
Abstract
Objective: To analyse the outcome of cerebral venous thrombosis (CVT) patients presenting with isolated headache, specifically to compare isolated headache patients with early vs. late CVT diagnosis.
Method: In the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT) database we compared the outcome of patients with isolated headache and a CVT diagnosed early (≤7 days from onset) vs. late (>7 days). We retrieved 100 patients with isolated headache, 52 patients with early CVT diagnosis (early isolated headache) and 48 with late CVT diagnosis (late isolated headache).
Results: Neurological worsening was more frequent within early isolated headache patients (23% vs. 8%) (p = 0.045). At the last follow-up (median 411 days), 93% patients had a complete recovery, and 4% were dead or dependent, with no significant difference between early isolated headache and late isolated headache.
Conclusion: The outcome of CVT patients with isolated headache diagnosed early or late was similarly favourable, but there was a higher proportion of neurological worsening in the acute phase among early isolated headache patients, who need close neurological monitoring.
Introduction
Headache is the most frequent and often the first symptom of cerebral venous thrombosis (CVT) (1–3). CVT patients whose clinical manifestations are limited to headache (isolated headache) and other features of the intracranial hypertension syndrome have been described as having a favourable outcome (4). However, CVT patients with isolated headache and isolated intracranial hypertension syndrome come to medical attention and are diagnosed significantly later than those with other more dramatic presenting syndromes, such as focal neurological deficit and encephalopathy (5,6). It is therefore possible that the good prognosis attributed to CVT patients with isolated headache is due to a selection bias. Patients with isolated headache who present and are diagnosed at an early stage can still deteriorate neurologically, eventually having a less favourable prognosis, whereas CVT patients with isolated headache who are diagnosed one or two weeks after the onset of symptoms have more tolerable symptoms and have not yet developed other neurological manifestations besides headache before the diagnosis of CVT.
In this study we investigate whether the outcome of CVT patients with isolated headache depends on the time interval between the onset of symptoms and the diagnosis of CVT.
Participants and methods
We used data from the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT) cohort, a multinational observational study that described clinical presentation, predisposing conditions, treatments and outcome in 624 consecutive symptomatic patients with CVT (2). From the ISCVT cohort, we selected patients who presented clinically with isolated headache. We used a clinical definition of isolated headache, as can be formulated by a general physician. Therefore, we excluded from the definition of ‘isolated headache’ only patients with other major neurological symptoms (focal neurological deficits, visual loss, seizures, decreased consciousness, altered mental state) and with diplopia or meningeal syndrome, but accepted those with headache accompanied by vomiting, transient visual symptoms, tinnitus and papilloedema. We did not exclude patients with papilloedema because papilloedema can be diagnosed only by fundoscopy, which is a technique not mastered by many medical doctors. We also did not include in the clinical definition of ‘isolated headache’ the results of subsequent ancillary procedures, and thus did not exclude patients with brain lesions on CT/MR, or elevated CSF cell count on lumbar puncture.
To define isolated headache diagnosed early and late in the course of CVT, we used the median delay (7 days) between the onset of the symptoms and the diagnosis of CVT in the ISCVT cohort (6). Thus, when the delay was up to 7 days patients were classified as having an ‘early isolated headache’ (EIH), and when the delay was more than 7 days they were classified as ‘late isolated headache’ (LIH).
We analysed the following outcomes: 1) survival and functional outcome at 6 months and at last available follow-up; 2) death within 30 days from the onset; 3) neurological worsening during the acute phase (neurological worsening was defined as either depressed consciousness, altered mental state, new focal neurological deficit, new seizure or visual loss (7)); and 4) new brain lesion on a repeated CT/MR performed in the acute phase. The outcome was classified according to the modified Rankin Scale (mRS) (0 to 6) (2), and was categorized as follows: complete recovery as mRS 0 to 1, partial recovery but independent as mRS 2, death or dependent as mRS 3 to 6 (8).
We compared the two groups (EIH vs. LIH) with respect to outcome and also for the baseline variables that could be predictors or influence the outcome, such as age, gender, aetiology, location of the thrombosis and treatment, using chi-square statistics, with continuity correction or the Fisher’s exact test when appropriate. When there were at least ten outcome events, multivariable analysis (dichotomic logistic regression analysis, backward method) to predict an outcome was performed, entering the two classes of median delay and variables with significant associations with the outcome in bivariable analysis. In addition, we performed two sensitivity analyses comparing the outcomes of the two groups, one excluding the patients who presented brain lesions in their admission CT/MR, and another excluding patients with papilloedema, to assess whether these variables influenced the results.
Results
From the 624 cases of the ISCVT cohort, 100 patients fulfilled the inclusion criteria and the exclusion criteria for this study. Of these, 29 had papilloedema and 18 had brain lesions on the admission CT/MR. There were 52 patients in the EIH group and 48 patients in the LIH group.
