
Abstract
Aim:
We aimed to investigate the association between baseline red cell distribution width (RDW) level and the risk of stroke in patients with heart failure (HF).
Methods:
A total of 153 consecutive patients with HF (New York Heart Association [NYHA] I-III and left ventricular ejection fraction of <40%) were included in this prospective study. All the patients were followed up for 1 year, and during this period the cerebrovascular disease was questioned.
Results:
In matched population, using propensity score matching comparing patients with HF having stroke with patients without stroke, we found significantly increased basal RDW and serum uric acid. The receiver-operating characteristic curves of RDW for predicting stroke are performed. An RDW ≥15.2% measured on admission had 87% sensitivity and 74% specificity in predicting stroke in patients with HF (area under the curve: 0.923, 95% confidence interval: 0.852-0.994, P < .001).
Conclusion:
In conclusion, this study demonstrated that RDW may be important hematological indices for stroke in patients with HF using propensity score analysis.
Introduction
Heart failure (HF) is a complex clinical syndrome caused by structural or functional changes in the ventricles, which affect the ventricular filling and/or ejection. 1 The HF is associated with an increased risk of stroke even if in sinus rhythm, 2 and the identification of new eligible indices of stroke could provide new knowledge about the pathogenesis and prevent this complication in patients with HF.
Red cell distribution width (RDW) indicates the presence of erythrocytes with different sizes (anisocytosis). 3 The RDW increases in many cases such as ineffective erythropoiesis caused by hemolysis and iron deficiency anemia. Also, pregnancy and some hematological disorders (such as thrombotic thrombocytopenic purpura [TTP]) and inflammatory bowel disease (IBD) may cause increase in RDW. 4–6 Previously, RDW is an indicator that is used for the differential diagnosis of the anemia, later, it was shown that it has a prognostic value in acute and chronic cardiac events in healthy population,. 7–9
Although it was shown that increased basal RDW level is an index of hospitalization and mortality of patient with HF, the relationship between RDW and risk of stroke has not been investigated comprehensively. 10,11 Therefore, in this particular study, we aimed to investigate the association between the baseline RDW level and the risk of stroke in patients with HF.
Methods
Patient Selection
A total of 153 consecutive patients with HF (New York Heart Association [NYHA] I-III and left ventricular ejection fraction [LVEF] of <40%) who were admitted to outpatients clinics of our hospital were included in this prospective study between June and September 2011. Patients with anemia (n: 10), history of stroke (n: 3), end-stage renal disease (ESRD; n: 3), inflammatory disease (n: 2), menorrhagia (n: 1), and malignancy (n: 1) were excluded. Finally, 133 nonanemic patients with stable chronic HF were included in the study. All patients were followed up for 1 year and during this period it was questioned prospectively whether they have cerebrovascular disease. The local ethics committee approved this study.
Patients’ laboratory and clinical characteristics, such as age, sex, diabetes mellitus (DM), hypertension (HTN), hypercholesterolemia, smoking, family history of cardiovascular disease, height, and weight, were questioned. By dividing weight in kilograms by height in meters squared (kg/m2), the body mass index (BMI) was calculated. The rhythm status was determined in all the patients on admission using electrocardiogram. The reason for HF (ischemic or nonischemic) and drug use was questioned in all the patients. Hemoglobin (Hb), RDW, white blood cell count, and other hematological indices were measured as part of the automated complete blood count using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). The glomerular filtration rate (GFR) was estimated by the simplified Modification of Diet in Renal Disease Equation.
