
Abstract
Objectives:
We aimed to investigate the relationship between red cell distribution width (RDW) value and coronary collateral circulation (CCC) in patients with non-ST elevation myocardial infarction (NSTEMI).
Methods:
The study population consisted of 322 consecutive patients with NSTEMI. The patients were classified into impaired CCC (group 1, Rentrop grades 0-1) or good CCC (group 2, Rentrop grades 2-3). Baseline RDW was measured as part of the automated complete blood count.
Results:
The RDW values were significantly higher in patients with impaired CCC than in those with good CCC (17.2 ± 2.3 vs 14.5 ± 2.5, P < .001). In multivariate logistic regression analysis, RDW (odds ratio: 1.52, 95% confidence interval: 1.30-1.78, P < .001), baseline creatine kinase MB (CK-MB), and absence of preinfarction angina were found to be the independent predictors of impaired CCC. In receiver–operating characteristic curve analysis, the RDW value >15.5 yielded an area under curve value of 0.783, with 77% sensitivity and 73% specificity.
Conclusions:
Our study results demonstrated that, high RDW, high CK-MB, and absence of preinfarction angina were found to be independent predictors of impaired CCC.
Introduction
Coronary collateral circulation (CCC) is an adaptive response to myocardial ischemia. 1 There are many collateral coronary arteries connecting the normal coronary arteries in individuals without angiographic coronary artery disease (CAD); however, most of these are not angiographically visible. 2,3 Patients with coronary stenosis or occlusion develop varying degrees of visible CCC. A well-developed CCC is associated with reduced infarction area and better ventricular functions. 4,5 Red cell distribution width (RDW) is a marker that has been shown to be correlated with adverse cardiovascular events, both in the short- and long term and associated with clinical conditions in various cardiovascular diseases. 6 –10 There is no study investigating the relationship between RDW and CCC to date. Therefore, in this study, we aimed to investigate the relationship between RDW value and CCC in patients with non-ST elevation myocardial infarction (NSTEMI).
Methods
Study Population
The study population consisted of 322 consecutive patients with NSTEMI who underwent coronary angiography at our hospital. The study was approved by the institutional ethics committee. The patients with baseline anemia (a hemoglobin level <13 g/dL in men and <12 g/dL in women; n = 32), history of blood transfusion within the last 3 months (n = 4), coronary angiogram showing a lesion of <80% stenosis (n = 66), active and ongoing infection (n = 12), chronic inflammatory disease (n = 4), and history of percutaneous coronary intervention (PCI; n = 17) or coronary artery bypass grafting (n = 11) were excluded from the study. Finally, 176 patients with NSTEMI were included in our study.
The clinical risk factors for the patients such as age, gender, hypertension (HTN), diabetes mellitus (DM), history of hyperlipidemia, smoking status, and family history were noted. Furthermore, on admission, each patient was evaluated for blood pressure, heart rate, Killip class, presence of cardiogenic shock, previously used drugs, presence of preinfarction angina, high sensitivity C-reactive protein (hs-CRP), serum creatinine, glucose, lipid profile, and hematologic indices. Prior to the PCI, each patient underwent transthoracic echocardiography using the biplane Simpson method and left ventricular ejection fraction (LVEF) was measured. Hematologic indices such as hemoglobin, white blood cell, RDW, mean platelet volume, and platelet counts were measured as part of the automated complete blood count (CBC) using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). Anemia on admission was defined as a baseline hemoglobin concentration less than 13 mg/dL in men and less than 12 mg/dL in women, in accordance with the World Health Organization criteria. 11 Hypertension was defined as systolic pressure >140 mm Hg and/or a diastolic pressure >90 mm Hg at least 2 times or if the individual was taking antihypertensive medications. The diagnosis of DM was based on the previous history of diabetes treated with or without drug therapies. Current smokers were defined as those who had smoked for some period during the past year.
