
Abstract
Immunological thrombocytopenias, as other forms of thrombocytopenia, are associated with bleeding. Occasionally, these patients manifest thrombotic events. A total of at least 29 patients were reported to have had either arterial (20 cases) or venous (9 cases) thrombosis while platelet count was less than 50 × 103/μL. The most frequent clinical manifestation was a myocardial infarction. Thrombosis occurred in the large majority of patients during prednisone therapy. Patients receiving cortisone or patients with Cushing syndrome show a hypercoagulable state characterized by elevated factor VIII levels, decreased fibrinolysis, and abnormal von Willebrand factor multimers composition. The same is probably true for prednisone-treated patients with thrombocytopenia. However, the 2 conditions are not identical since prednisone is a mainly glycoactive compound, whereas cortisol produced in excess in Cushing syndrome is mainly mineraloactive. The presence of large, young, hyperactive platelets may also play a role. Prednisone-treated patients with thrombocytopenia have to be considered as potentially thrombophilic.
Introduction
Thromboses represent a major health problem in the Western world. They are usually associated with hypertension, old age, diabetes, dyslipidemia, smoking, myeloprolipherative disease, coagulation inhibitors defects, trauma, pregnancy, surgery, oral contraceptives, and immobilization.
The occurrence of arterial or venous thrombotic events in bleeding disorders is rare but it has been reported both in congenital and acquired conditions. In recent years, particular emphasis has been placed on the thrombotic, mainly arterial, events seen in middle aged patients with hemophilia. 1,2 The availability of adequate replacement therapy has radically changed the mean life expectancy of these patients. An unexpected side effect of this improvement in survival has been the appearance of atherosclerotic and thrombotic events. The same phenomenon was observed with rare clotting disorders, mainly factor VII (FVII) deficiency. 3
The occurrence of thrombotic events in patients with thrombocytopenia is a rare event. However, both congenital and acquired forms of thrombocytopenia have been occasionally associated with arterial and/or venous thrombosis. 4 –10
The purpose of the present study was to analyze critically all reported cases of thrombosis in patients with idiopathic or immunological thrombocytopenic purpura (ITP) in an attempt to clarify the role played in these patients by different potential prothrombotic mechanisms.
Patients and Methods
All articles dealing with the occurrence of thrombotic events in patients with ITP were examined. Personal files dealing with patients with ITP studied in Padua during the years 1980 to 2006 were also reevaluated.
Reports, regardless of the language, were retrieved by means of an unlimited time PubMed search using pertinent key words. Actual articles were then obtained with the help of Pinali Medical Library of our University and through the courtesy of Data Med, Sorengo, Switzerland. Cross-checking of the references listed by the single articles was carried out in order to exclude omissions.
Inclusion criteria were (1) established diagnosis of ITP; (2) platelet number at time of thrombosis below 50 × 103/μL; (3) lack of any other bleeding disorder, a normal PT and aPTT were considered a sine qua noncondition; (4) thrombosis occurring postsplenectomy or postintravenous immunoglobulin (IVIG) infusion was included, provided the platelet count at time of thrombosis was always below 50 × 103/μL; (5) the thrombotic events had to be demonstrated by objective means, namely a positive sonography and/or venography, pulmonary scintiscan or arteriography or spiral CAT for venous thromboembolism and positive cardiac enzymes, compatible electrocardiography and/or echocardiogram, consistent coronarographic or arteriographic results for arterial thrombosis. Exclusion criteria were (1) hereditary or familiar forms of thrombocytopenias and (2) thrombocytopenia due to leukemias, disseminated intravascular clotting DIC, lupus erythematosus systemicus LES, thrombotic thrombocytopenic purpura, hypersplenism, or antiphospholipid antibody syndrome.
The presence of congenital or acquired associated risk factors such as clotting prothrombotic defects, trauma, surgery, bone fractures, pregnancy, delivery, old age, hypertension, smoking, diabetes, dyslipidemia, obesity, bed immobilization, and oral contraception were all recorded.
The therapeutic regimen at the time of thrombosis and that followed by the patient during the last month previous to the thrombotic event was recorded.
The management of the thrombotic event and its evolution was also recorded. Acute coronary syndromes (unstable angina or non-ST elevation myocardial infarction [MI]) were also included in the MI series providing the patient had undergone cardiac invasive procedures. Those who were treated conservatively were excluded. Patients with simple angina were excluded even if they had undergone invasive procedures. The type of MI (anterior, anterolateral, posterior or inferior, and diffuse or massive) was recorded whenever possible.
Results
At least 20 patients (1 from personal files and 19 from the literature) with ITP were found to have had arterial thrombosis (15 MI, 2 unstable angina, 2 ischemic stroke, and 1 peripheral arteries thrombosis). 4,6,8,11 –27 Another patient, from personal files, had to be excluded because at time of thrombosis (MI), the platelet level was 100 × 103/μL. 28 Age varied between 37 and 80. Ten were male and 10 were female (Table 1).
