having a history of smoking for a certain period within the past year. The glomerular filtration rate (GFR) was estimated by the simplified Modification of Diet in Renal Disease Equation. 11 Renal insufficiency was described as a GFR value <60 mL/min per 1.732 m2.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation. Categorical variables are expressed as percentages. To compare parametric continuous variables, analysis of variance or Kruskall-Wallis test were used. The chi-square test was used to compare the categorical variables. Multivariate logistic regression analysis was used to identify the independent predictors of high SS. All variables showing significance values <.05 in univariate analysis were included in the multivariate model. The receiver–operating characteristic (ROC) analyses were used to detect the cutoff value of NLR in prediction of high SS. Association between variables was tested using Spearman or Pearson correlation coefficient, when appropriate. Two-tailed P values <.05 were considered as statistically significant. Interobserver reproducibility was assessed by Bland-Altman analysis and intraobserver reproducibility was assessed by intraclass correlation coefficient. All statistical studies were carried out with the SPSS program (version 15.0, SPSS, Chicago, Illinois).
Results
The mean age of our 186 patients was 61.8 ± 11.1 years and 64% of the study population was male. The mean SS was 27 ± 11 (median, 24; range, 7-54). As 38.7% of the patients were of low SS group, 26.9% and 34.4% were of intermediate and high SS groups, respectively. Baseline clinical, biochemical, and angiographic characteristics relative to SS tertiles are shown in Table 1.
Baseline Characteristics According to Syntax Score Tertiles.
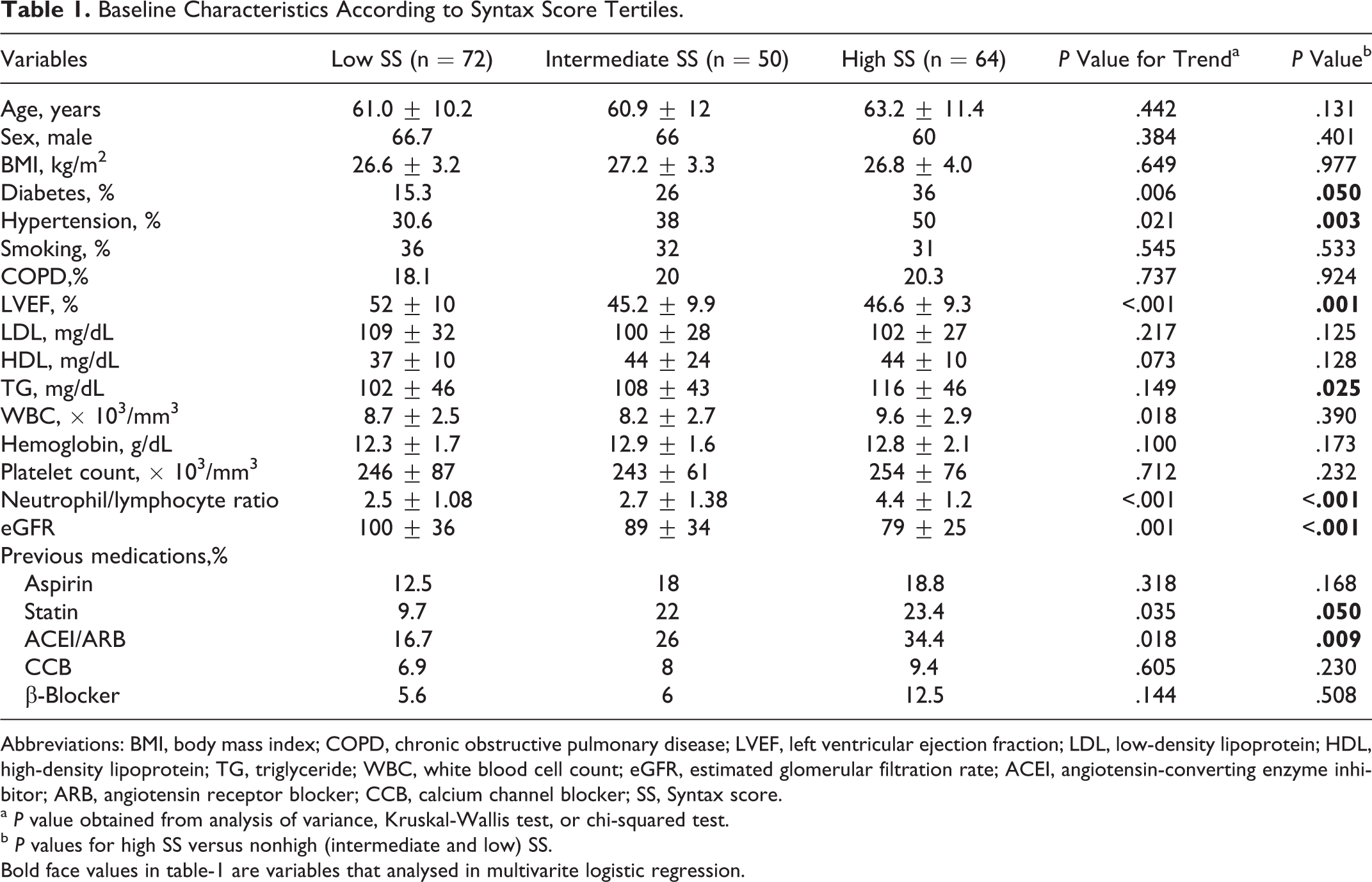
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglyceride; WBC, white blood cell count; eGFR, estimated glomerular filtration rate; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; SS, Syntax score.