Coronary Angiography
Quantitative coronary angiography was performed using standard Judkins method via transfemoral route. The inclusion criteria were the presence of 80% or greater degree of diameter stenosis in at least 1 coronary artery in coronary angiography. Therefore, since development of CCC is known to be inadequate in patients not complying with this criterium, 12 they were excluded from the study. The coronary collateral circulation was graded according to the Rentrop classification. 12 Accordingly, Grade 0 classified as no filling; Grade 1 classified as filling of side branches via collateral channels without visualization of the epicardial segment; Grade 2 classified as partial filling of the epicardial major coronary artery via collateral channels; and Grade 3 classified as complete filling of the epicardial major coronary artery. In patients with more than 1 coronary lesion, when there was more than 1 CCC, the CCC with the highest Rentrop grade was used. Thrombolysis in myocardial infarction (TIMI) flow grade and TIMI myocardial perfusion grade (TMPG) were measured as described before. The patients were classified into impaired CCC (group 1, Rentrop grades 0-1) or good CCC (group 2, Rentrop grades 2-3). Multivessel disease was defined as the presence of a lesion in 2 or more major epicardial arteries. Distal embolization was defined as distal filling defect with an abrupt “cutoff” in one or more peripheral coronary branch of interventional artery. Both TIMI flow grade and TMPG were measured as described before. 13,14
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation whereas categorical variables are expressed as percentage. Comparisons between 2 CCC groups were made using the Student t test or Mann-Whitney U test or chi-square tests, as appropriate. Comparison between Rentrop grades were made using the analysis of variance and Tukey honestly significant difference test was chosen as a post hoc test. Multiple logistic regression analysis was performed to identify the independent predictors of CCC using variables showing marginal