Transthoracic echocardiography was performed on patients before they were discharged using a system V (Vingmed, GE Horton, Norway) with a 2.5 MHz phased-array transducer. Recordings were taken on patients positioned in the left lateral decubitus position. The LVEF was measured using the modified Simpson rule. 12
Definitions
Anemia on admission was defined as a baseline Hb concentration less than 13 mg/dL in men and less than 12 mg/dL in women, in accordance with the World Health Organization criteria. 13 The diagnosis of DM was based on the previous history of diabetes with or without drug therapies. Hypercholesterolemia was defined as total cholesterol of ≥200 mg/dL. Obesity was defined as a BMI of ≥30 kg/m2. Current smokers were defined as those who had smoked for some period during the past year. Patients were considered as having ESRD, if they were dependent on chronic dialysis. Renal insufficiency was defined as a GFR of <60 mL/min/1.732 m2. 14
Statistics
Continuous variables are expressed as mean ± standard deviation. Categorical variables are expressed as percentages. To compare parametric continuous variables, the Student t test was used; the Mann-Whitney U was used to compare nonparametric continuous variables. To compare categorical variables, the chi-square test was used. The receiver–operating characteristics (ROC) curve was used to demonstrate the sensitivity and specificity of RDW and its respective optimal cutoff value for predicting stroke in patients with NYHA I to III HF.
As the study was nonrandomized, a propensity score was created with variables frequently used by the clinician when deciding the prediction of stroke for each patient (age, sex, diabetes, HTN, triglyceride [TG], high-density lipoprotein [HDL], low-density lipoprotein [LDL], LVEF, systolic pulmonary artery pressure (sPAP), glucose, and creatinine) to balance patient characteristics and to generate propensity-matched analysis for the 2 groups. The propensity score was developed using SPSS, version 20.0 for Windows and the R statistical package, version 2.12.1. Two-tailed P values <.05 were considered to indicate statistical significance.
Results
The RDW values of 133 patients enrolled in the study (mean age 65.9±10.9, %71.4 male) ranged from 11% to 24% (median 14.8%, mean 15.4% ± 2.2%). The baseline characteristics of the patients with and without stroke are summarized in Table 1. Patients with HF with and without stroke were comparable for age, sex, HF etiology, atrial fibrillation, LVEF, sPAP, cardiovascular risk factors, and medication. When patients with HF having stroke