
Abstract
Keywords
Introduction
Coronary artery ectasia (CAE), an abnormality of the coronary anatomy, has been defined as a dilatated artery luminal diameter that is 1.5 or more times greater than the diameter of the normal portion of the artery. 1 The incidence of CAE has been found in up to 5% of angiographic and in 0.22% to 1.4% of autopsy series.2,3 The CAE can cause angina pectoris and even myocardial infarctions in patients without coronary artery disease (CAD). The underlying mechanism of the abnormal luminal dilatation seen in CAE is not entirely known. 4
Red cell distribution width (RDW) is a numerical measure of the size variability in circulating erythrocytes. 5 This parameter is routinely used by physicians in clinical practice as part of the automated complete blood count (CBC), in particular it is mainly used for the differential diagnosis of anemia. 6 Recent studies have demonstrated a strong independent association between levels of high RDW and the risk of adverse outcomes in patients with cardiovascular disease,7,8 acute coronary syndromes,9,10 heart failure,11,12 and also in the general population. 13 However, to the best of our knowledge, there is no study regarding the assessment of RDW in patients with CAE in the literature. Therefore, the aim of our study was to evaluate the levels of RDW in patients with CAE.
Methods
Study Population
We prospectively evaluated patients who underwent coronary angiography in our catheter laboratory. The first group consisted of 54 patients (CAE group, 28 males; mean age, 59 ± 12) with isolated CAE without significant stenosis. These patients are selected from individuals who had undertaken coronary angiography because of the presence of chest pain or positive or equivocal results of noninvasive screening tests for myocardial ischemia. The second group consisted of 40 consecutive participants with angiographically shown normal coronary arteries without CAE (control group, 17 males; mean age, 56 ± 10 years). Patients were excluded from the study if they had obstructive CAD, acute coronary syndrome, cardiomyopathy, valvular heart disease, and chronic obstructive pulmonary disease. This study complied with the Declaration of Helsinki and was approved by the local ethics committee.
Coronary Angiograms
Conventional coronary angiography was performed in all patients after admission. Femoral artery cannulation was used for arterial access site and Judkins system was applied for cannulation of the left and right coronary arteries. After obtaining images by standard approaches, each angiogram was interpreted by 2 independent cardiologists. The diagnosis of CAE was rendered if any 1.5-fold or greater dilatation was evident, relative to adjacent normal coronary segments. 3 When there was no identifiable adjacent normal segment, the mean diameter of the corresponding coronary segment in the control group served as the normal value. According to the results of coronary angiography, significant coronary artery stenosis was defined as ≥50% of major coronary arteries.
Laboratory Parameters
Blood samples were drawn from an antecubital vein before coronary angiography after a 12-hour overnight fast. Blood glucose, high-sensitive C-reactive protein (hs-CRP), total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglyceride levels were recorded. Hematological parameters, including hemoglobin (Hb), white blood cell (WBC) count, RDW, and platelet count, were analyzed by standard methods.
Statistical Analysis
SPSS 15.0 statistical program (SPSS, version 15.0 for Windows; SPSS, Chicago, Illinois) was used for statistical study. Continuous variables were expressed as mean ± standard deviation and categorical variables were expressed as percentage. Continuous variables were compared using the Student t test or Mann-Whitney U test. The χ2 test or the Fisher exact test was applied for the catagorical variables. A probability value of P < .05 was considered significant for all statistics.
