
Abstract
Elevated red blood cell distribution width (RDW) has been associated with adverse outcomes of heart failure and pulmonary hypertension. A total of 702 consecutive patients with acute pulmonary embolism (PE) were evaluated. There was a graded increase in mortality rate with RDW quartiles of 5.8% in quartile I (≤13.6), 9.7% in quartile II (13.7%-14.5%), 13.1% in quartile III (14.6%-16.3%), and 20% in quartile IV (>16.3%; P < .001). Patients who died had higher baseline RDW values (16.1% [11.7-28.3] vs 14.5% [10.7-32.5]; P < .001). The optimal cutoff value of RDW for predicting in-hospital mortality was ≥15%. The area under the curve of mortality for RDW was 0.649 (confidence interval [CI]: 0.584-0.715); the negative predictive value was 93%. In multivariable regression analysis, RDW remained associated with an increased odds of death (odds ratio: 1.2, 95% CI: 1.1-1.4). High RDW level was an independent predictor of short-term mortality in PE. The RDW levels may provide a potential marker to predict outcome in patients with PE.
Introduction
Red blood cell distribution width (RDW) is a quantitative measurement of the variability in size of circulating red blood cells. Recently, a strong association between elevations in RDW and adverse outcomes has been demonstrated in patients with chronic heart failure (HF), pulmonary hypertension, myocardial infarction, and also for patients in intensive care units. Inflammation has been proposed as a possible mechanism for the association of the elevated RDW in these patients. 1 –5 Also, an elevated RDW may be related to anemia, nutritional deficiencies, hemodilution, and abnormalities of the erythropoietin response. 6 However, the pathophysiology underlying the association between RDW and outcomes of cardiovascular diseases remains unclear.
Some studies have found that inflammation, as reflected by increased blood levels of C-reactive protein (CRP), is associated with increased risk of atherothrombosis. 7,8 Inflammation may also play a role in venous thromboembolism (VTE), a common thrombotic vascular condition. 9 Recently, several studies have established a relationship between inflammation and VTE. 10 –12 For example, Folsom et al suggest that elevated CRP is independently associated with increased risk of VTE. 10 The RDW has also been proposed to have some association with inflammation through the CRP and other inflammatory markers. 13
We speculated that a higher RDW would be independently associated with poor clinical outcomes in patients with pulmonary embolism (PE). We therefore investigated the prognostic value of RDW in patients with PE.
Materials and Methods
Study Design
The study retrospectively enrolled 725 consecutive patients who were diagnosed with acute PE between October 2003 and September 2009. The study was approved by the local ethical committee. The study was conducted at a university hospital, a tertiary care hospital that serves as a primary referral center for patients with suspected PE.
Patients and Setting
The patient demographic characteristics, clinical, and laboratory parameters were abstracted from the our hospital electronic database. The study consisted of consecutive patients with PE who were admitted with suspicion of PE and were diagnosed using computerized tomography pulmonary angiography (CTPA), a lung scan and/or clinical diagnosis. 14 Patients ≥18 years who were discharged with a primary diagnosis of PE were included in the study. The primary end point was all-cause inhospital mortality. Patients with shock or hypotensive PE (massive high risk) were defined according to the European Society of Cardiology as those with a systolic blood pressure of 90 mm Hg or a pressure drop of ≥40 mm Hg over 15 minutes if not caused by new onset arrhythmia. 14 For calculation of the simplified pulmonary embolism severity index (sPESI), 1 point was given for the presence of each one of the following variables: (1) age >80 years; (2) history of cancer; (3) history of chronic cardiopulmonary disease (HF or pulmonary disease); (4) heart rate ≥110 beats/min (bpm); (5) systolic blood pressure 90 to 100 mm Hg; and (6) arterial oxyhemoglobin saturation <90% measured at the time of PE diagnosis. Missing data were considered to be normal reference. 15,16 Patients were classified into either a low-risk (0 points) or a high-risk (≥1 point[s]) group reference. 16
Biochemical Analysis
We used hemograms obtained at the time of patient presentation for our analysis. Baseline RDW was measured using a Beckman Coulter Automated CBC Analyzer (Beckman Coulter, Inc, Fullerton, Miami). The normal reference value for RDW in the laboratory of our hospital is between 11.6% and 16.5%. According to the definition of the World Health Organization, we defined anemia as a hemoglobin (Hb) level <13 g/dL for men and <12 g/dL for women.
Troponin T (Tn-T) was determined by a quantitative electrochemiluminescence assay (Elecsys 2010; Roche, Mannheim, Germany, normal value <0.010 ng/mL) on admission.