were compared with patients without stroke, we found significantly increased basal RDW creatinine, LDL, and decreased potassium levels in unmatched analysis. A propensity score was created with variables frequently used by the clinician when deciding the prediction of stroke for each patient (age, sex, diabetes, HTN, TG, HDL, LDL, LVEF, sPAP, glucose, and creatinine) to balance patient characteristics and to generate propensity-matched analysis for the 2 groups (Figure 1 and table 2). In matched population, when comparing patients with HF having strokewith patients without stroke, we found significantly increased basal RDW (16.9 ± 1.14 vs 14.8 ± 1.6, P < .001) and serum uric acid (8.8 ± 1.7 vs 7.5 ± 1.1, P = .027).
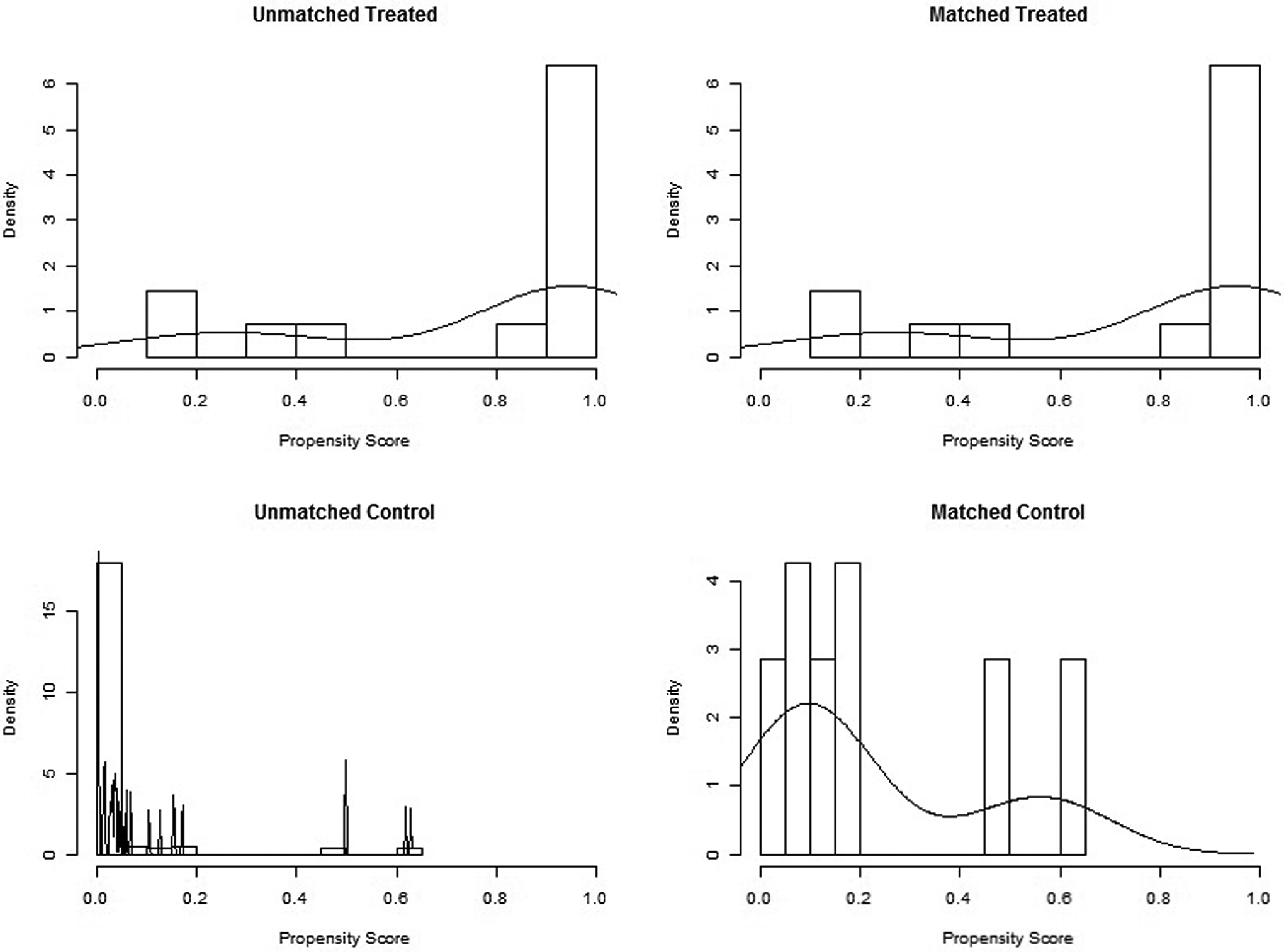
A propensity score histogram before and after matching.
The Baseline Characteristics of the Patients With and Without Stroke Before Propensity Matching.
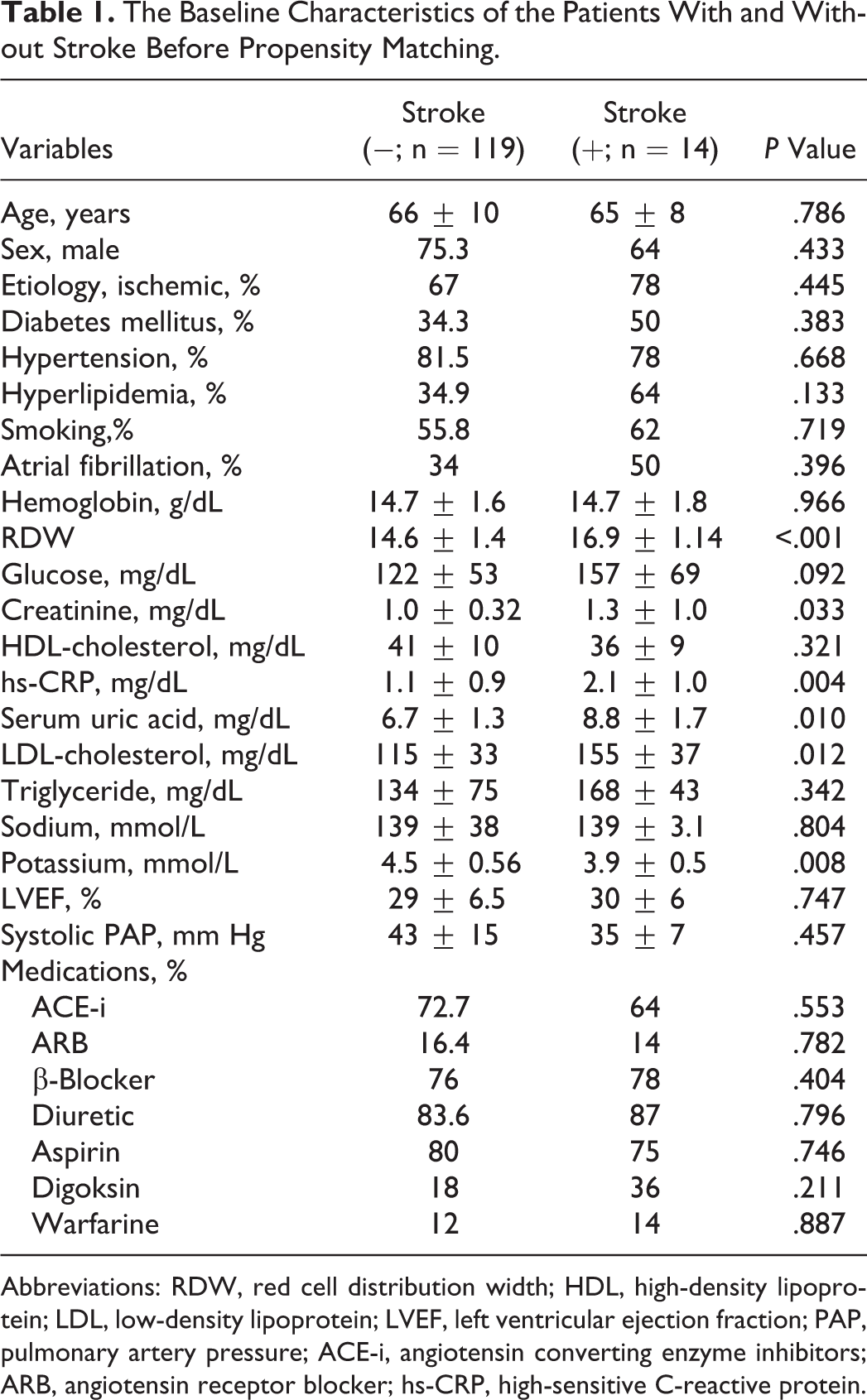
Abbreviations: RDW, red cell distribution width; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; PAP, pulmonary artery pressure; ACE-i, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blocker; hs-CRP, high-sensitive C-reactive protein.
The Baseline Characteristics of the Patients With and Without Stroke After Propensity Matching.
