
Abstract
We assessed the potential safety of withholding treatment of pulmonary embolism (PE) limited to subsegmental branches. Literature review showed that untreated patients with mostly subsegmental PE had no fatal recurrences in 1 to 3 months and no nonfatal recurrences of PE in 3 months. Patients with suspected PE who had nondiagnostic ventilation/perfusion lung scans, adequate cardiorespiratory reserve or low or moderate clinical probability, and negative serial noninvasive leg tests were shown not to require treatment. It appears safe, therefore, to withhold treatment of subsegmental PE providing (1) pulmonary–respiratory reserve is good; (2) no evidence of deep venous thrombosis (DVT) on serial testing; (3) major risk factor for PE was transient and no longer present; (4) no history of central venous catheterization or atrial fibrillation; and (5) willingness to return for serial venous ultrasound. After fully informing patients, some may choose to be treated and some may choose not to be treated.
Interest in subsegmental pulmonary embolism (PE) has intensified with the ability to show such apparent small PE with contrast-enhanced computed tomography (CT). 1 The clinical relevance of isolated subsegmental PE and the management of such patients are uncertain. 1 The diagnosis of isolated subsegmental PE is uncertain, 2 although images with thin-collimation multidetector CT are compelling.3–5 The purpose of this article is to update evidence related to the diagnosis and management of isolated subsegmental PE.
Prevalence
Small PE at Autopsy
The existence of PE in small pulmonary artery branches is not a recent discovery. A detailed postmortem investigation of small PE was published in 1964. 6 The authors used arteriography of the cannulated and inflated lungs following injection of a barium sulfate–gelatin–mercury mass or later by a gelatin–potassium iodide–barium sulfate preparation. This was followed by careful dissection and histological examination. Among the 34 patients with recent PE as a terminal event, the astounding observation at autopsy was that PE lodged in muscular arterial segments (0.1-1 mm diameter) in every case (34 of 34, 100%), in arterioles (0.03-0.1 mm) in 13 (38%) of 34, and in elastic arteries (≥1 mm diameter) in only 8 (24%) of 34. Conventional pulmonary angiography and CT pulmonary angiography would, at best, show only elastic pulmonary arterial branches (≥1 mm diameter). Only the minority of patients in this necropsy study, therefore, had PE of a size that one could hope to see with the best imaging techniques.
Small PE as a Cause of Chronic Thromboembolic Pulmonary Hypertension
Patients with chronic thromboembolic pulmonary hypertension may have (1) central organized thrombi in the main or lobar pulmonary arteries, (2) intimal thickening and fibrosis proximal to the segmental arteries, (3) disease with distal segmental and subsegmental arteries only, or (4) hypertensive distal vasculopathy without visible thromboembolic disease. 7 These may occur alone or in combination. 7 Disease of distal segmental and subsegmental arteries only was observed in about 12% of patients in this selected group who underwent operation for chronic thromboembolic pulmonary hypertension. 7
Isolated Subsegmental PE
The reported prevalence of isolated subsegmental PE is shown in Table 1.2,3,8–27 In Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) II, with mostly 4-detector CT angiograms, 8 (4%) of 181 patients with PE showed isolated subsegmental PE. 2 We define isolated subsegmental PE as a PE shown on CT angiography that occurred in a subsegmental branch but no larger order of vessels. The subsegmental PE may involve one or more than one subsegmental branch.