Statistical Analysis
The Kolmogorov-Smirnov test was used to test for a normal distribution of continuous variables. Data characterized by a normal distribution were expressed as mean and standard deviation. Parameters without such a distribution were expressed as a median with range. Student test (normal distribution) or Mann-Whitney (nonnormal distribution) test was used for comparing the 2 groups. The Kruskal-Wallis (nonnormal distribution) test was used for comparing more than 2 groups. Discrete variables were compared using the Fisher exact test (chi-square test). The Spearman test was used to assess the correlation between variables. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated according to standard formulae. The investigation for a prognostic cutoff value is based on receiver–operating characteristic (ROC) curves.
Multivariate logistic regression analysis (by excluding hypotensive patients) was used as a stepwise descending method from prognostic factors with a P value significance of <.1 in the univariate analysis. P values <.05 were considered statistically significant.
Results
Seven hundred and twenty-five consecutive patients with acute PE were initially included in this study. Twenty-three patients were subsequently excluded due to their insufficient data from hospital records and the study enrolled 702 patients with acute PE. Computerized tomography pulmonary angiography was used most frequently to confirm acute PE (n = 657, 93.6%), followed by lung scans (n = 27, 3.8%) and clinical diagnosis (n = 18, 2.6%). Of all, 97.4% of the patients with PE had confirmation of PE through either CTPA and lung scan, which was shown as having better performance than using clinical criteria alone in the diagnosis of PE previously. 17 There was no statistically significant difference between the patients with PE diagnosed clinically and the patients with PE diagnosed radiologically (CTPA or lung scan) from the point of RDW values (14.6, 10.7-32.5) in clinically diagnosed patients with PE vs 13.7; 12-17.8 in radiologically diagnosed patients with PE; P = .75).
The median age was 68 (range: 20-95) years and 458 members of the study group (65%) were females.
