
Abstract
In this study, we aimed to investigate the value of mean platelet volume (MPV), platelet distribution width (PDW) and platelet count in cerebral venous sinus thrombosis (CVST) patients and in control subjects. Fifty-three patients with evidence of CVST and thirty-five controls with similar baseline characteristics were included in the study. CVST patients were further divided into two subgroups based on the presence or absence of parenchymal lesions in cranial MRI. Our analyses revealed a significant difference in MPV and PDW values between CVST patients with lesions and controls (P < 0.05). MPV and PDW values were significantly increased in CVST patients with brain parenchmal lesions, suggesting that MPV and PDW values can be used to predict the severity of CVST.
Introduction
Cerebral venous sinus thrombosis (CVST) is a rare but serious neurological disease. The CVST accounts for approximately 1% of all strokes. 1 All age groups can be affected, but it usually affects younger adults. 1 , 2 The clinical presentation and prognosis depend on the size of the thrombotic process and its location and severity. Poor prognostic factors include older age, coma, cortical and deep cerebral venous system involvement, increased intracranial pressure, parenchymal involvement (edema and hemorrhage), and complications such as pulmonary embolism. 1 –3
The process of venous thrombosis is not completely understood. Unlike arterial thrombosis, damage of the vessel wall is not necessary in venous thrombosis. Thrombosis begins with the aggregation of erythrocytes, fibrin, and platelets. 4,5 Platelets produce proinflammatory molecules and these proinflammatory molecules have prothrombotic activity, which leads to the formation and progression of pathological thrombosis with activated gp2b/3a. 6 The spread of peripheral venous thrombi is limited, likely by valves. In contrast, the spread of cerebral dural sinus thrombosis is common due to a lack of valves and this may influence the prognosis. 7,8
The mean platelet volume (MPV) and platelet distribution width (PDW) are parameters of platelet volume that can be determined routinely in nearly all clinical laboratories. Although some reports indicate PDW as a specific marker, 9 MPV is widely used to measure the platelet size. 10,11 The combined use of MPV and PDW could predict activation of coagulation more efficiently. 9 Large platelets are metabolically and enzymatically more active than small platelets and large platelets produce more thromboxane A2 and beta thromboglobulin, which has prothrombotic features and is associated with increased platelet activity, including increased platelet aggregation and increased adhesion molecule expression. 10 –12 The MPV and PDW are increased in patients with vascular diseases, diabetes mellitus, acute myocardial infarction (MI), and hypercholesterolemia. 13 –18
In a literature search of venous vascular events, we found few reports about MPV and venous thrombosis. In 1 venous thromboembolism study, an increased MPV was identified as a predictor of venous thromboembolism, such as deep vein thrombosis and pulmonary embolism. 19 –21 No study has examined PDW and venous thrombosis. In this study, we investigated the value of MPV and PDW in patients with CVST. In addition, we examined the association between MPV and PDW and the severity of disease.
Methods and Materials
The study included 53 cases of CVST admitted to our clinic within 24 hours after the onset of symptoms between March 2008 and December 2011. Patients with pregnancy, arterial stroke, peripheral vascular disease, infection, acute MI, hypertension, diabetes mellitus and medical treatment with antiaggregants, anticoagulants, and lipid-lowering drugs were excluded.
The diagnosis of CVST was based on a clinical evaluation, cranial magnetic resonance imaging (MRI), MR-venography, or digital subtraction angiography (DSA). The patients’ medical history and medication use were determined and the patients underwent physical and neurological examinations. Routine hematological and biochemical analyses were determined for CVST groups, including glucose, blood urea nitrogen, creatinine, liver function tests, electrolytes, and thyroid function tests. Antinuclear antibody, anti-double stranded DNA, lupus anticoagulant, antiphospholipid antibodies, protein S and C, antithrombin III, and factor V Leiden mutation were also tested. The prothrombin gene mutation (G20210) was analyzed in some patients with CVST.