Prevalence of Isolated Subsegmental PE on CT or Conventional Pulmonary Angiograms
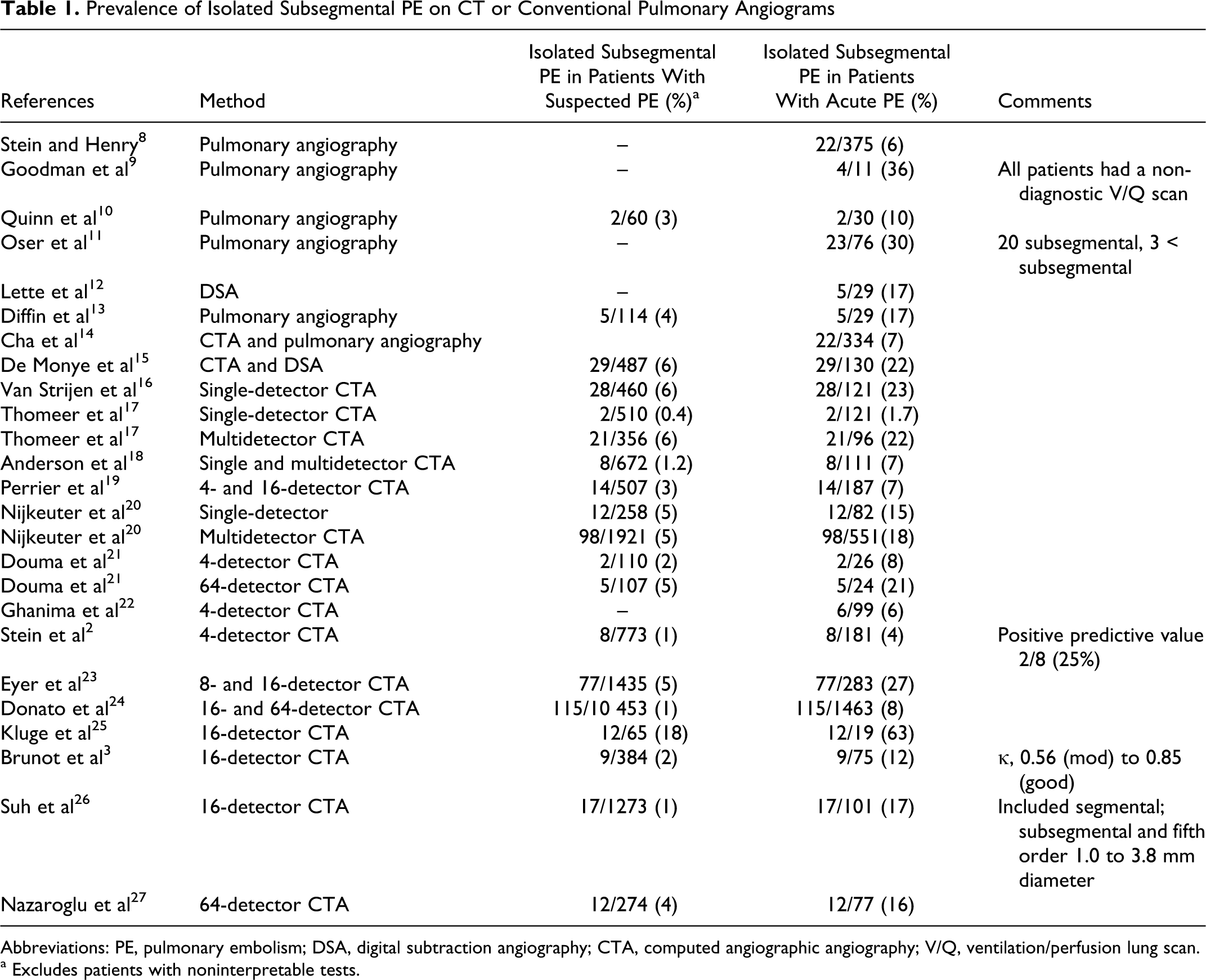
Abbreviations: PE, pulmonary embolism; DSA, digital subtraction angiography; CTA, computed angiographic angiography; V/Q, ventilation/perfusion lung scan.
a Excludes patients with noninterpretable tests.
Incidental PE
Incidental PE may be found in asymptomatic patients who undergo CT angiography for reasons other than suspected PE.28–31 Ritchie et al, with 4- and 16-detector CT angiography, found unexpected PE in 28 (6%) of 487 patients who underwent contrast-enhanced CT for reasons other than suspected acute PE. 31 Among these, isolated subsegmental PE was identified in 5 patients. Others,29,32 with single-detector CT angiography, found unexpected PE in 1% to 2% and with 4-detector CT angiography found 30 unexpected PE in 3%. None of these investigators found isolated subsegmental PE.28–30 Dexter, in a prior generation (P. D. Stein and J. E. Dalen, personal communication, 1964), and more recently Gurney suggested that one of the normal functions of the lung is to remove small emboli, which, if allowed to enter the arterial circulation, would have disastrous consequences. 33 Such PE would be completely asymptomatic. Thus, many small PE may be a normal part of existence and unrecognized until identified by CT angiography or autopsy.