The risk factors for PE include immobility (14%), surgery (26%), cancer (13%), previous VTE (11%), and other causes (19%). In all, 17% of patients were classified as having idiopathic PE. On admission, 72 (10%) had a massive embolism and 317 (42.7%) patients had deep vein thrombosis.
Overall, 346 (48.3%) patients had anemia (ie, Hb level <13 g/dL in men and <12 g/dL in women). The median serum Tn-T concentration was 0.018 ng/mL (range: 0.01-1.1) at admission; 255 (56%) of 452 patients had elevated serum Tn-T on admission. The median hospital stay was 10 (0-43) days.
Overall, 364 (52%) patients had high sPESI score. The RDW values were higher in patients with higher sPESI score than the patients with lower sPESI score (15.1%; 10.7-28.3) vs 14.3%; 11.7-32.5, P < .001).
Comparison of Baseline Patient Characteristics by RDW Level
The median RDW level was 14.6% (range: 11-33) at admission. We divided the patients into 2 RDW groups (low and high) according to the cutoff value for predicting PE mortality (listed in Table 1).
Baseline Patients Characteristics According to Baseline RDW Level.a
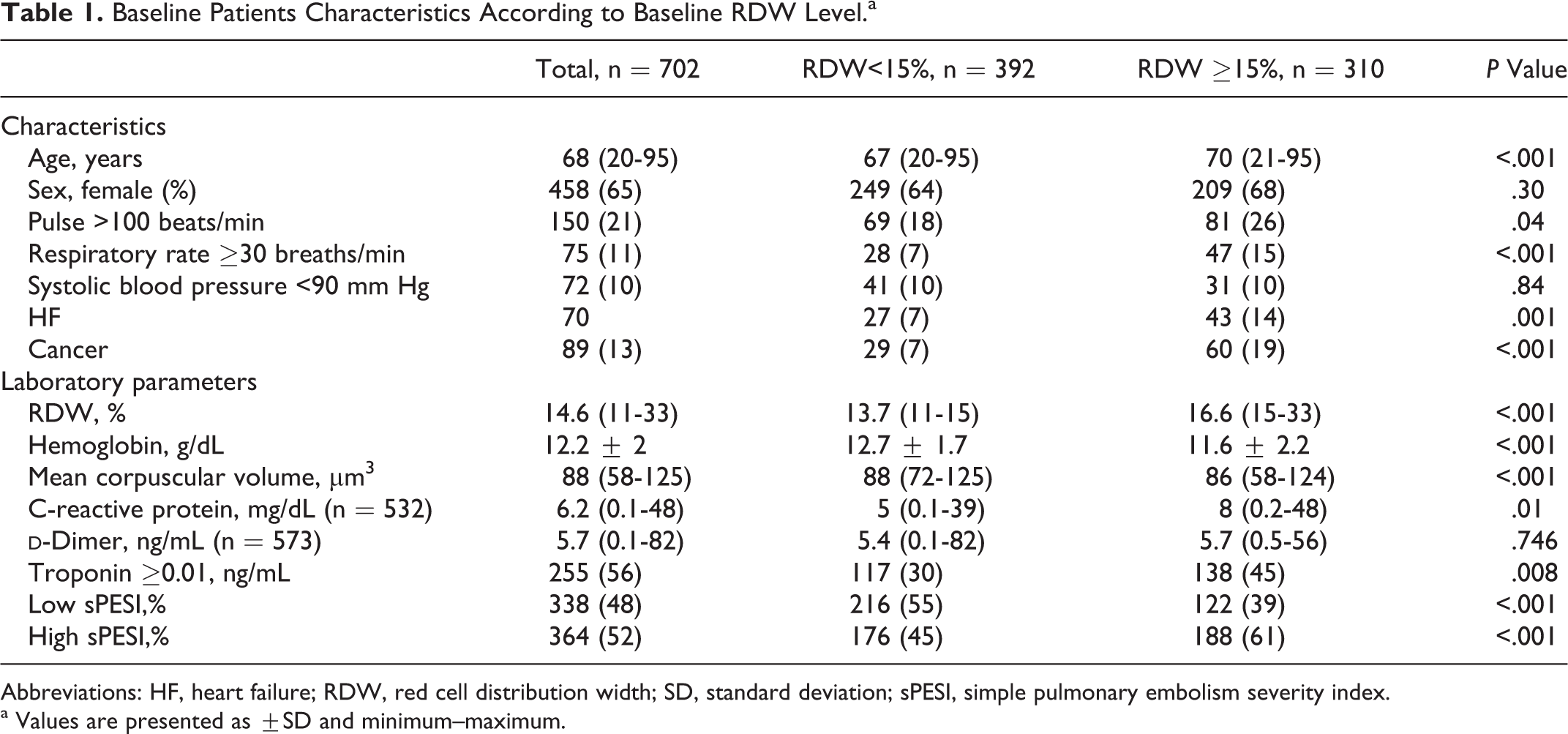
Abbreviations: HF, heart failure; RDW, red cell distribution width; SD, standard deviation; sPESI, simple pulmonary embolism severity index.
a Values are presented as ±SD and minimum–maximum.
The patients with elevated Tn-T level (≥0.01 ng/mL) had higher median RDW levels than the patients with lower Tn-T level (<0.01 ng/mL; 15.2; 12.1%-26.6% vs 14.5; 11.9%-32.5%; P = .006). Elevated Tn-T ≥.01 levels were more frequently seen in patients with RDW levels ≥15 than in patients with RDW levels <15 and this was statistically significant (45% vs 30%, P = .008).
There was no significant difference between RDW levels (high or low or RDW quartiles) in relation to the length of the stay in hospital.
Correlations of RDW
There was significant positive correlation between RDW and age (r = .16, P < .001), CRP (r = .10, P = .041), and elevated Tn-T (r = −.13, P = .006). The RDW was negatively correlated with Hb (r = −.34, P < .001) and with mean corpuscular volume (MCV; r = −.26, P < .001).
Mortality
Overall, inhospital mortality was 85 (12%). Patients who died had higher baseline RDW values (16.1%; 11.7-28.3 vs 14.5%; 10.7-32.5; P < .001; Figure 1).
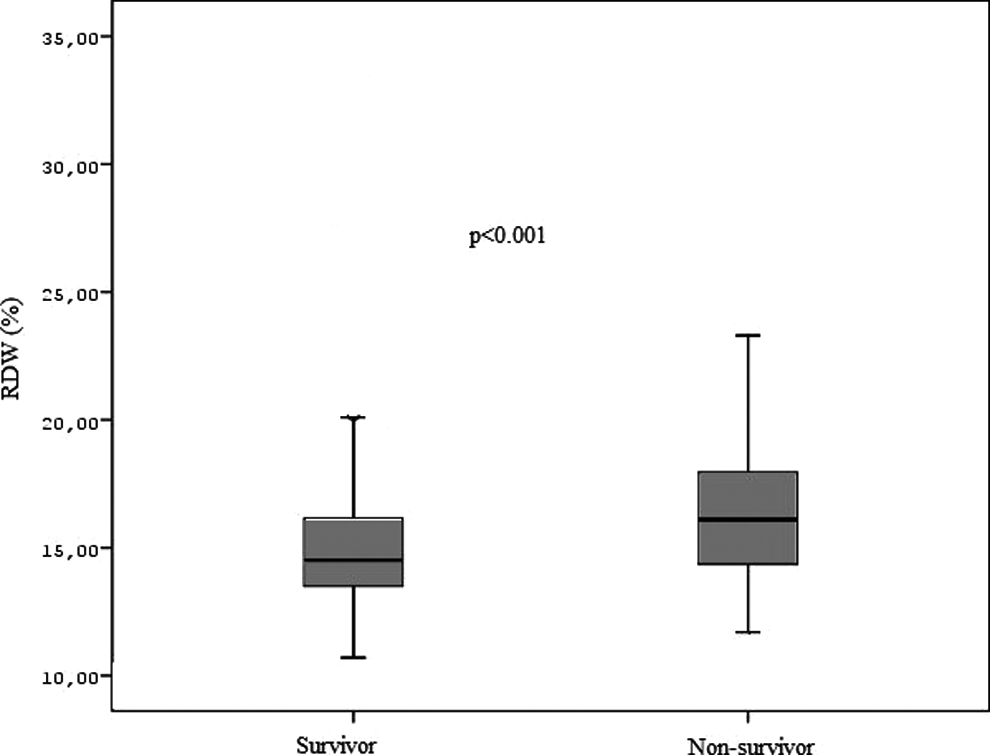
Box plot showing red blood cell distribution width (RDW) levels among patients with pulmonary embolism ([PE]; survivors vs nonsurvivors).