Comparison of early and late isolated headache groups at baseline
Baseline characteristics

N indicates total number of patients; EIH, early isolated headache; LIH, late isolated headache. p values were calculated using chi-square statistics with continuity correction or Fisher’s exact test when appropriate.
Eighty-eight patients were treated with intravenous heparin or subcutaneous low-molecular-weight heparin in therapeutic dosages, 90.4% in the EIH group and 85.4% in the LIH group (p = 0.45).
Outcome
Last follow-up (median 411 days) was primarily performed at outpatient clinics (64%), 30% of patients were contacted by phone, and in 6% follow-up information was obtained by other means of communication.
Sixteen patients (16%) experienced clinical worsening (Figure 1). Worsening was more frequent in patients with isolated headache and early CVT diagnosis (12 patients, 23.1%) than in patients with isolated headache and late CVT diagnosis (4, 8.3%) (p = 0.045). There was no significant difference between the groups regarding the proportion of patients who developed depressed consciousness (p = 0.32), altered mental state (p = 1), new seizure (p = 0.27), or visual loss (p = 1). New focal deficits appeared in nine patients, all with early CVT diagnosis (p = 0.008) (Table 2). On logistic regression with clinical worsening as outcome, the odds ratio (95% confidence interval) for early CVT diagnosis adjusted for any lesion on CT/MR, more than one occlusion and superior sagittal sinus thrombosis was 1.92 (0.52–7.1).
Type of neurological worsening in patients with isolated headache diagnosed early (EIH) and late (LIH). Numbers indicate proportions (%). Outcome in isolated headache diagnosed early and late N indicates total number of patients; EIH, early isolated headache; LIH, late isolated headache. pP values were calculated using chi-square statistics with continuity correction or Fisher’s exact test when appropriate. mRS: modified Rankin Scale.
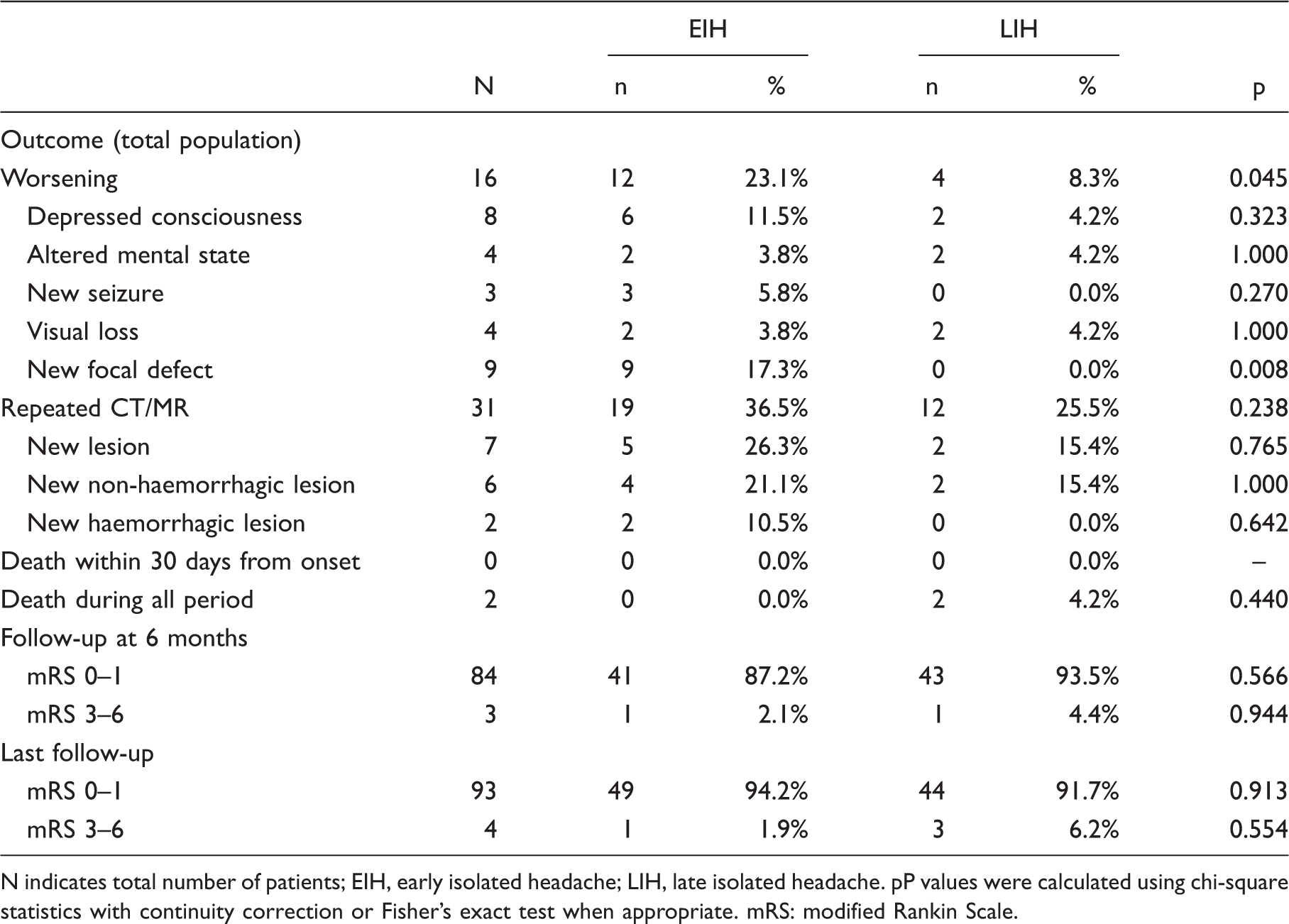
Among the 31 patients who repeated the CT/MR examination, six had a new visible lesion with no difference between the two groups.