Diagnosis
Wedge Pulmonary Angiography
With considerable effort, and a technique no longer used, it was possible to show intraluminal filling defects in pulmonary arterial branches of 1.5 to 2.0 mm diameter. 34 This was accomplished by wedge arteriography, where a 7F size (2.3 mm diameter) end-hole catheter was wedged into a pulmonary artery branch and 1.0 mL of contrast material was injected. Pulmonary branches of 0.2 mm diameter can be clearly shown. Short of this technique, with superselective injections into the pulmonary artery (not wedge injections) cutoffs of small branches and filling defects of branches not quite so small can be shown. Diminished arborization of peripheral pulmonary arterial branches is not necessarily indicative of microemboli and can be seen in severe lung disease. 35
Computed Tomographic Angiography
The positive predictive value of apparent isolated subsegmental PE in PIOPED II was only 2 (25%) of 8. 2 Of the 773 patients with complete data in PIOPED II, 36 4-slice scans were used in 691 (89%); 8-slice scans in 37 (5%); and 16-slice scans in 45 (6%). Imaging with 64-detector CT may be more accurate, but there is no readily available reference test to establish this.
Review by Le Gal et al indicated that single or multiple subsegmental PE were identified more frequently in patients with suspected PE evaluated by multidetector CT angiography, 17 (2.2%) of 770, than with single-detector CT angiography, 37 22 (1.0%) of 2232. Carrier et al, based on systematic review, found isolated subsegmental PE in 4.7% of patients with PE diagnosed by single-detector CT and in 9.4% of patients with PE diagnosed by multidetector PE. 32 Ghaye, in a review of patients with confirmed PE, also reported more subsegmental PE identified with multidetector CT angiography than with single-detector angiography. 5
Present day clinical experience is that the clot burden in patients with isolated subsegmental PE is small. Deep venous thrombosis (DVT) is usually absent in patients with PE limited to subsegmental branches.26,27
Treatment and No Treatment
Outcome of Untreated Patients With Isolated Subsegmental PE
Only a few investigations have shown the outcome of untreated patients with isolated subsegmental PE (Table 2).14,23,24,38,39 The evidence suggesting that patients with subsegmental PE could do without treatment comes from small retrospective cohort series. Most untreated patients had no evidence of DVT. Pooled data in 105 untreated patients with mostly isolated subsegmental PE, but in some with PE in larger brunches, showed no fatal recurrences in 1 to 3 months.14,23,24,38,39 There were 0 (0%) of 58 nonfatal recurrences of PE in 3 months.14,23,24,38 Major hemorrhage24,39 from anticoagulants occurred in 7% to 8%.
Treatment With Anticoagulants Compared With No Treatment of Isolated Subsegmental Pulmonary Embolism
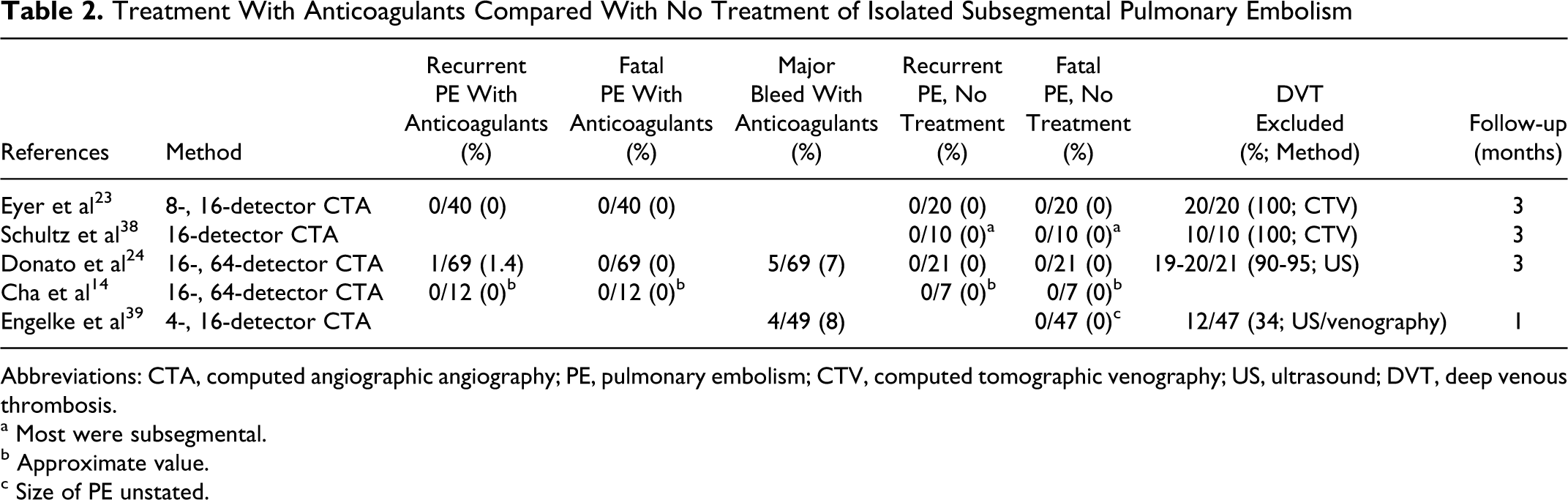
Abbreviations: CTA, computed angiographic angiography; PE, pulmonary embolism; CTV, computed tomographic venography; US, ultrasound; DVT, deep venous thrombosis.