The ROC analysis was used to identify the optimal RDW cutoff value for all deaths (Figure 2). In the ROC analysis, the area under the curve was 0.649 (confidence interval [CI]: 0.584-0.715) of RDW levels for all-cause mortality. Serum RDW ≥15% showed sensitivity and specificity for all-cause deaths of 66% (95% CI = 55%-76% and 59%; 95% CI: 55%-63%), respectively. Also, serum RDW levels ≥15% showed high negative predictive value of (93%; 95% CI: 90-95) for all-cause deaths.
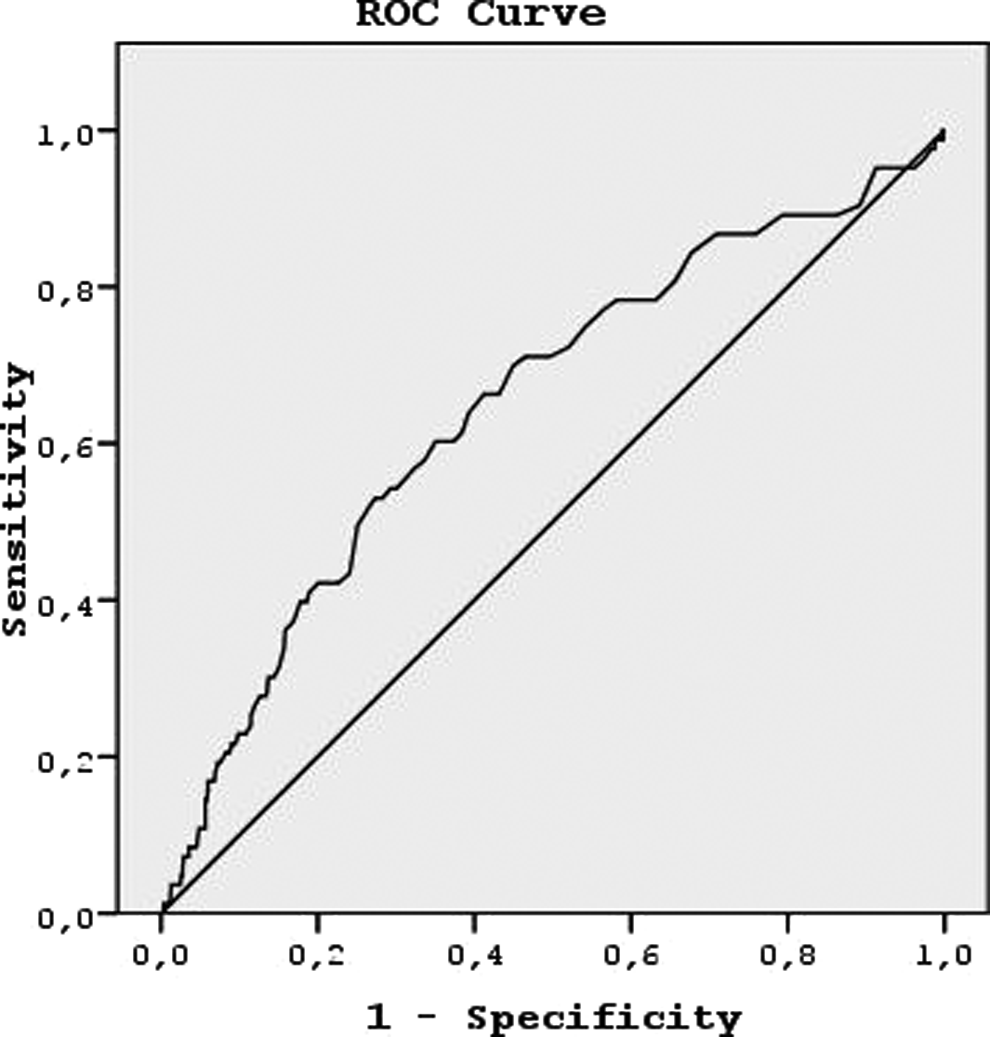
Receiver–operating characteristic curve of ability of red blood cell distribution width (RDW) to predict overall mortality (details are seen in the text).