a P value obtained from analysis of variance, Kruskal-Wallis test, or chi-squared test.
b P values for high SS versus nonhigh (intermediate and low) SS.
Bold face values in table-1 are variables that analysed in multivarite logistic regression.
The patients in the high SS group demonstrated higher DM and HTN frequency, lower LVEF, estimated GFR (eGFR), and higher TG and NLR when compared to the other SS tertiles. Furthermore, history of previous statin and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use was more common in the high SS group. Detailed NLR values relative to SS tertiles are shown in Figure 1.
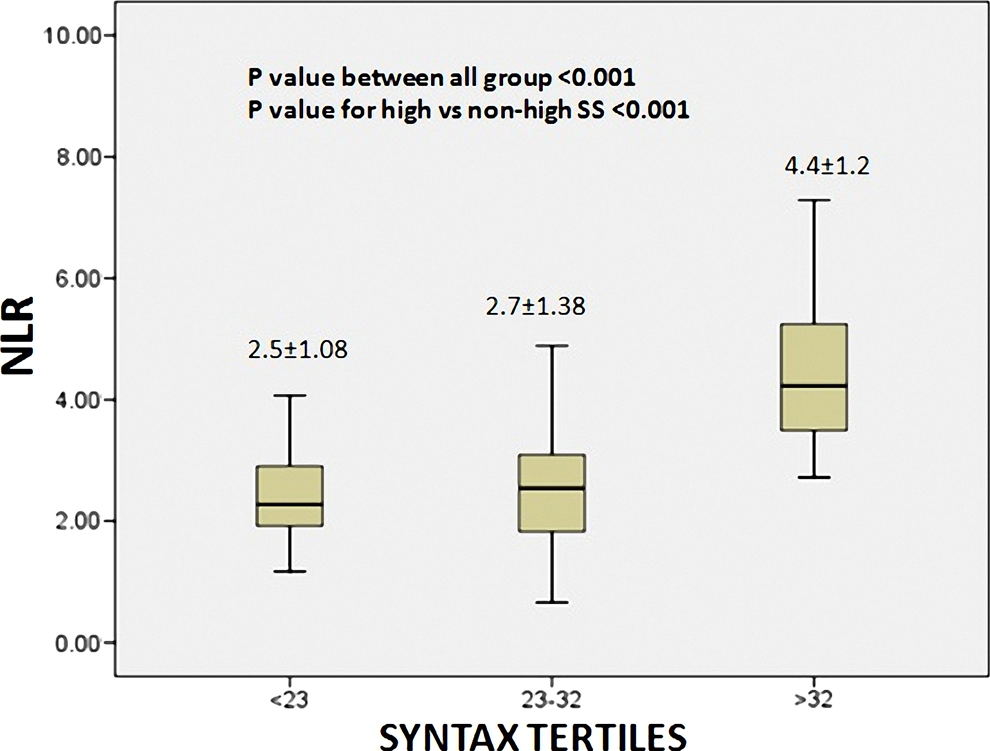
Neutrophil to lymphocyte ratio (NLR) values according to Syntax score.
In order to determine the predictors of high SS, the variables found to be significantly different in the univariate analysis were included in the multivariate logistic analysis. As a result; LVEF (odds ratio [OR], 0.94; 95% confidence interval [CI], 0.91-0.98; P = .004), eGFR (OR, 0.97; 95% CI, 0.96-0.99; P < .001), and NLR (OR, 1.67; 95% CI, 1.25-2.24; P < .001) were found to be the independent predictors of high SS (Table 2). The area under the ROC curve of NLR was 0.72 (0.65-0.80, P < .001) for predicting high SS (Figure 2). The optimal cutoff value of NLR to predict high SS was 2.7. Any NLR value higher than 2.7 has a sensitivity of 72% and a specificity of 61%. There was a significant correlation between NLR ratio and continuous SS (r: .552, P < .001; Figure 3).