Patients With Immune Thrombocytopenia and Arterial Thrombosis.
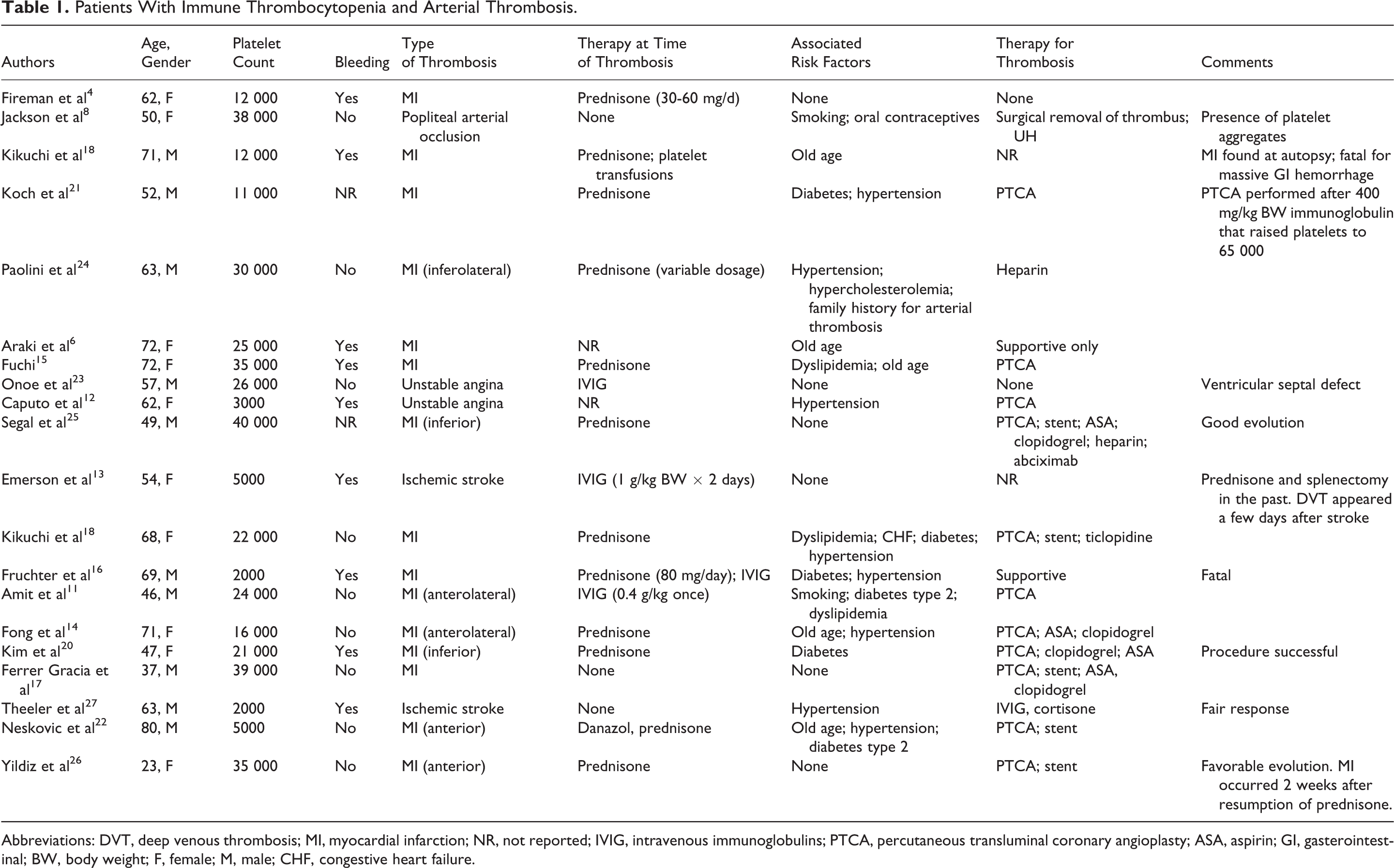
Abbreviations: DVT, deep venous thrombosis; MI, myocardial infarction; NR, not reported; IVIG, intravenous immunoglobulins; PTCA, percutaneous transluminal coronary angioplasty; ASA, aspirin; GI, gasterointestinal; BW, body weight; F, female; M, male; CHF, congestive heart failure.
At least 9 patients with ITP presented venous thrombosis, 4 deep venous thrombosis (DVT), 1 of which with pulmonary embolism; 1 jugular vein thrombosis and 4 patients cerebral sinuses thrombosis. Age varied between 12 and 83. Four were male and 4 were female. 5,7,9,29 –33 The total number of patients with ITP who presented a thrombotic event while platelets were less than 50 000/μL reached, therefore, the number of 29 (14 male and 15 female) with an age range of 12 to 83 (Table 2).