There was also a graded increase in mortality rate with each RDW quartiles: 5.8% in quartile I (≤13.6), 9.7% in quartile II (13.7%-14.5%), 13.1% in quartile III (14.6%-16.3%), and 20% in quartile IV (>16.3%; P < .001 between groups 1 and 3; groups 2 and 4; and groups 1 and 4; Figure 3).
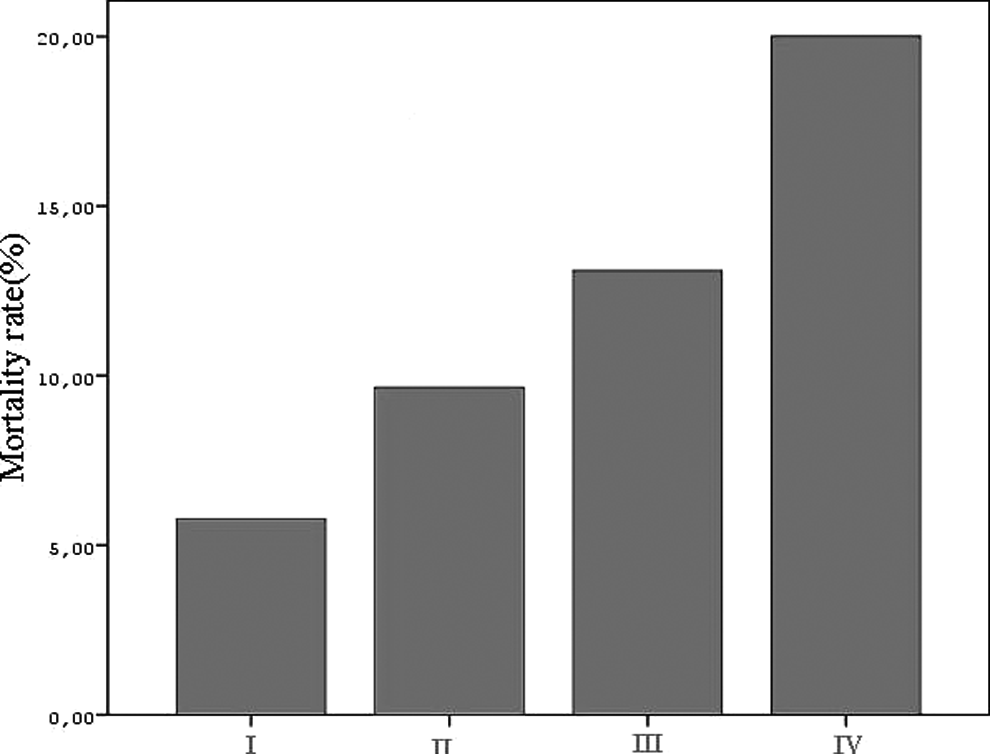
Pulmonary embolism (PE) mortality rate in patients with different red blood cell width quartiles. P < .001 for comparison of groups 1 and 2, groups 2 and 4, and groups 1 and 4.
The cumulative in-hospital mortality was not significantly higher among patients with anemia than in patients without anemia (11.2% vs 13%, P = .4). Median Hb levels were not higher among the patients who survived than for those who died (12.5 vs 12.4; P = .67). Median MCV levels were higher among the patients who died than those who survived (89 vs 87.5; P = .012).
Mortality predictors for univariate analysis included demographics (sex), clinical (respiratory rate breaths/min, sPESI [history of cancer, chronic lung disease, and HF, systolic arterial blood pressure <100 mm Hg, pulse ≥110 beats/min, and arterial oxygen saturation <90%]), and laboratory variables (CRP,