association with it on univariate testing (P < .10). Receiver–operating characteristic (ROC) analyses were used to detect the cutoff value of RDW in the prediction of CCC. Correlation analyses between variables were performed using Pearson or Spearman correlation. A P value <.05 was considered significant. All statistical analyses were carried out using SPSS 17.0 for Windows (SPSS Inc, Chicago, Illinois).
Results
A total of 176 patients with NSTEMI (mean age was 61.3 ± 12.3 years and male ratio was 57.4%) were included in the study. Table 1 shows the comparison of groups 1 and 2 relative to baseline characteristics. Compared to the patients with good CCC, patients with impaired CCC exhibited higher frequency of DM and lower preinfarction rates, as well as lower LVEF, higher neutrophil/lymphocyte ratio (NLR), hs-CRP, baseline creatine kinase MB (CK-MB) along with higher degree of impaired myocardial perfusion.
Baseline Characteristics According to Coronary Collateral Circulation.
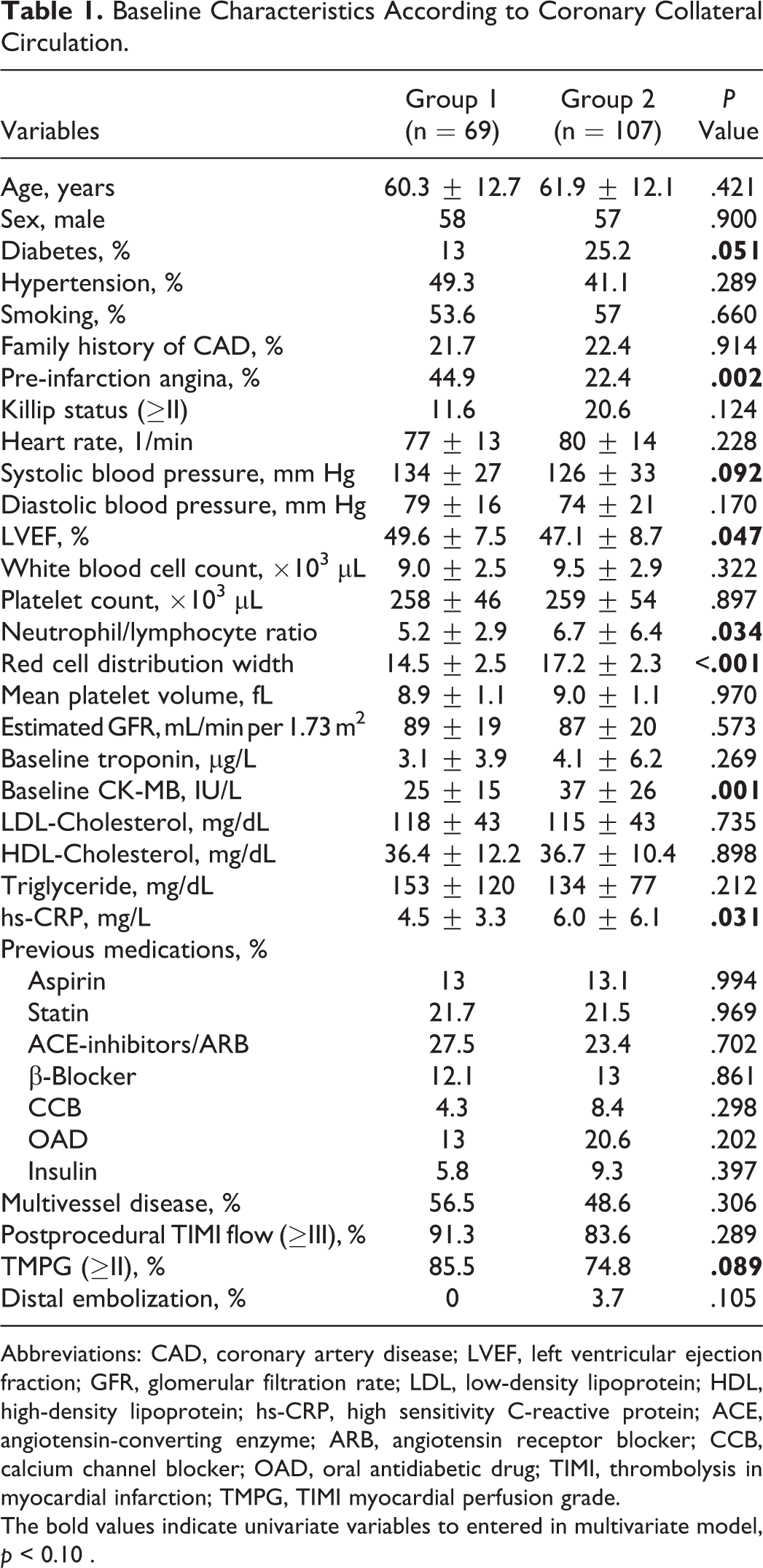
Abbreviations: CAD, coronary artery disease; LVEF, left ventricular ejection fraction; GFR, glomerular filtration rate; LDL, low-density lipoprotein; HDL, high-density lipoprotein; hs-CRP, high sensitivity C-reactive protein; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; OAD, oral antidiabetic drug; TIMI, thrombolysis in myocardial infarction; TMPG, TIMI myocardial perfusion grade. The bold values indicate univariate variables to entered in multivariate model, p < 0.10 .
Compared to the patients with good CCC, the patients with impaired CCC manifested significantly higher RDW values (17.2 ± 2.3 vs 14.5 ± 2.5, P < .001). Furthermore, Rentrop grade 2 and 3 patients had significantly lower RDW values when compared to the Rentrop grade 0 and 1 patients (13.3 ± 2.5, 14.8 ± 2.5, 16.6 ± 2.4, 18.2 ± 1.8, respectively, P value for trend <.001). Although RDW values were lower in Rentrop grade 1 patients than in Rentrop grade 0 patients (P = .004), there was no difference between Rentrop grade 2 and Rentrop grade 3 patients (P = .122; Figure 1).