Venous Thrombosis in Patients With Immunological Thrombocytopenia.
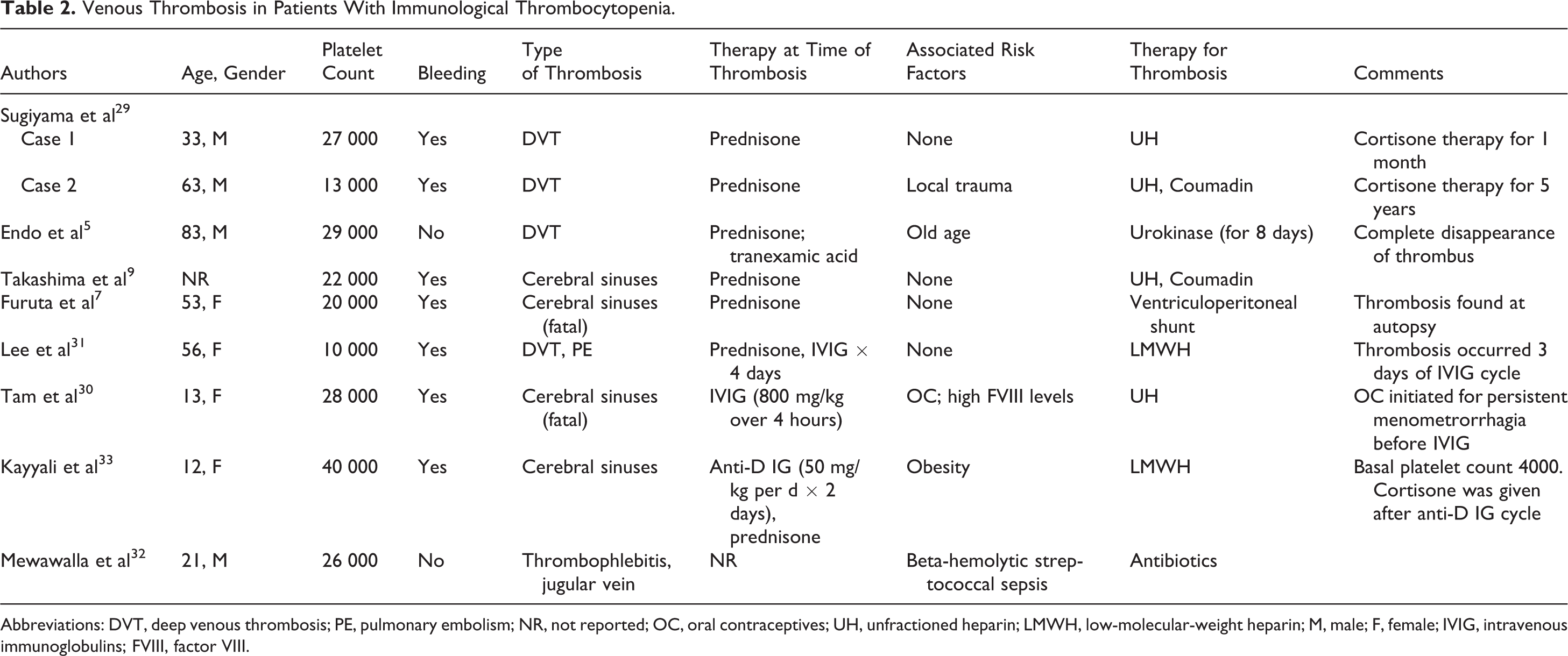
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism; NR, not reported; OC, oral contraceptives; UH, unfractioned heparin; LMWH, low-molecular-weight heparin; M, male; F, female; IVIG, intravenous immunoglobulins; FVIII, factor VIII.
Associated risk factors were present in 14 of the 20 patients with arterial thrombosis and in 5 of the 9 patients with venous thrombosis. The most frequent associated risk factors for arterial thrombosis were hypertension, dyslipidemia, smoking, and diabetes. Old age (>70 years) was also present in 4 cases. On the contrary, 4 patients with venous thrombosis had no classical risk factors (4 of 9). Trauma, old age, oral contraception, obesity, and sepsis were present in the remaining 5 patients.
Cortisone therapy, at variable dosage, was present at the time of thrombosis in almost all patients (19 of the 26 patients). Three patients were taking IVIGs, 1 patient was on danazol together with prednisone while 2 patients were taking no medication. In 3 instances, the therapy at time of thrombosis was not reported.