The patients were divided into 2 subgroups based on the presence (n = 23) or absence (n = 30) of MRI parenchymal lesions. There were 35 healthy, age- and sex-matched individuals for comparison with patient group.
The mean age was 34.8 ± 11.4 (range 20-66) years in the no-lesion group, 36.5 ± 15.7 (19-74) years in the lesion group, and 35.3 ± 12.5 (range 20-68) in the controls. The female/male ratio was 25/5 for the no-lesion group, 17/6 for the lesion group, and 26/9 for the controls. The sex distribution and mean age were similar in all 3 groups.
Blood samples for MPV and platelet counts (PCs) were collected within the first 24 hours of hospitalization. All blood samples were taken from the antecubital vein. Both MPV and PC were measured on a Beckman Coulter LH 780 Hematology Analyzer (Beckman Coulter Inc., Brea, CA, USA). In our laboratory, the normal values are as follows: MPV: 6.8 to 10.8 fL, PDW: 11 to 15, and PC: 156 000 to 353 000/mL.
We compared the MPV, PDW, and PC values among the patients with CVST (both with lesion group and no-lesion group) and controls.
Statistical analysis was performed using the Statistical Package for the Social Sciences, ver. 16.0 (SPSS, Chicago, Illinois). Age was compared between the groups using the independent sample t test. Categorical variables such as sex were analyzed using the chi-square test. The distribution of continuous variables was tested for normality using the Kolmogorov-Smirnov test (P < .05). The Mann-Whitney U test was used to compare MPV, PDW values, and the PC. Statistical differences in the MPV, PDW, and platelet values were compared among CVST with brain parenchymal lesions, CVST without brain parenchymal lesions, and control groups using the Kruskal-Wallis test. The post hoc Bonferroni correction was performed to determine any significant main effects or interactions. P values ≤.05 were taken as significant.
Results
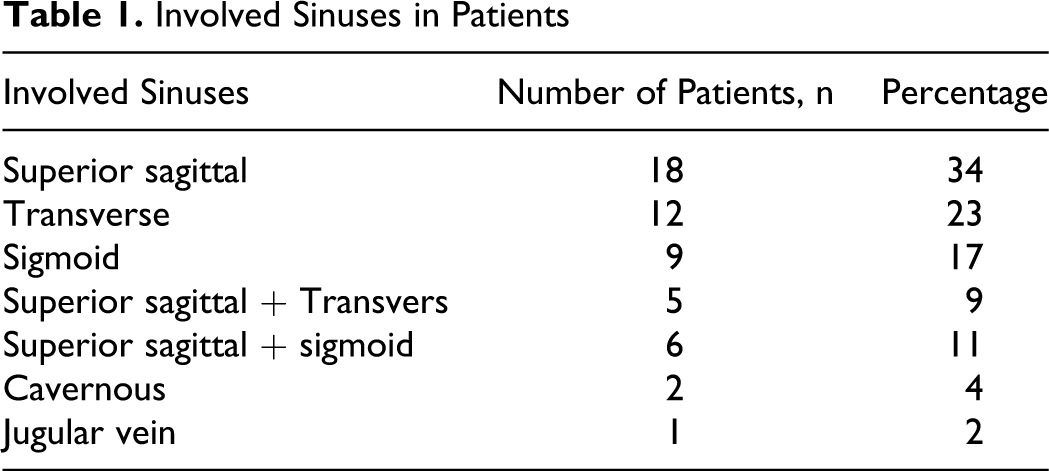
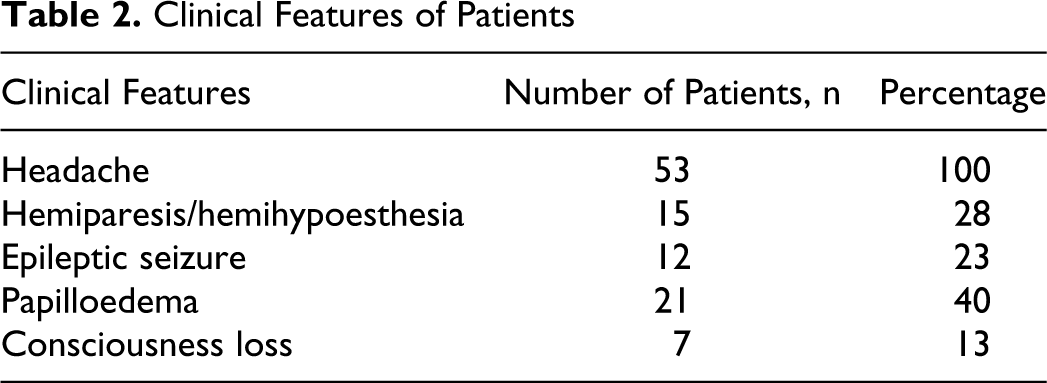
The diagnosis of CVST was confirmed by MRI and MR venography in 51 cases; DSA was performed in 2 cases. The most frequently affected sinuses were the superior sagittal and transverse (Table 1). We divided the patients into 2 subgroups based on the presence or absence of MRI parenchymal lesions. Twenty-three patients presented with venous infarction on cranial MRI. The most prevalent symptom was headache, which was found in all patients (Table 2).