a Most were subsegmental.
b Approximate value.
c Size of PE unstated.
Risk of Major Bleeding and Death From Anticoagulants
Meta-analysis of bleeding rates reported in 33 studies was performed. 40 Data included 10 757 patients with venous thromboembolism who were treated 4374 patient-years with vitamin K antagonists for at least 3 months (target international normalized ratio 2.0-3.0). Major bleeding occurred in 7% per year. Fatal bleeding occurred in 1.3% per year. The case fatality rate for major bleeding was 13.4%. 40 In the initial 3 months of treatment, major bleeding occurred in 2.1% and fatal bleeding occurred in 0.4%. 40 In the Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry, 1880 patients with PE were treated with anticoagulants. 41 During the initial hospitalization, 0.2% died from bleeding. In general, therefore, 2 to 4 of 1000 patients died from anticoagulants in the first 3 months of anticoagulant therapy.
Possible Alternative to Treatment With Anticoagulants in Selected Patients
If some patients may not require treatment of PE with anticoagulants, what might be the characteristics of such a patient? The following seem to be a reasonable answer. (1) Adequate pulmonary–respiratory reserve, so if PE did recur, the likelihood is that it would not be fatal. Pulmonary–respiratory reserve was defined as adequate if none of the following were present: pulmonary edema, right ventricular failure, hypotension (systolic pressure <90 mm Hg), syncope, acute tachyarrhythmias, or respiratory failure shown by severely abnormal spirometry (forced expiratory volume in 1 second <1.0 L or vital capacity <1.5 L), or blood gas measurements (P
Hull et al introduced the concept that patients with suspected acute PE and nondiagnostic ventilation/perfusion lung scans, who have negative serial noninvasive tests of the lower extremities, do not require treatment with anticoagulants, provided cardiorespiratory reserve is adequate. 43 Others followed with the requirement that the pretest clinical probability of PE should be low or moderate. 44 Such untreated patients with unproven PE had a low (0.5%-0.6%) rate of PE on follow-up.42,44
The strategy of withholding treatment of acute PE if serial ultrasonography is negative is based on the observation that PE arises from DVT of the lower extremities in most patients. The safety of withholding treatment in patients with suspected PE, providing serial leg tests are negative, supports this observation.42,44 Autopsy showed DVT of the lower extremities in 80% to 97% of patients with PE.45–48 Thrombosis confined to pelvic veins or inferior vena cava is uncommon, 3 (3%) of 105 in PIOPED II. 2
Our finding 49 is that in the investigation 44 by Wells et al, 117 patients with PE may have been followed off-treatment. The rate of PE in 3 months would have been 3 (2.6%) of 117. This rate of recurrent PE was not higher than in patients treated with anticoagulants in PIOPED. 50 Among patients treated only with anticoagulants in PIOPED I, recurrent nonfatal PE, fatal recurrent PE or death from the initial PE occurred in 11 (3.7%) of 297 in the first 3 months. 50 Nearly the same results were shown among patients in the Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry (EMPEROR) after 30 days. 41 Death or recurrent PE in 30 days occurred in 69 (3.7%) of 1880 patients, among whom 98% were treated only with anticoagulants.