Results
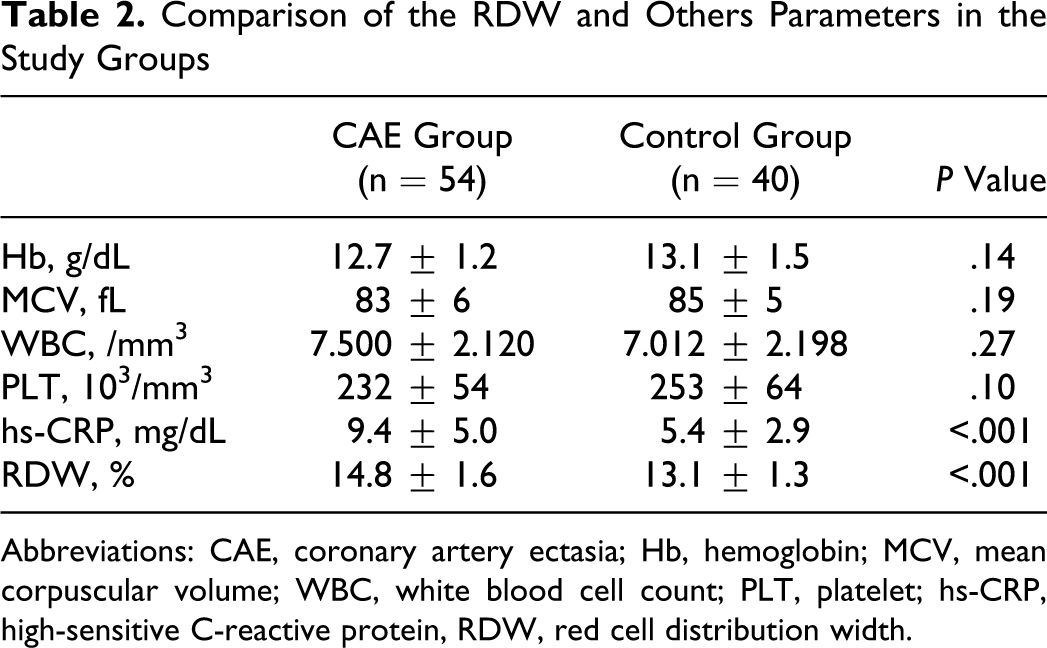
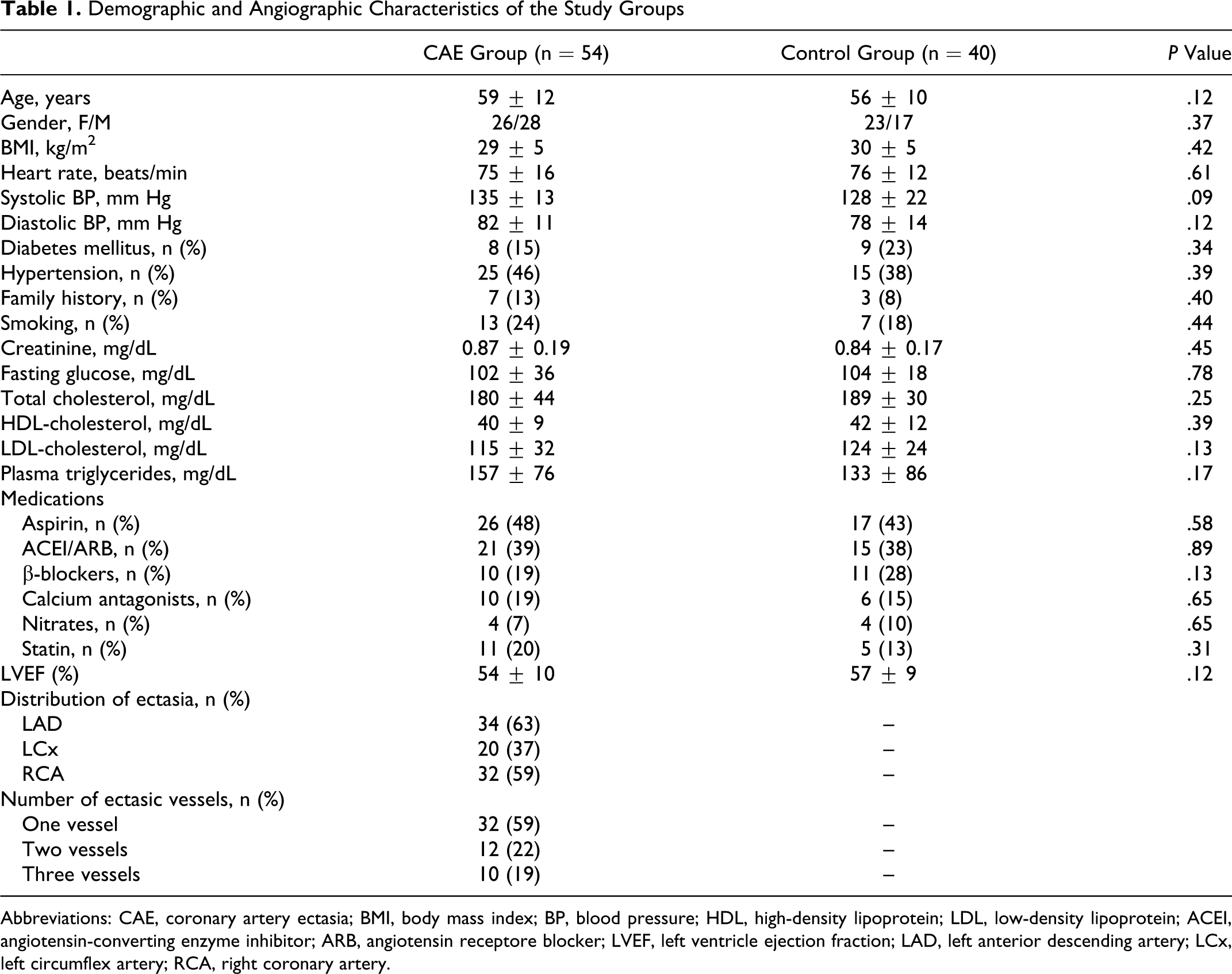
The baseline characteristics of the study groups are shown in Table 1. According to the basic clinical and demographic characteristics, both groups of the study were similar with respect to age and gender. Both groups were similar in blood pressure, heart rate, left ventricular ejection fraction, medications and incidence of hypertension, diabetes mellitus, and other cardiovascular risk factors (P > .05). Also, angiographic features of CAE were given in Table 1. In the Hb and mean corpuscular volume, there were no significant difference in the CAE group compared with the control group (12.7 ± 1.2 g/dL vs 13.1 ± 1.5 g/dL, P = .14 and 82.8 ± 5.9 fL vs 84.6 ± 4.8 fL, P = .19, respectively). There was no significant difference in platelet and WBC count between the groups (P > .05; Table 2).