Involved Sinuses in Patients
Clinical Features of Patients
The PC, PDW, and MPV values were compared among the 3 groups listed in Table 3. Also the comparison of MPV and PDW between patients with CVST and controls is shown in Figures 1 and 2. The PC was higher in the CVST groups, but the difference between the controls and both CVST groups was not significant with P = .08. We found a significant difference in the PDW among the controls and total CVST group with P = .003. We did not find significant differences in MPV between the total CVST group and controls (P = .3), but there was a significant difference among the CVST lesion group and controls (P < .001).
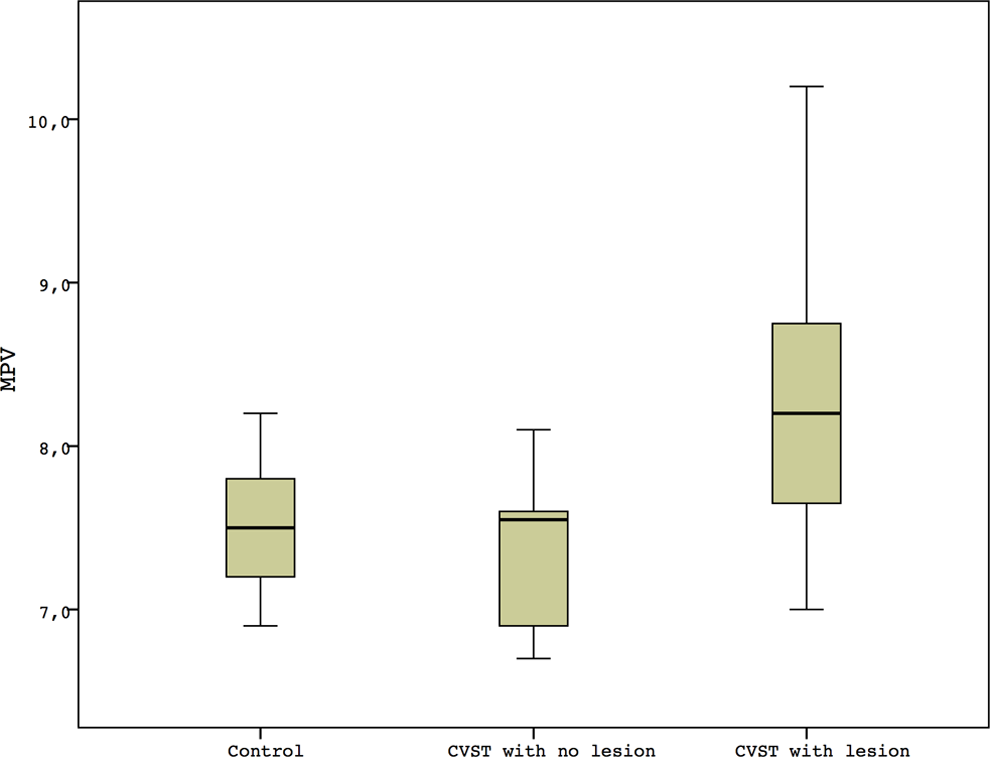
Comparison of MPV in patients with CVST groups and controls. CVST indicates cerebral venous sinus thrombosis; MPV, mean platelet volume.