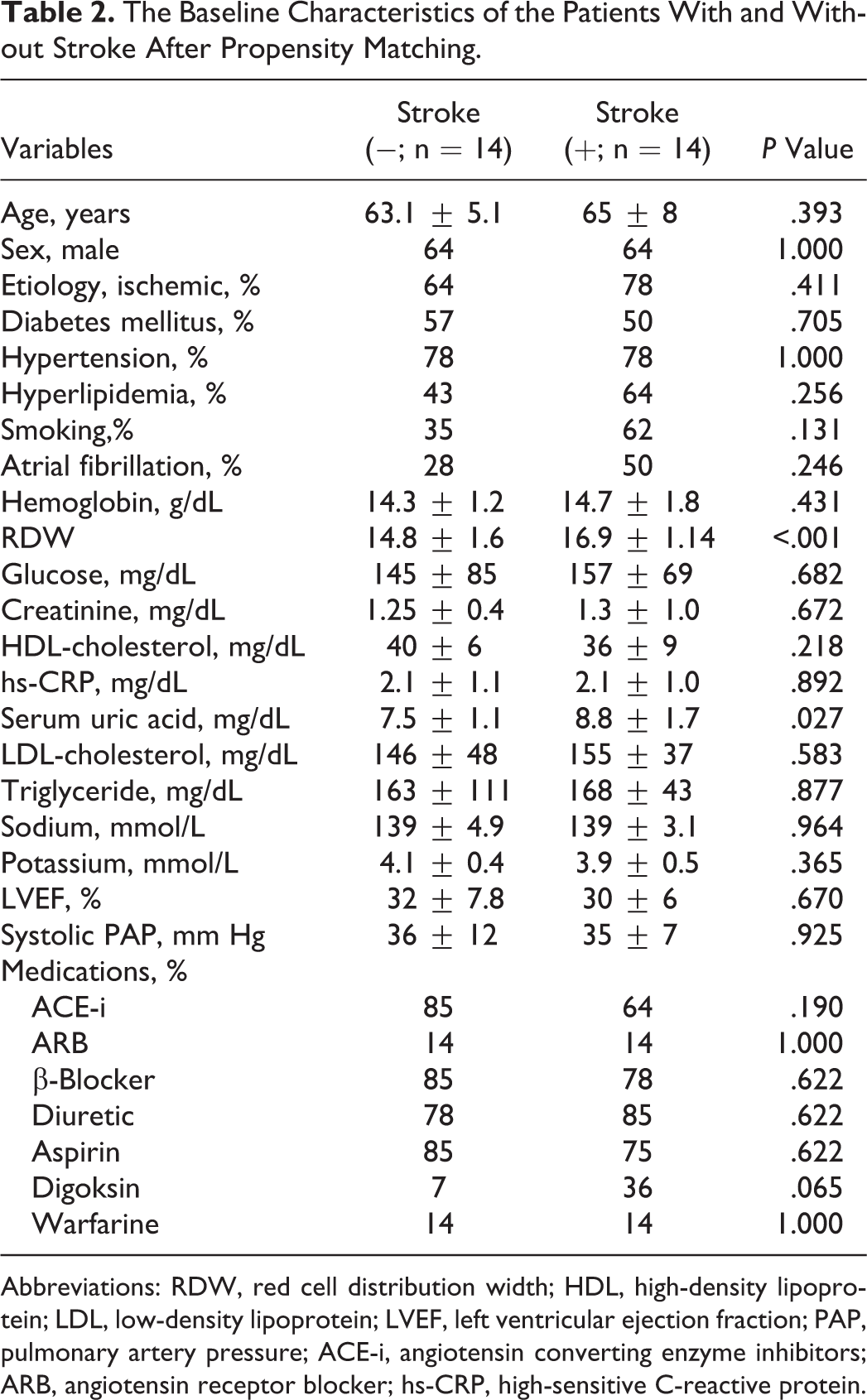
Abbreviations: RDW, red cell distribution width; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; PAP, pulmonary artery pressure; ACE-i, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blocker; hs-CRP, high-sensitive C-reactive protein.
The ROC curves of RDW for predicting stroke is shown in Figure 2. A RDW ≥15.2% measured on admission had 87% sensitivity and 74% specificity in predicting stroke in patients with HF (area under the curve: 0.923, 95% confidence interval: 0.852-0.994, P < .001). In addition, the analyses made in the whole study population showed that there is a significant correlation between RDW, high-sensitive C-reactive protein (r: .312, P: .006), and uric acid levels (r: .299, P: .010; Figure 3).