Hemoglobin, MCV, and
Predictors of PE Mortality by Univariate Logistic Regression (n = 630).a
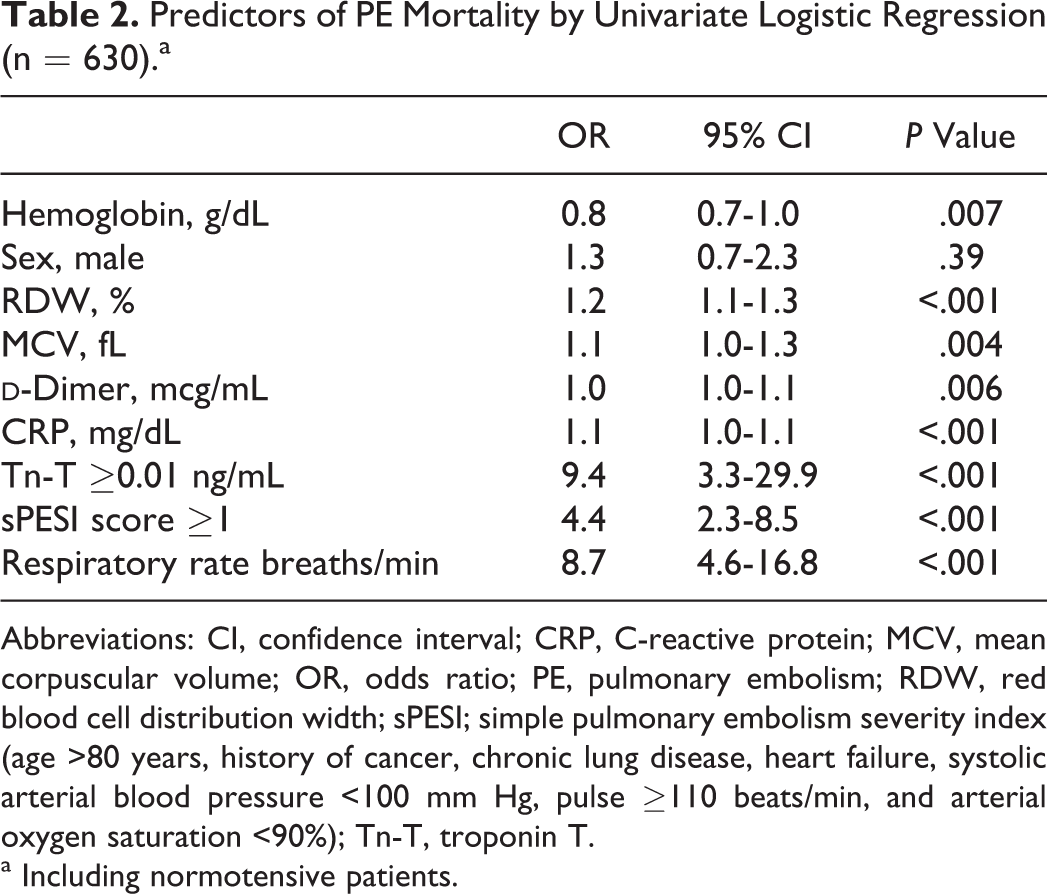
Abbreviations: CI, confidence interval; CRP, C-reactive protein; MCV, mean corpuscular volume; OR, odds ratio; PE, pulmonary embolism; RDW, red blood cell distribution width; sPESI; simple pulmonary embolism severity index (age >80 years, history of cancer, chronic lung disease, heart failure, systolic arterial blood pressure <100 mm Hg, pulse ≥110 beats/min, and arterial oxygen saturation <90%); Tn-T, troponin T.
a Including normotensive patients.
Independent Predictors of PE Mortality by Multivarite Logistic Regression Analysis (n = 630).a
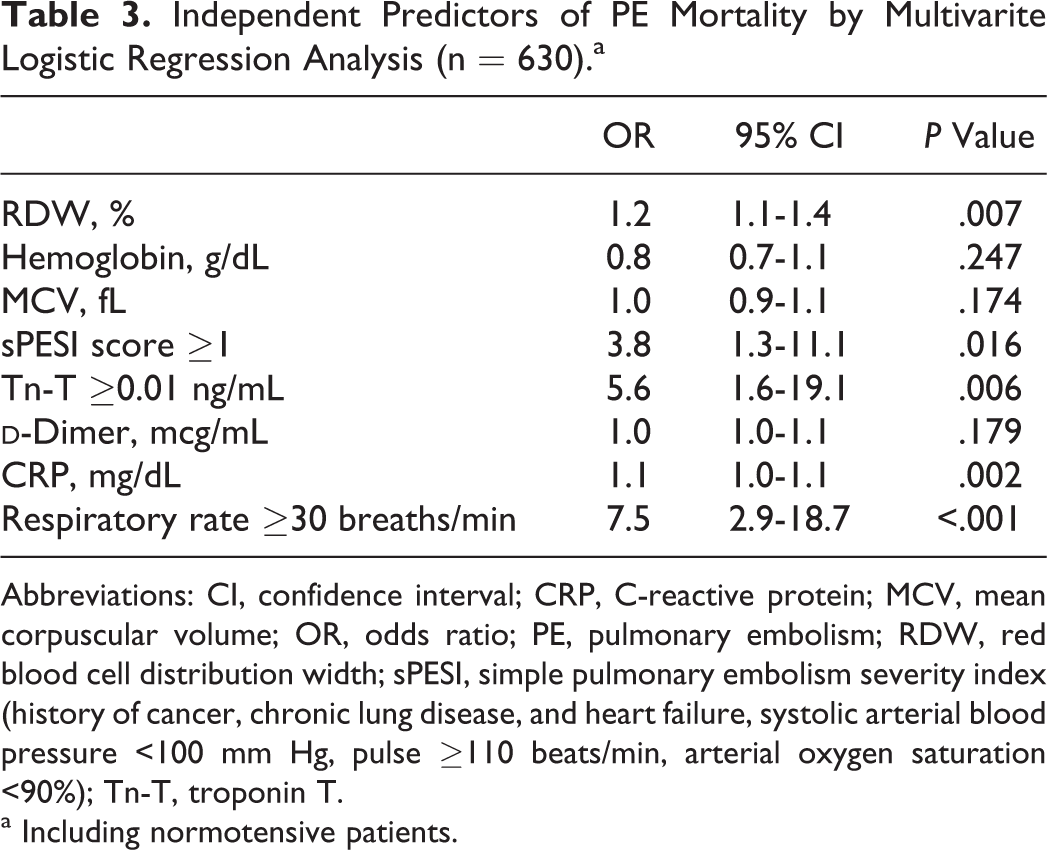
Abbreviations: CI, confidence interval; CRP, C-reactive protein; MCV, mean corpuscular volume; OR, odds ratio; PE, pulmonary embolism; RDW, red blood cell distribution width; sPESI, simple pulmonary embolism severity index (history of cancer, chronic lung disease, and heart failure, systolic arterial blood pressure <100 mm Hg, pulse ≥110 beats/min, arterial oxygen saturation <90%); Tn-T, troponin T.