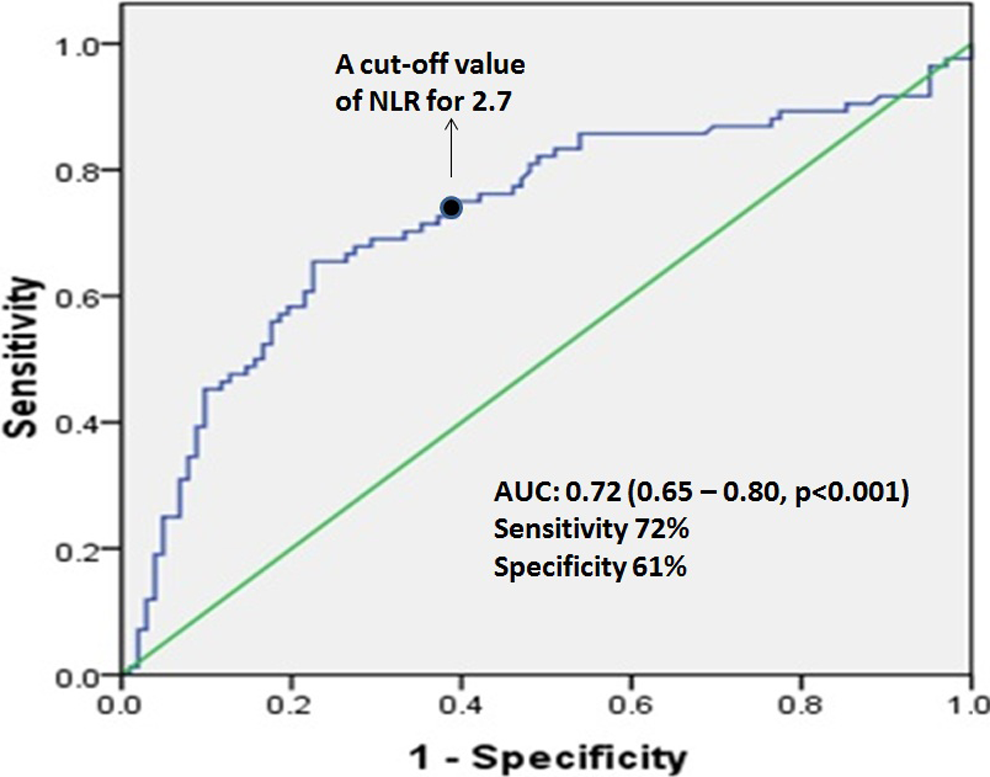
Receiver–operating characteristic (ROC) curves for neutrophil to lymphocyte ratio (NLR) values in prediction of high Syntax score.
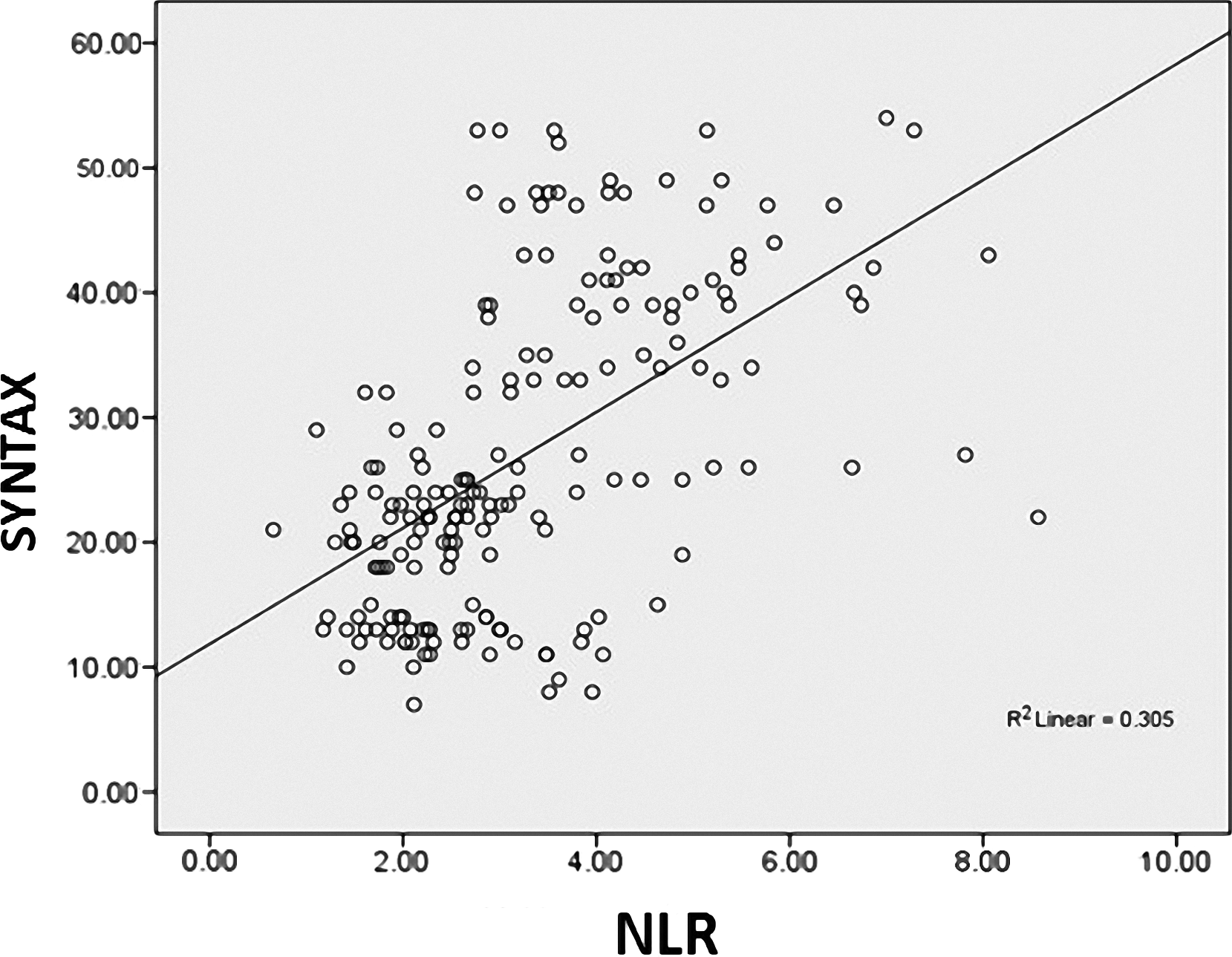
Correlation plot between Syntax score and neutrophil to lymphocyte ratio (NLR).