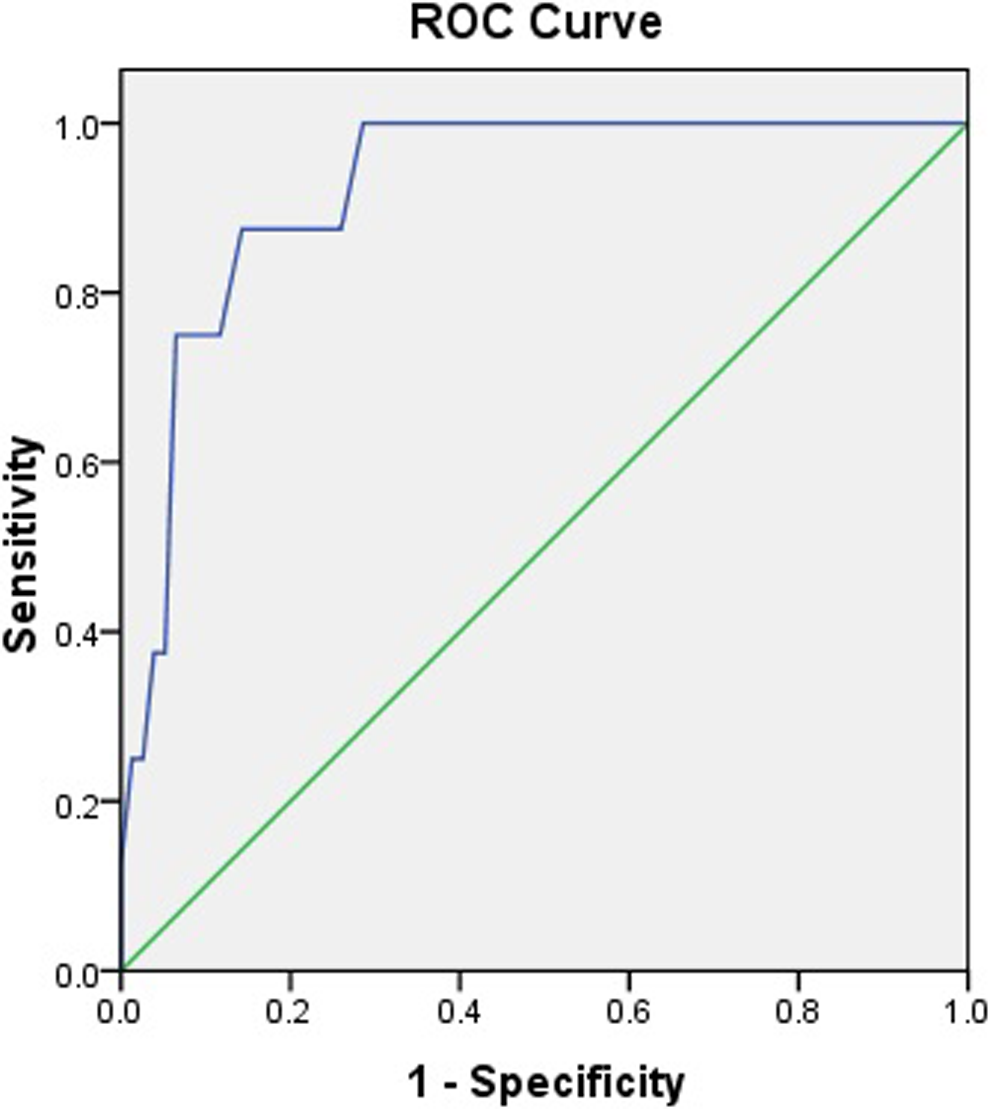
Receiver–operating characteristic curve analysis for red cell distribution width (RDW) value in prediction of stroke.