a Including normotensive patients.
The cutoff value of RDW obtained by Kaplan-Meier survival analysis defined by ROC analysis showed a significant survival difference for all-cause mortality (P < .001; Figure 4).
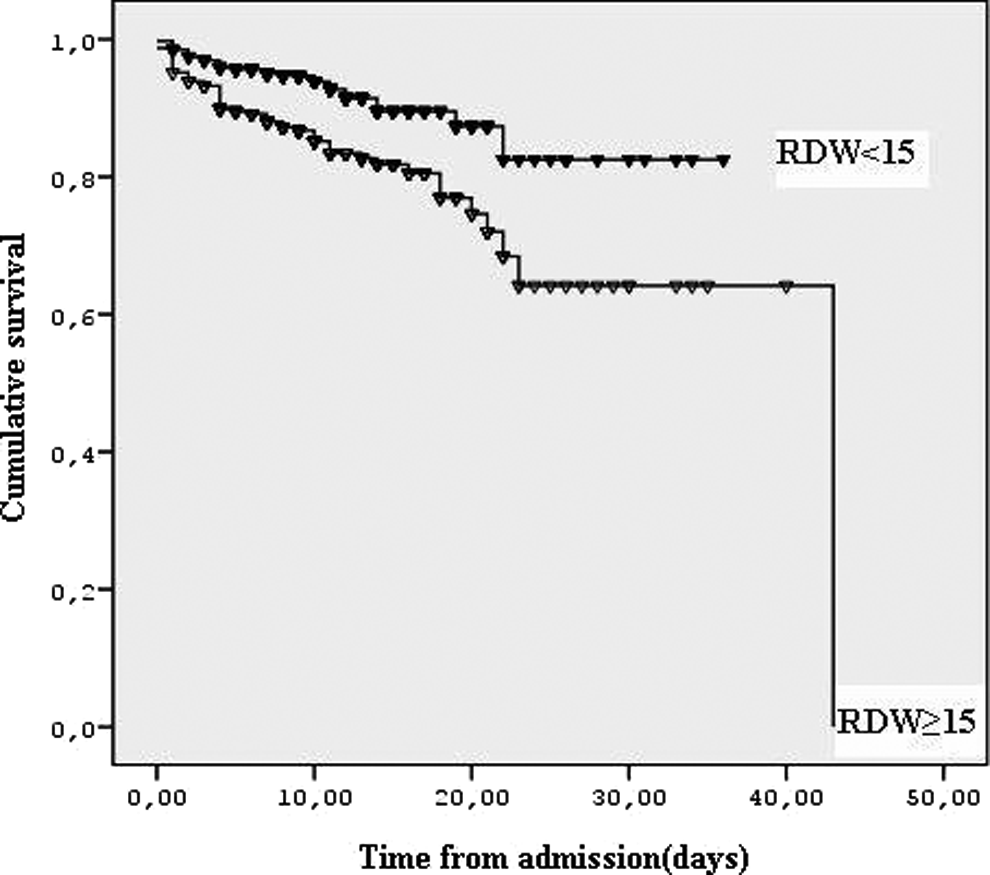
Kaplan-Meier estimates of in-hospital mortality for patients with pulmonary embolism according to the cutoff values of red blood cell distribution width (RDW).
Sensitivity and negative predictive value of high sPESI were 81% and 95%, respectively. Specificity and positive predictive value of high sPESI were 52% and 19%, respectively.
Discussion
The present study is a clinical determination of the prognostic value of RDW in patients with PE. The main finding of this study is that increasing RDW levels may potentially serve as an acceptable independent predictor of greater mortality in patients with PE.