Demographic and Angiographic Characteristics of the Study Groups
Abbreviations: CAE, coronary artery ectasia; BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptore blocker; LVEF, left ventricle ejection fraction; LAD, left anterior descending artery; LCx, left circumflex artery; RCA, right coronary artery.
Comparison of the RDW and Others Parameters in the Study Groups
Abbreviations: CAE, coronary artery ectasia; Hb, hemoglobin; MCV, mean corpuscular volume; WBC, white blood cell count; PLT, platelet; hs-CRP, high-sensitive C-reactive protein, RDW, red cell distribution width.
The RDW was significantly higher in the CAE group than the control (14.8 ± 1.6 vs 13.1 ± 1.3, respectively, P < .001). Also, hs-CRP levels in the patients with CAE were significantly higher as compared with controls (9.4 ± 5.0 and 5.4 ± 2.9 mg/L, respectively, P < .001; Table 2).
Discussion
This is the first study to evaluate RDW levels in patients with CAE. We showed that RDW was significantly higher in the CAE group compared with the control group. Additionally, hs-CRP levels in the patients with CAE were significantly higher as compared with controls.
The RDW reflects variability in the size of circulating red cells (anisocytosis) and is routinely reported by analysers as part of the routine CBCs. 5 The formula for calculating RDW is (standard deviation of red cell volume/mean cell volume) × 100. Thus, elevated RDW means that there is heterogeneity of cell sizes in the peripheral blood smear.14,15 Increased RDW can be seen in hemolysis, nutritional deficiencies such as iron, vitamin B12, and folate, or after blood transfusion. 8 Additionally, an elevated RDW levels can result from conditions that modify the shape of red blood cells due to the premature release of immature cells into the bloodstream (severe blood loss), abnormal Hbs (eg, sickle cell anemia), hemolysis, or hemolytic anemias.5,14
Previous studies have reported a strong association between increased RDW and cardiovascular mortality and morbidity in different populations. In 2 large heart failure populations (CHARM and DUKE Databank), RDW was demonstrated to be a very strong independent predictor of morbidity and mortality. 11 In another study, Cavusoglu et al 9 demonstrated that increased RDW was a strong independent predictor of all-cause mortality in an unselected population of male patients referred for coronary angiography. Also, Patel et al 13 measured RDW in a healthy sample of 8175 adults aged >45 and found that for every 1% increment in RDW, the all-cause mortality risk increased by 22%. The physiological mechanisms that underlie the association of RDW with CAE are entirely unknown, systemic factors that alter erythrocyte homeostasis, such as inflammation and oxidative stress, likely play a role. Aydin et al 16 showed that higher levels of inflammation markers (interleukin 6 [IL-6], tumor necrosis factor-α [TNF-α]) were associated with CAE. Also, Sezen et al 17 demonstrated that the relationship between oxidative stress and CAE existed. Inflammation might contribute to an increased RDW by impairing iron metabolism, inhibiting the production of or response to erythropoietin, and shortening red blood cell survival.18,19 Additionally, in previous studies, inflammatory cytokines have been found to suppress the maturation of erythrocytes, thus immature erythrocytes enter into the circulation and may accelerate erythropoiesis.20,21 These conditions lead to an increase in the heterogeneity of circulating erythrocytes. The RDW is widely available to clinicians as a part of the CBC and hence incurs no additional costs.
Study Limitations
The major limitation is that this is a cross-sectional design of the study. Another limitation in this study was that we did not measure inflammatory cytokines. Despite adjusting for multiple risk factors, it is possible that there may have been residual confounding conditions and medications, for example, folate, iron, and vitamin B12. In addition, RDW was assessed only once. We have no data on changes in RDW levels during the course of hospital stay.
In conclusion, this study demonstrates that the RDW and hs-CRP were higher in the CAE group compared with the control group. These results showed that RDW is a reliable, simple, and inexpensive marker for patients with CAE, but further studies with a greater sample size are needed to confirm our results.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.