Modified Rankin Scale distribution in isolated headache diagnosed early and late

N indicates total number of patients; EIH, early isolated headache; LIH, late isolated headache. p values were calculated using chi-square statistics with continuity correction or Fisher’s exact test when appropriate. mRS: modified Rankin Scale.
Sensitivity analysis
Outcome excluding patients with lesions on CT/MR
Of 81 patients without brain lesions on their admission CT/MR, only nine patients had clinical worsening (four with depressed consciousness, three with altered mental state, one with a new seizure, three with visual loss, and four with a new focal neurological deficit). Although there were no significant differences between the two groups, there was still a trend for patients in the EIH group to develop new focal neurological deficits (four patients vs. none in the LIH) (p = 0.085). No significant differences were found between the two groups concerning any of the other outcomes.
Outcome excluding patients with papilloedema
Of the 69 patients without papilloedema, 14 experienced clinical worsening (depressed consciousness in six patients, altered mental state in three patients, new seizure in three patients, visual loss in four patients and a new focal neurological deficit in seven patients). There were no significant differences between the two groups, but there was still a trend for new focal defects to appear in the EIH (seven vs. none in the LIH group) (p = 0.079). No significant differences were found between both groups concerning any of the other outcomes.
Discussion
This study was based on a large cohort of CVT patients and demonstrated that the vast majority of patients with isolated headache had a complete recovery and none died in the acute phase. This was observed both for those diagnosed early (EIH) and late (LIH) in the course of CVT. No significant difference was found between EIH and LIH concerning acute or long term outcomes. The important exception was neurological worsening after admission, which was significantly more frequent in the EIH group. Patients who developed new focal neurological signs were all in the EIH group.
Strengths of this study include the multicentre cohort design, which decreases bias, especially inclusion bias, and increases the external validity of the results. Follow-up information was obtained for all patients, predominantly by direct interview. A limitation of the study is the difficulty to ascertain the exact day of onset of the symptoms of CVT, which often does not have an acute onset. We used a definition of isolated headache from the perspective of a general physician, based on clinical symptoms and signs from onset to hospital admission. Other authors have used a more strict definition, requiring the absence of papilloedema, normal CSF exam and no brain lesions on CT/MR (9). In this study we used a clinical definition of isolated headache syndrome based on the clinical presentation of patients, without including information from subsequent ancillary examinations (fundoscopy, lumbar puncture and neuroimaging), which may not be always performed. For this reason we did not exclude patients with papilloedema, lesions on CT/MR, or elevated CSF count.
Concerning statistical limitation, although the sample size was large, the number of outcome events was in general low, precluding multivariable analysis. Also we did not adjust for multiple comparisons, because our main concern was not to miss a potential difference in outcome between the two groups, which would have consequences regarding the safety of the patients.
Brain lesions in CVT are caused by venous occlusion and are associated with a higher risk of unfavourable outcome (8,10). Usually parenchymal lesions on CT/MR cause seizures or focal deficits, but in some cases an isolated headache is the only symptom. This was mainly observed in the EIH group. In our study 16% of all patients deteriorated. As expected, worsening was more frequent in the EIH group (23.1%). The most common deterioration was a new focal neurological deficit, caused most probably by a new lesion as shown on repeated CT/MR. When we excluded all patients with lesions on CT/MR, a significant difference was no longer found between both groups, which demonstrates that brain lesions have an important role in the immediate outcome or are an indicator of more severe venous obstruction. In fact, thrombosis at multiple sites and occlusion of the superior sagittal sinus were more frequent among patients with early CVT diagnosis.
Despite the limitations of the study, our findings may have practical clinical importance, because patients presenting early (before CT/MR has been performed) after symptom onset with isolated headache caused by CVT seem to have a higher risk of neurological deterioration. They should be promptly evaluated and, if a CVT diagnosis is confirmed, they should be clinically monitored and repeatedly examined for new focal neurological signs.