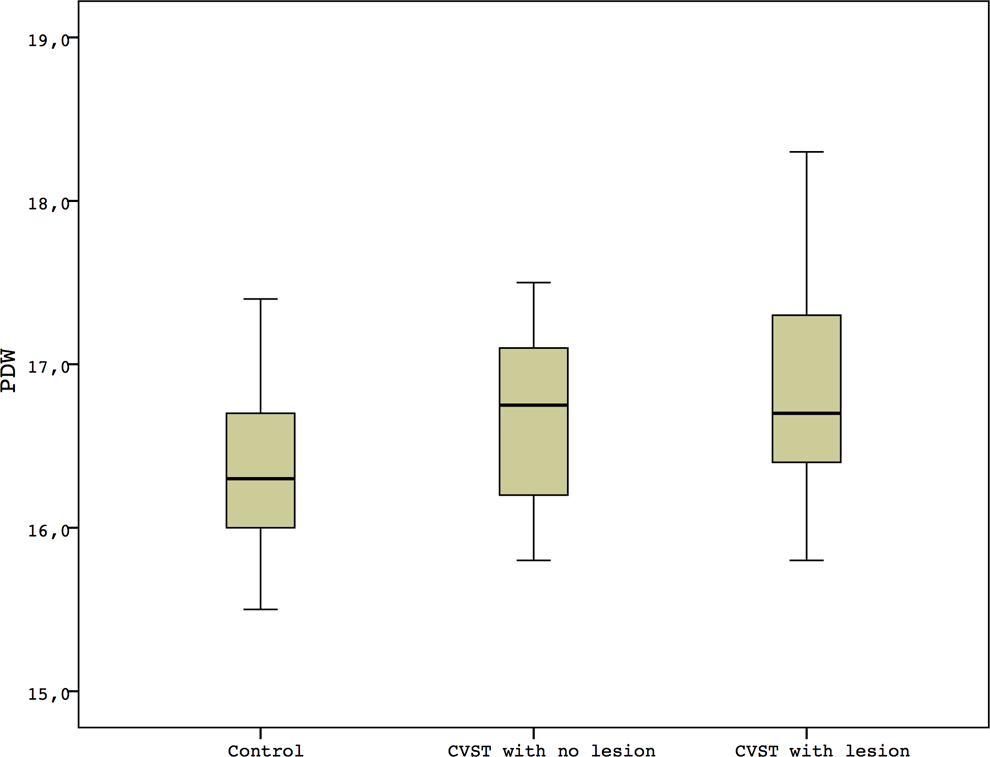
Comparison of PDW in patients with CVST groups and controls. CVST indicates cerebral venous sinus thrombosis; PDW, platelet distribution width.