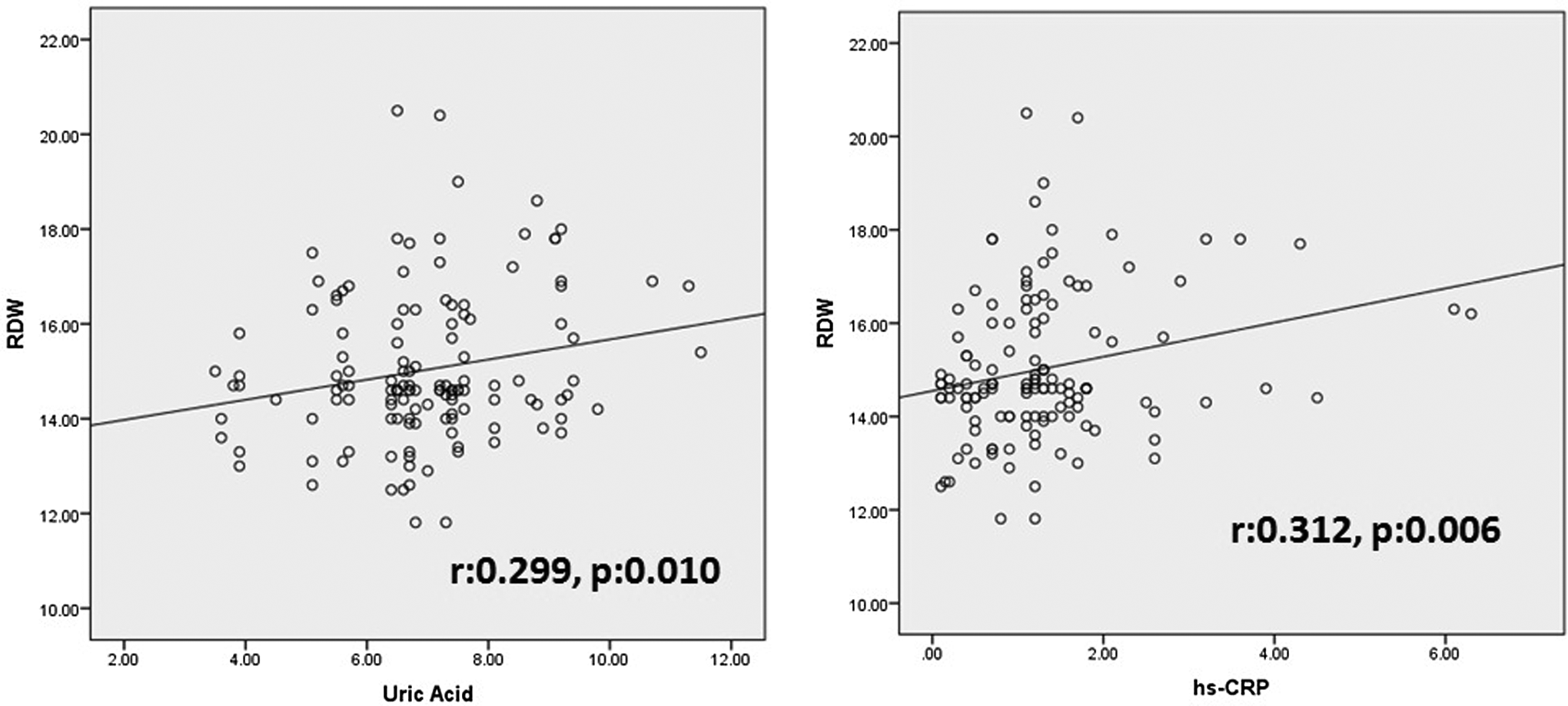
Relation of red cell distribution width (RDW) with uric acid and high-sensitive C-reactive protein (hs-CRP) in a scatter figures.
Throughout the study, all strokes (n = 14) were analyzed. Transient ischemic attack (2 cardioembolic and 1 significant carotid artery disease), cardioembolic stroke, significant carotid artery disease, and thromboembolic events of vertebra-basillary arterial system were detected in 3, 5, 3, and 2 patients, respectively. However, we could not find the exact etiology in 1 patient.