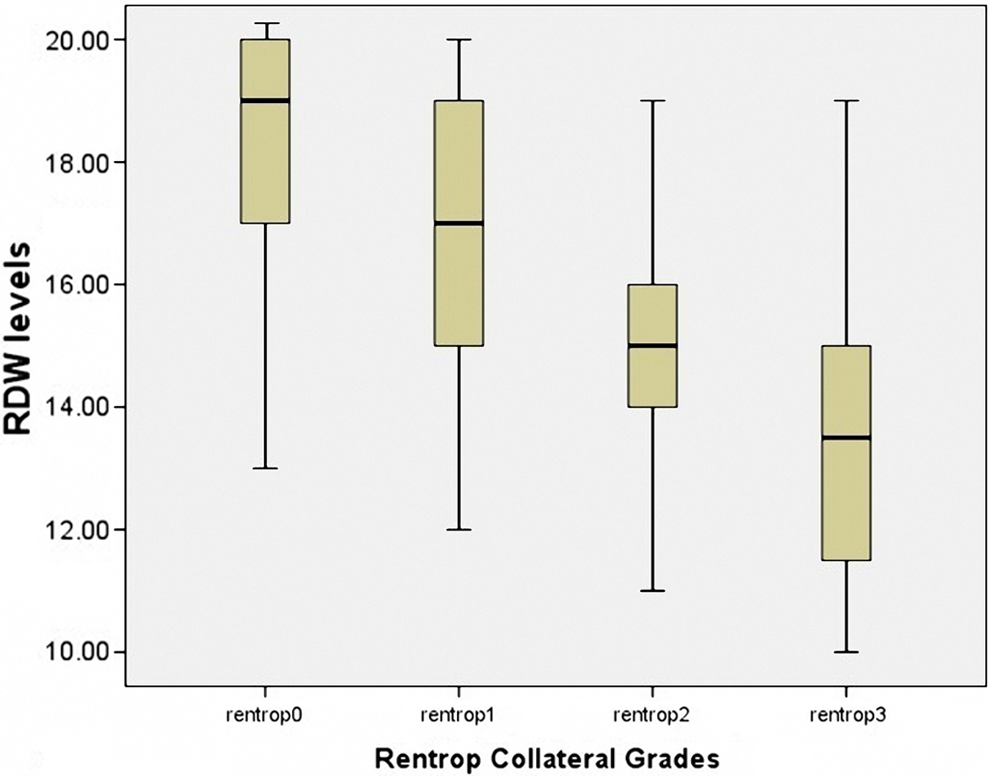
Red cell distribution width (RDW) value according to Rentrop grades.
Multivariate logistic regression test was employed for determining the independent predictors of impaired CCC. The variables that were found to have significance in the univariate analysis (pre-infarction angina, diabetes, LVEF, hs-CRP, NLR, RDW, baseline CK-MB, and TMPG) were included in the multivariate model. Among those, RDW (odds ratio [OR]: 1.52, 95% confidence interval [CI]: 1.30-1.78, P < .001), baseline CK-MB (OR: 0.96, 95% CI: 0.93-0.99, P = .008), and presence of preinfarction angina (OR: 0.23, 95% CI: 0.10-0.54, P = .001) were found to be the independent predictors of impaired CCC (Table 2). The ROC curve analysis was performed to detect the best cutoff value of RDW in the prediction of impaired CCC. The RDW value >15.5 yielded an area under curve value of 0.783 (95% CI: 0.713-0.853; P < .001). Furthermore, RDW value >15.5 demonstrated a sensitivity of 77% and specificity of 73% for the prediction of CCC (Figure 2).
Multivariate Logistic Regression Analysis to Detect the Independent Predictors of Impaired Coronary Collateral Circulation.
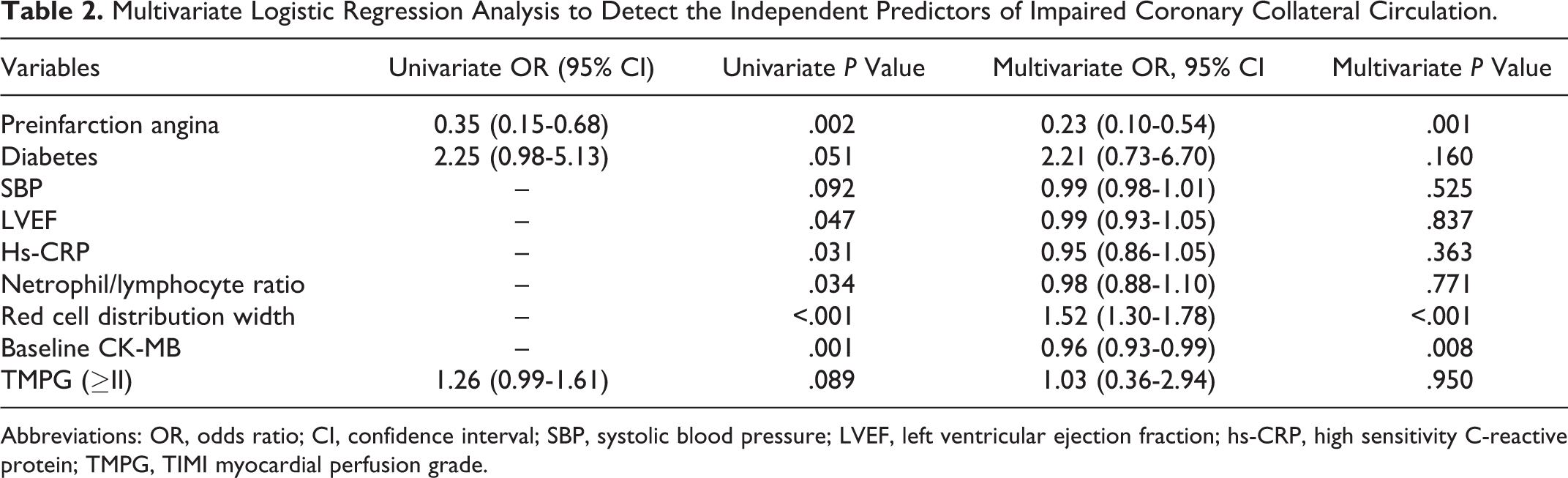
Abbreviations: OR, odds ratio; CI, confidence interval; SBP, systolic blood pressure; LVEF, left ventricular ejection fraction; hs-CRP, high sensitivity C-reactive protein; TMPG, TIMI myocardial perfusion grade.