Discussion
Thrombotic events in immune thrombocytopenia occur mainly in 2 setting, namely after splenectomy and, in the venous, after immunoglobulin (IVIG) administration. The thrombotic event in postsplenectomy is likely due to the rebound platelet increase often observed after the procedure. On the contrary, the IVIG-related thrombotic events have been associated with clotting factors contaminants in the globulin preparation, to increased viscosity and to still undefined causes. 34
Both arterial and venous thromboses have been described in this setting but patients, in most instances, had a normal or even an increased platelet count. 3,10,34 The patients here presented are different, in the sense that they were all thrombocytopenic (platelet count less than 50000/μL) at the time of the thrombotic event regardless of the therapy. Furthermore, most of them have not received immunoglobulins. The pathogenetic mechanism is unknown. Cortisone may play an important role since a hypercoagulable state and actual thrombosis have been demonstrated in patients receiving this treatment. 35 The same is true for patients with Cushing syndrome. The hypercoagulable state of Cushing syndrome has been extensively studied by our group and found to be due to decreased fibrinolysis secondary to increased plasminogen activation inhibitor (PAI) levels, high FVIII levels, and increased presence of high molecular weight von Willebrand factor (vWF) multimers. 36,37,38 These multiple changes indicate a complex hypercoagulable state involving clotting factors (increased FVIII) and potential platelet hyperaggregation (presence of high-molecular-weight vWF multimers) and decreased fibrinolysis (increased PAI levels). It is difficult or impossible to indicate which of these conditions plays the most important role. Since increased FVIII levels have been demonstrated to be, alone, a cause of venous thrombosis, it is likely that this may play a major role. 39,40 Thrombosis in Cushing syndrome are frequent, particularly in the peri- and postoperative states. Adequate anticoagulant prophylaxis has been demonstrated to reduce drastically the surgery-related thrombosis. 41
At least 19 of the 26 patients here discussed were receiving cortisone therapy during the period immediately before or at the time of the thrombotic event occurred. This represents surely a clear majority even though not a constant finding. Since Cushing patients are not thrombocytopenic and do not bleed, one should admit that cortisone therapy may overcome the antithrombotic effect of a low platelet count. Cortisone therapy is likely to play always a role since even patients who developed thrombosis after splenectomy or after IVIG had been treated previously with prednisone or equivalent steroid. Actually, cortisone was maintained to play a major role even in IVIG-related thrombosis. 42 However, in the case of thrombotic events secondary to IVIG, the role of residual clotting factor or other impurities cannot be ruled out. 34 Finally, it has to be noted that cortisone therapy cannot be fully equated to the condition existing in Cushing syndrome. Prednisone in fact is mainly a glycoactive compound while cortisol is mainly mineraloactive.
The presence of young, large, hyperactive platelets, typical of chronic thrombocytopenia, or the presence of platelet microparticles could also be implicated as a possible prothrombotic factor in order to justify the higher prevalence of arterial thrombosis. 8,22,33
The results of this study indicate that patients with thrombocytopenia on prednisone therapy may represent a prothrombotic condition that, alone or in association with other risk factors (diabetes, hypertension, old age, IVIG administration, or even splenectomy), may contribute to the occurrence of thrombotic events. In a small group of prednisone-treated patients with thrombocytopenia without thrombosis we found, as expected, a coagulation pattern similar to that seen in Cushing syndrome (Girolami A, unpublished observations).
The majority of the thrombotic events are arterial and concern mainly the coronary arteries. Cerebrovascular and peripheral arterial occlusions are rare and the reasons for this discrepancy are unknown. It seems that patients with thrombocytopenia have a predilection for coronary disease.
As far as venous thrombosis are concerned, there is, contrary to what seen for arterial thrombosis, an equal prevalence of DVT and cerebral sinuses thrombosis. No report of portal vein thrombosis has been published, contrary to what seen in essential thrombocythemia. In the case of venous thrombosis, cortisone therapy also seems to play a role since the majority of patients had been taking this medication at time of thrombosis. This is in agreement with the observation that elevated FVIII levels seem to be associated mainly with venous thrombosis. 38
The limitation of this study concerns the fact that only a few of these patients were studied for congenital thrombophilia. It would have been particularly important to exclude this for the 2 female patients who presented venous thrombosis at the age of 12 and 13 years.
The indications for the management of thrombosis in patients with thrombocytopenia have not been established yet. However, the overall tendency emerging from this critical review is to treat them as normal participants even though every attempt has to be made to raise platelet number by immunoglobulins or by platelet transfusions. This is particularly so in case of invasive procedures for coronary syndromes. The discontinuation of cortisone therapy would seem to be indicated on the basis of the studies on Cushing syndrome. 40,41
However, this has never been attempted probably because of the lack of alternatives or for fear to cause a further decrease in platelet count with consequent danger of bleeding. The recent interest in the relation existing between patients with low platelet count and thrombosis is well demonstrated by the observation that thrombotic events may occur even in congenital thrombocytopenias. 43,44
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: in part by the Associazione Emofilia ed altre Coagulopatie delle Tre Venezie.