Logistic Regression Analysis to Determine the Independent Predictors of High Syntax Score.
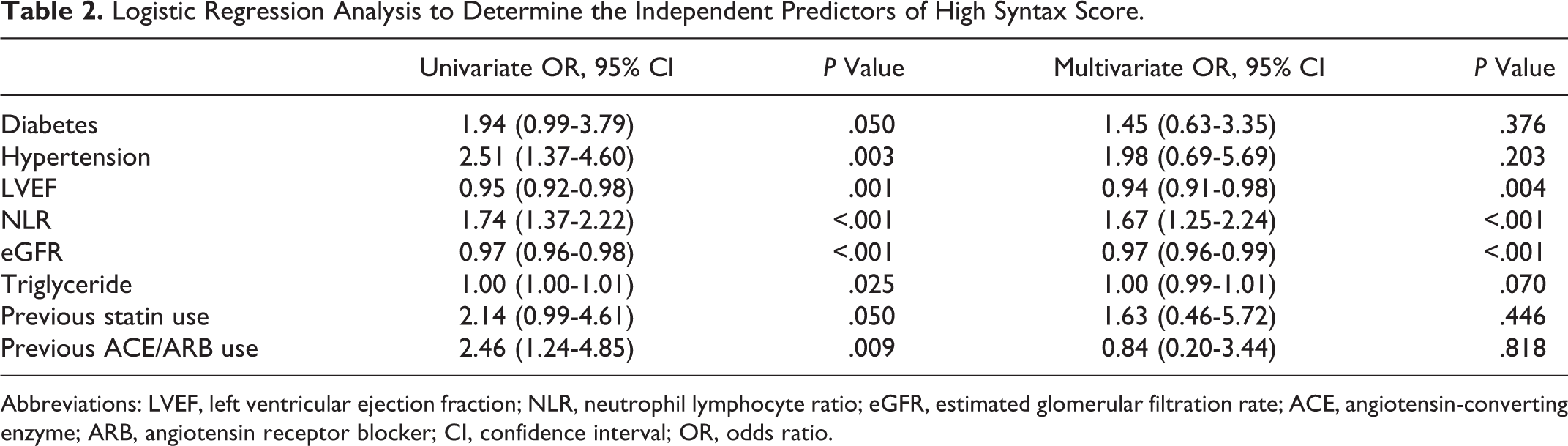
Abbreviations: LVEF, left ventricular ejection fraction; NLR, neutrophil lymphocyte ratio; eGFR, estimated glomerular filtration rate; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CI, confidence interval; OR, odds ratio.