In the present study, RDW remained a good predictor of mortality adjusting for hemoglobin concentration and others parameters. A current study has shown that patients with PE with anemia had higher mortality levels than patients with PE having normal hemoglobin levels. 18 However, in a meta-analysis, 19 RDW has been shown to be more strongly associated with mortality in nonanemic than in anemic older adults. In the present study, there was no significant difference between patients with anemia and patients without anemia in PE mortality. Pulmonary embolism is an acute disease process, therefore hemoglobin levels cannot be the direct cause of PE mortality. However, the higher mortality risk among anemic patients may be associated with increased risk of bleeding. In addition, hemoglobin levels are mostly associated with underlying disease in PE. Therefore, it may be said that the mortality of PE is actually related to the these associated comorbidity rather than to the hemoglobin level. Contrary to Hb levels, we found a significant association between RDW and in-hospital mortality. These results support the hypothesis that there would be several potential factors affecting the RDW level apart from the anemia.
Although the role of inflammation in PE remains unclear, a meta-analysis has shown that markers of inflammation such as interleukin 6 (IL-6), IL-8, and monocyte chemotactic protein were involved in the pathogenesis of VTE. 11 There was also a significant association between CRP and right ventricular dysfuntion in patients with PE. 20 Interestingly, the JUPITER study, a randomized trial, recently showed that statins lower the risk of VTE. 21 Actually, it was reported in this study that this risk-lowering effect of statin treatment in patients with PE is not only related to its anticoagulant effect but also related to its antiinflammatory effect. In a previous study, it was found that there was a significant correlation between inflammatory cytokines (eg, IL-6) and RDW in idiopathic pulmonary hypertension. 5 In the study significant correlations was found between CRP and RDW in patients with PE. Therefore, our data suggest the hypothesis that high RDW levels may reflect a variety of pathologic processes, such as inflammatory stress and may be potentially attributed to the poor outcomes in patients with PE.
The present study showed 364 (52%) patients with PE had high sPESI score. The RDW values were higher in those patients with higher sPESI score than the patients with lower sPESI score that was statistically significant. Venetz et al found that negative predictive value of sPESI score was 97%. 22 The present study showed negative predictive value of RDW as 93%. However, sPESI score is composed of multiple parameters including age >80 years, history of cancer, history of chronic cardiopulmonary disease (HF or pulmonary disease), heart rate ≥110 bpm, systolic blood pressure 90 to 100 mm Hg, and arterial oxyhemoglobin saturation <90% measured at the time of PE diagnosis. Variability of even 1 parameter (eg, age >80) may lead these patients with PE being grouped as high risk. On the other hand, RDW is simple, easily applied and single parameter that was found to have similar performance with sPESI score in the present study.
Similarly, serum levels of RDW ≥15 % show high negative predictive values for all-causes of death (93%) in our study. The present study also showed that RDW level was higher in patients elevated with Tn-T, which is known as a good predictor of mortality in patients with PE. On the other hand, patients with high RDW levels carry the highest risk of mortality. Therefore, it is suggested that low RDW levels can be used for favorable clinical outcome. Given the widespread availability and cost-effectiveness of RDW in comparison with that of the natriuretic peptides, RDW may represent a valuable alternative marker for risk stratification in patients with PE. However, these approach may be addressed by further studies.
When we look at the clinical implications of our findings for the future management of PE we find that, first, RDW is a routinely available test as a part of the automated blood count that is standard component of routine medical use. For example, on admission cardiac biomarkers may be used in patients with high RDW in PE. It would be a cost-effective approach. Second, high RDW levels in acute patients with PE may provide us with clinical awareness from the point of view of risk strafication of these patients with PE. It would be better to follow-up the RDW in patients who have high risk for PE.
There are several limitations to this study. Although this was a retrospective study, RDW is routinely measured as part of a full blood count on admission. We did not investigate the causes of elevated RDW, such as iron or vitamin B12 deficiency, which could confound the relationship between RDW and adverse outcomes. However, anemia did not predict all-cause mortality in our study. Another limitation is that the long-term outcomes of the patients discharged from hospital are unknown. In addition, when interpreting our results one should also consider that no autopsy was performed for defining pure PE-related deaths. Finally, because this study was not a prospective controlled design study, we do not have all the echocardiographic paramaters for right ventricular dysfunction for a comparison with RDW which may be important for future studies.
Finally, RDW is a newly recognized and an independent predictor of mortality in PE. Especially low RDW can be used for the prediction of good clinical course in patients with PE. The RDW may also become a promising parameter for risk stratification of PE, although RDW is not found superior to troponin. Considering that RDW is an inexpensive and simple test that is routinely reported to physicians, further prospective researches should determine whether RDW is a useful risk assessment tool in patients with PE.
Footnotes
Acknowledgment
The authors thank Prof RW Guillery from University of Oxford for language correction of the manuscript.
Authors’ Note
Dr Ozsu was involved in the conception, coordination, design, interpretation of the study and drafting, reading, analyzing the data, and approval of the manuscript. Dr Abul was involved with analyzing the data, drafting, and reading. Dr Gunaydin was involved with the data collection. Dr Orem contributed to biochemical analysis and interpretation, and Dr Ozlu was involved with coordination, design, and interpretation of the study and drafting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.