Demographic Data and Laboratory Parameters of Patients and Controls
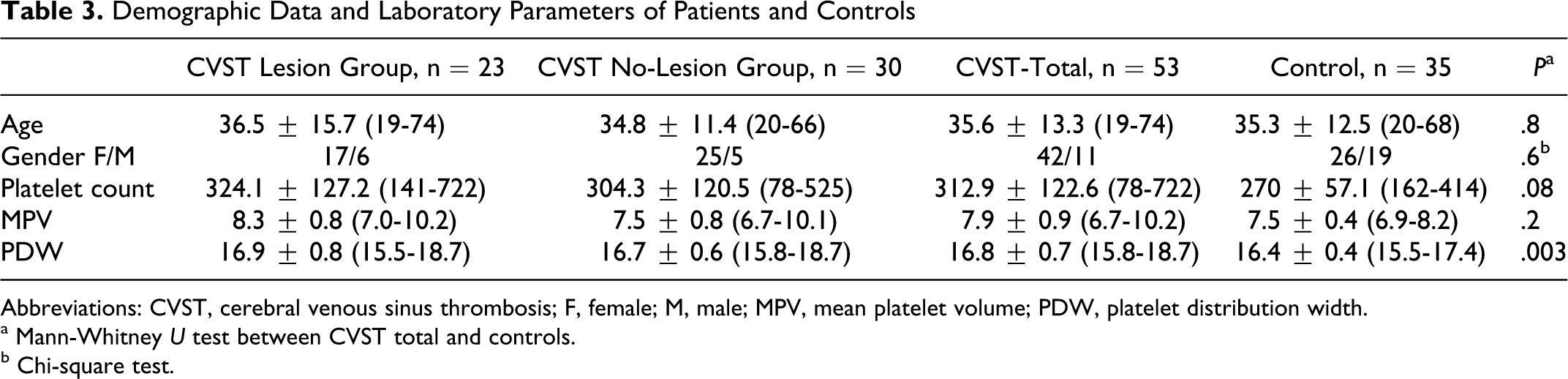
Abbreviations: CVST, cerebral venous sinus thrombosis; F, female; M, male; MPV, mean platelet volume; PDW, platelet distribution width.
a Mann-Whitney U test between CVST total and controls.
b Chi-square test.
Discussion
We aimed to investigate the platelet indices (MPV and PDW) in the early phase of patients with CVST. We found that MPV and PDW are raised in patients who have suffered CVST with brain parenchymal lesions.
O'Malley et al found a higher MPV in patients with acute ischemic stroke than controls, but they did not detect any significant differences in the MPV between the acute and chronic phases of stroke. 22 Platelets have a mean life of 8 days; therefore, a higher MPV may affect the acute phase of stroke. In another study, Muscari et al found higher MPV values in arterial stroke with the greatest neurological impairment. 23 In addition, MPV was higher in the coronary artery disease infarct group. 24 There are only a few studies about MPV and peripheral venous thromboembolism. The Tromsø Study investigated the role of MPV and PC in peripheral venous thromboembolism in patients with deep vein thrombosis and pulmonary embolism. Participants with a higher MPV had a significantly increased risk of unprovoked venous thromboembolism than normal participants. 19
Although MPV is the most extensively studied platelet activation marker, recently PDW has been investigated as prospective platelet activation marker. 17,18,22 Platelet activation leads changes in morphology of platelets as spherical shape and pseudopodia formation. These changes possibly reflect the PDW. 9 Amin et al reported increased PDW in vasoocclusive crisis in sickle cell anemia. 25 Also increased PDW was found in coronary artery disease, myeloproliferative disorders, and diabetes mellitus. 24,26 The PDW is thought to be a more specific marker of platelet activation. 9
We found increased MPV and PDW values with brain lesions and severe neurological abnormalities in patients with CVST. This may be related in response to the production of cytokines and hormonal factors in parenchymal lesion with CVST. Our findings suggest that the increased MPV and PDW contribute to the prethrombotic situation in the acute phase of CVST and larger platelets may play an important role in infarction. Increased MPV and PDW may be a predictive factor for poor prognosis as age, coma, cortical and deep cerebral venous system involvement, increased intracranial pressure, and parenchymal involvement. Our patients were young and most of them have no comorbid disease like hypertension, coronary artery disease, or diabetes mellitus which may lead to increase in MPW and PDW. So our findings suggest that increased MPV and PDW may be related to acute reaction in patients with CVST.
Limitations of our study include the absence of other markers of platelet activation and aggregation markers, thrombotic status, and fibrinolytic status. In addition, there was no follow-up. Therefore, we do not know the late-stage course or prognostic importance of MPV and PDW in patients with CVST.
In conclusion, platelet indices (MPV and PDW) can easily be identified using routine hematological analyses. It is a simple, important, and cost-effective parameter that can be used widely to predict the severity of vascular disease. Increased MPV and PDW may predict the presence of severe and extended parenchymal lesions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.