Accuracy of Venous Ultrasound for Diagnosis of DVT in Assessment for No Treatment
Among 149 patients with acute PE diagnosed by a high-probability lung scan or positive pulmonary angiogram, bilateral B-mode gray-scale compression ultrasonography of the proximal leg veins showed DVT in 43 (29%) of 149 patients. 51 Others showed DVT by B-mode compression ultrasound in 70 (43%) of 162 patients with PE diagnosed by a high-probability ventilation/perfusion lung scan 44 and in 35 (58%) of 60 patients diagnosed by a high-probability ventilation/perfusion lung scan in combination with a high clinical probability. 44 Based on autopsy data showing that on average, 92% of patients with PE had thrombi that originated in the lower extremities,45–48 the sensitivity of compression ultrasound would seem to be limited. Pooled data with compression ultrasound of the proximal deep veins in patients with clinically suspected symptomatic acute DVT, using contrast venography as a reference standard, showed a sensitivity in 234 (92%) of 253 patients and specificity in 325 (98%) of 330 patients.52–56
Pooled data with compression ultrasound in asymptomatic patients with a high risk of DVT, using contrast venography as a reference standard, showed sensitivity in 28 (55%) of 51 patients for proximal DVT.57–59 Specificity was found in 456 (94%) of 485 patients.57–59 More recently, 60 among patients who underwent hip or knee replacement and obligatory venography, the sensitivity of compression ultrasound for proximal DVT was only 21%. The low sensitivity may reflect that the venous thrombi are small, nonoccluding, or distal. 60 Sensitivity of ultrasound depends on the number of compression maneuvers performed. 61
It would seem that detection of DVT by compression ultrasound is potentially the only limiting factor in withholding treatment in patients with PE. The issue is not if venous ultrasound is accurate, but if it is accurate enough to detect DVT of sufficient size to be an important risk of PE. The investigation by Wells et al suggests that this is the case. 44
Accuracy of CT Venography for Detecting DVT in Assessment for No Treatment
Computed tomography venography and compression ultrasound are diagnostically equivalent. 36 There was 95.5% concordance between CT venography and ultrasound for the diagnosis or exclusion of DVT. 36 Diagnostic results in patients with signs or symptoms of DVT, asymptomatic patients, and patients with a history of DVT were similar irrespective of whether CT venography or ultrasound was used. In PIOPED II, with mostly 4-detector CT, 43 (4%) of 1062 of CT venograms were eliminated due to quality issues or lack of reader consensus. 36 Others, with 64-detector CT, showed insufficient quality of CT venography in 35 (11%) of 306 patients. 27
Published Recommendations
Recommendations for antithrombotic therapy for PE in the American College of Chest Physicians Evidence-Based Practice Guidelines (8th Edition) were that patients with PE secondary to a transient (reversible) risk factor should be treated with a vitamin K antagonist for 3 months. 62 For patients with unprovoked PE, it was recommended that treatment should be at least for 3 months and the risk–benefit ratio of long-term treatment should be considered. 62 For patients with PE and cancer, treatment was recommended for 3 to 6 months and probably indefinitely or until the cancer is resolved. In patients who were unexpectedly found to have asymptomatic PE, recommendations were the same for initial and long-term anticoagulation as for comparable patients with symptomatic PE. 62
The Fleischner Society suggested that the clinical relevance of small peripheral PE and the need to administer anticoagulants in such patients is a subject of debate. 63 They suggested that in patients with small PE and no DVT, the risks associated with anticoagulant therapy outweigh the benefits. They emphasized that because isolated subsegmental PE may herald subsequent PE, negative findings on the study of the lower extremities are mandatory. 63
Conclusion
Based on these data, we suggest that patients with isolated subsegmental PE need not be treated with anticoagulants, provided they meet the following criteria. (1) Good pulmonary–respiratory reserve; (2) no evidence of DVT with serial leg tests; (3) a transient (reversible) major risk factor for PE that is no longer present; (4) no history of central venous catheterization and no history of atrial fibrillation; and (5) a compliant and trustworthy patient who would return for serial noninvasive leg tests. With the information in hand, a clinician can now have a meaningful dialogue with a patient on the advantages and disadvantages of treating their isolated subsegmental pulmonary emboli. Some patients may choose to be treated or choose not to be treated. Further research is needed to clarify the need for anticoagulant therapy for subsegmental PE. The criteria for selecting patients who may not require treatment need to be validated in a prospective investigation. Ideally, this information should be provided by a randomized controlled trial.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.