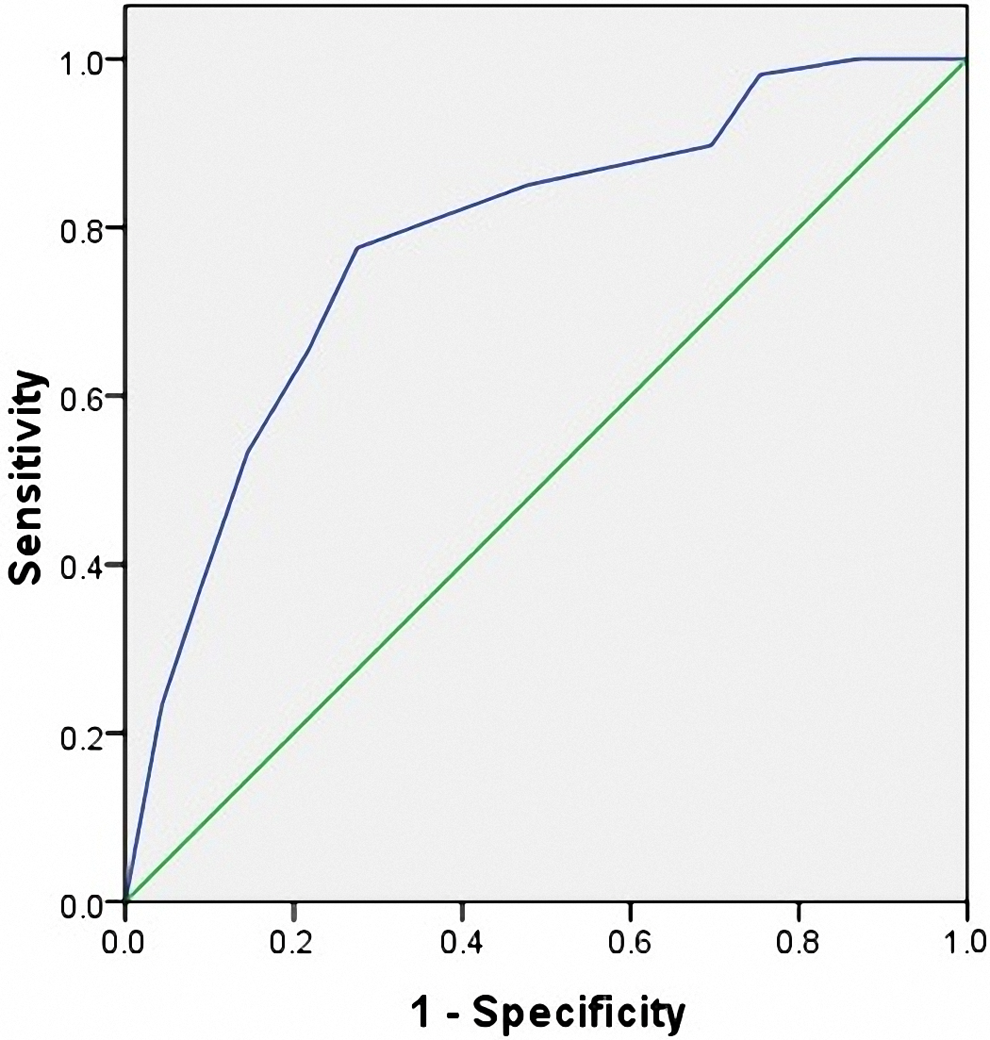
Receiver–operating characteristic (ROC) curves for red cell distribution width (RDW) value in prediction of impaired coronary collateral circulation (CCC).