Discussion
In this study, for the first time in the literature, we evaluated the relationship between baseline RDW levels and the risk of stroke in patients with HF. The study results revealed that elevated basal levels of RDW in stable patients with HF are significantly associated with stroke, according to the propensity score analysis. The risk of stroke increased in the patients with HF regardless of atrial fibrillation. 2 Hospitalization in patients with chronic HF, stroke, and mortality risk is closely associated with increased oxidative stress, and these are shown in the previous studies. 15 Increased vascular oxidative stress and vascular endothelial dysfunction trigger the atherosclerosis responsible for the stroke. 16,17
The clinical usage of RDW is rare outside of differential diagnosis of anemia. Studies showed that RDW is predictive for HF development in healthy population and in patient that had MI, and it is also predictive for mortality in patients with HF. 10,11 The following studies showed that increased RDW levels are related to poor prognosis in acute myocardial infarction 8 and stable angina pectoris. 7 The relationship between RDW and stroke is controversial. Malandrino et al reported that higher RDW values are related to increased risk of stroke in diabetes. 18 Tonelli et al demonstrated that increased RDW levels were related to increased risk of stroke in patients with coronary artery disease who were free of HF. 7 Ani and Ovbiagele showed that elevated RDW was a predictor of cardiovascular and all-cause mortality in patients with history of stroke. Additionally, they reported RDW was higher in patients with stroke compared to patients without stroke. 19 In contrast, Ntaios et al revealed that RDW does not predict severity or functional outcome in patients with acute ischemic stroke. Additionally, they found that RDW was related to low ejection fraction. 20 Indeed, increased RAAS activation system was shown to be caused by increased erythropoiesis. 21 Height of RDW is thought to be closely related to the mortality in patients with HF and stroke, but there is no enough information about predictive value for stroke in patients with HF. With this study, we showed that increased RDW levels in stable patients with HF can be indices of stroke in 1-year follow-up.
Several mechanisms may be suggested for increased stroke risk in patients with HF with elevated RDW levels. But the most probable mechanism is oxidative stress. There is a relationship between uric acid levels and stroke risk as an indicator of increased oxidative stress. 22 Increased oxidative stress, by causing injury to the vessel wall (which is responsible for many strokes triggering atherosclerosis), is thought to have the tendency to develop stroke. 16 , 17 In our study, we found that uric acid was an independent predictor of stroke. There is a close relationship between elevated levels of RDW and reduced oxidative stress in the previous studies. 23 Similarly, we found that RDW was significantly correlated with uric acid level. The possible mechanism is increased RDW levels after increased oxidative stress. 24 , 25 Red blood cells have a strong antioxidant capacity so that they are exposed to oxidative stress and damage commonly. Therefore, it is more possible to be damaged by oxidative stress and immature blood cell participation to the circulation. More studies are needed to fully understand the pathophysiological mechanistic relationship between RDW and stroke. However, we thought that the oxidative stress, which is closely related to stroke development risk, affects the erythropoiesis, by increasing the level of RDW.
In conclusion, this study demonstrated that RDW may be an important hematological index for stroke in patients with HF. The use of anticoagulant therapy in patients with HF regardless of rhythm remains controversial. 2,26 This large-scale prospective, randomized studies in patients with HF and with a high RDW show the need for closer follow-up and/or preventive treatment against the risk of stroke development (such as the anticoagulants).
Limitations
First, being a single-center study and containing a relatively low number of patients may be a limitation. Second, we did not make distinction between hemorrhagic and ischemic stroke. Third, the RDW may increase in many clinical situations such as hemolysis, transfusion, and iron, vitamin B12, and folate deficiency, which cause ineffective erythropoiesis. In addition, clinical situations such as pregnancy, TTP, and IBD can result in increased RDW levels. In this study, only the Hb level was checked, and those of iron, vitamin B12, and folic acid were not. However, none of the patients in the study had the diagnosis of IBD or TTP, and also they were not pregnant or in malnutrition. Only stable patients were taken into the study, and they were followed up in terms of stroke prospectively. In our study, nonanalysis of oxidative stress indicators is seen to be a limitation, but in the previous studies those markers have been shown to be correlated with RDW.
Footnotes
Acknowledgment
The authors thank Dr Tanboga for performing Propensity score matching analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.