In agreement analysis on 30 randomly selected patients, there were good interobserver (mean difference: 3.3 [95% limits of agreement −2.9, 6.3]) and intraobserver reproducibility (intraclass correlation coefficient 0.91, 95% CI 0.85-0.96) for SS.
Discussion
In the present study, we demonstrated the relation of NLR with the severity and complexity of CAD assessed by SS in stable patients with CAD who underwent coronary angiography. To our knowledge, the present study is the first report evaluating the relationship of NLR with the severity and complexity of CAD by SS in patients with stable CAD.
Although cell proliferation secondary to endothelial damage has been recognized as the triggering reason for the formation of atherosclerotic lesions, today it has been shown that many factors are involved alongside inflammatory process in the onset and progression of this event. 1,12 In addition to their role in the onset of atherosclerosis, inflammatory cells are also known to play a part in plaque rupture and formation of thrombosis in acute coronary syndromes. 2 Mortality rate rises with increasing levels of inflammation markers in both healthy individuals and symptomatic and/or asymptomatic patients with CAD. 4,13 Therefore, many inflammation markers such as WBC, C-reactive protein (CRP), and homocysteine are used in the prediction of ischemic cardiovascular events in asymptomatic patients. 5
As shown for CRP, 14 WBC and its subtypes are also known to be markers of inflammation in cardiovascular diseases. 15 The NLR, known as a systemic inflammation marker, has been shown to have the greatest predictive power for adverse outcome in patients with or at high risk of CAD. 16,17 Neutrophil infiltration, both in the atherosclerotic plaques of animal models and in the responsible plaques and infarct zones of patients with acute CAD, indicates that they are involved in each stage of this process. Furthermore, lymphocytes have been demonstrated to play a significant role in atherosclerosis, as well. 18 Since NLR is measured by proportioning 2 inflammatory markers (neutrophil and lymphocyte), it has a stronger predictive value. 17 Umesh et al studied 2833 patients hospitalized with the diagnosis of acute coronary syndrome (cases of STEMI, non-STEMI, and unstable angina) and observed higher increases in inhospital and 6-month mortality rates in the group with highest NLR. In this study, NLR was highest in patients with STEMI as well as in those who were less on drugs such as aspirin, β-blockers, and statins. 6 In a study including patients with ST elevation, the increasing level of NLR within the first 96 hours of the onset of symptoms was found to be associated with 2.5- to 4.2-fold increases in mortality. 17 In another study which consisted of patients with STEMI who underwent early intervention (within the first 12 hours), raised NLR was observed to be correlated with increasing mortality during both hospital stay and long-term follow-up (mean, 5.2 years). 19
Similarly, Papa et al studied 422 participants with stable CAD and after a follow-up period of 3 years, they observed that raised NLR, widely recognized as an indicator of systemic inflammation, was associated with higher mortality. 20 In the present study, NLR was found to have a significant relationship with the severity and complexity of CAD in patients with stable CAD. In consistence with our study, Kaya et al evaluated 172 cases of CAD by coronary angiography while assessing the severity of the disease by Gensini score, and they revealed a significant relationship between the NLR and the severity of CAD. When NLR was above 2.5, it was observed to have a sensitivity of 62% and specificity of 69% for the severity of atherosclerosis. 21 Unlike this study, we evaluated the severity of CAD by SS and observed higher sensitivity and specificity values when NLR was >2.7. In addition, Sahin et al demonstrated that NLR was significantly correlated with severity of CAD assessed by SS in patients with STEMI. 18
Similar to CRP, an inflammation marker that shows a correlation with cardiac mortality, NLR appears to be a promising marker that might be used more commonly in the follow-up of patients with CAD in the near future.
Limitations
This is an observational, single-institution study with a relatively small sample size and was thus subject to various unaccounted confounders inherent in such an analysis. Additionally, we could not compare NLR with other inflammatory markers, such as CRP, fibrinogen, or myeloperoxidase, because they were not routinely obtained in our study population.
Conclusion
The NLR is a readily measurable systemic inflammatory marker that is independently associated with the presence and complexity of stable CAD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.