Discussion
Our study results demonstrated that high RDW, high CK-MB, and absence of preinfarction angina were found to be independent predictors of impaired CCC.
Coronary collateral vessels are structures that are normally present in the human heart, though being invisible by angiography. However, when coronary stenosis develops, these normally invisible collaterals gradually become angiographically visible. The CCC development occurs as a result of angiogenesis (new vessel formation) and/or arteriogenesis (growth of preexisting arterioles). 15 Many factors may take part in the development of CCC such as severity and rate of progression of coronary stenosis, DM, HTN, smoking status, endothelial dysfunction, exercise, endogenous mediators, oxidative stress, and drugs used. 1 The CCC development in acute coronary syndromes has been found to be associated with better myocardial perfusion and ventricular functions as well as lower incidence of adverse cardiovascular events in the long term. 16 –18
In CCC development, many endogenous mediators such as growth factors, vascular endothelial growth factor (VEGF), nitric oxide (NO), inflammatory markers, and neurohumoral markers are involved along with endothelial dysfunction. 15 The RDW is a marker of variation in size of circulating red cells and is routinely reported by red blood cell analyzers as a part of routine CBC. Many studies have shown that RDW is an independent predictor of adverse events in the long term in both stable and acute coronary syndromes and that it is associated with impaired epicardial and myocardial perfusion after PCI in cases of acute coronary syndromes. 7,19 However, to date no study has been performed on the relationship between RDW and development of CCC in patients with CAD. In the present study, we demonstrated that raised RDW level was an independent predictor of impaired CCC. The mechanistic relationship between RDW and CCC can be explained by 3 proposed mechanisms. First, elevated RDW levels may inhibit the development of CCC. Raised RDW levels are associated with high erythropoietin, 20 B-type natriuretic peptide (BNP), 21 and tumor necrosis factor α (TNF-α) 22 levels. Furthermore, independent of RDW, these factors are also at raised levels in acute coronary syndrome as well. Pedram et al showed that natriuretic peptides inhibited angiogenesis. 23 Erythropoietin and TNF-α modulate erythropoiesis as well. Second, the developmental process of CCC may end up with increased RDW. Some endogenous factors that are increased throughout the development of CCC may alter RDW levels by affecting erythropoiesis. Several important angiogenesis modulators such as VEGF, fibroblast growth factor (FGF), and platelet-derived growth factor can also further activate erythropoiesis by increasing erythropoietin synthesis. 24 –26 Third, other than causal relationship, the process modulating the development of CCC may also have an impact on the RDW levels. For instance, endothelial dysfunction is important in terms of CCC development; however, it is known to be associated with RDW levels 27 as well. Furthermore, in the present study, we also found a relationship between CCC and preinfarction angina. It is known that well-developed CCC was observed in the presence of preinfarction angina. 1
In conclusion, whether it is the cause or the result, it is a fact that RDW levels are associated with impaired development of CCC in patients with NSTEMI. This suggests that clinically determining the RDW levels, which requires only a simple and cheap test, can be helpful in the detection of high-risk patients.
Limitation
Relatively small sample size is one of the major limitations of our study. The cross-sectional design of our study makes it difficult to comment on the causal relationship of RDW and impaired CCC. Finally, one of the most important limitations was the failure to measure some parameters such as FGF, VEGF, NO, erythropoietin, TNF-α, and BNP that could be helpful in evaluating the relationship between RDW and impaired CCC in detail.
Conclusion
In conclusion, we demonstrated that higher RDW value was associated with impaired CCC in patients with NSTEMI. We need further studies to investigate the cause and effect relationship between RDW and CCC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.