
Abstract
Introduction
Systemic thromboembolism is a complication of aortic stenosis (AS). 1 Previous studies have demonstrated that platelet activation occurs in patients with AS.1–6 Evidence from several studies has shown that shear stresses in turbulent flow as a result of stenotic valves induce platelet activation.7–10
Mean platelet volume (MPV) is a simple and easy method of assessing platelet function.11,12 In comparison to smaller ones, larger platelets have more granules, aggregate more rapidly with collagen, have higher thromboxane A2 level, and express more glycoprotein Ib and IIb/IIIa receptors.13–15
Although it has been shown that platelet activation occurs in patients with AS, to the best of our knowledge, no study has examined MPV in patients with AS. In this study, we investigated the MPV in patients with AS to evaluate platelet activation in this group of patients.
Patients and Methods
Study Population
The study group consisted of 43 patients with predominant AS (23 females and 20 males, mean age 61.9 ± 13.7 years). An age-, gender- and body mass index−matched control group was composed of 35 healthy volunteers (19 females and 16 males with a mean age 59.1 ± 10.0 years). All patients and control participants underwent echocardiographic examination. The etiology was calcific AS in 28 patients and rheumatic AS in 15 patients. Echocardiographic evaluation in the control group revealed no abnormalities of cardiac structure and function. As a concomitant valvular disease, only mild aortic/mitral/tricuspid/pulmonary regurgitation without mitral/tricuspid/pulmonary stenosis was allowed. Exclusion criteria were left ventricular systolic dysfunction, known coronary artery disease, acute coronary syndrome, atrial fibrillation, history of renal or liver disease, malignancy, hematological disorders, acute or chronic infection, current use of lipid-lowering agents, and stroke. The study was approved by the local ethics committee, and all patients gave their informed consent.
Echocardiography
The M-mode, 2-dimensional, and Doppler echocardiographic examinations were obtained using GE VingMed System FiVe (Norway) to assess the basic echocardiographic measurements and aortic and other valvular assessment. Left atrial and ventricular dimensions and left ventricular ejection fraction were measured by M-mode echocardiography in the parasternal long axis view using the American Echocardiography Society M-mode technique. 16 Peak aortic velocity, peak aortic gradient, and mean aortic gradient were derived by Doppler. 17 Aortic and other valvular regurgitation were evaluated by Doppler color flow mapping.
Biochemical Measurements
Blood samples were drawn from the antecubital vein by careful veinpuncture in a 21-g sterile syringe without stasis at 08.00 to 10.00
Statistical Analysis
Data were analyzed with the SPSS software version 10.0 for Windows. Continuous variables from the study groups were reported as mean ± standard deviation and categorical variables as percentages. To compare continuous variables, the Student t test or Mann-Whitney U test were used where appropriate. Categorical variables were compared with the chi-square test. Statistical significance was defined as P < .05.
Results
Clinical features, laboratory, and echocardiographic findings of the study and control groups are summarized in Table 1. There were no statistically significant differences between the 2 groups with respect to age; gender; body mass index; systolic and diastolic blood pressures; and levels of glucose, creatinine, total cholesterol, triglyceride, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, hemoglobin, white blood cell count (WBC), and platelet count. Mean platelet volume was significantly higher in patients with AS when compared with control group (8.7 ± 1.0 vs 7.9 ± 0.9 fL, respectively; P = .001).
Comparison of Clinical, Laboratory, and Echocardiographic Findings of the Aortic Stenosis Patients and Control Participants
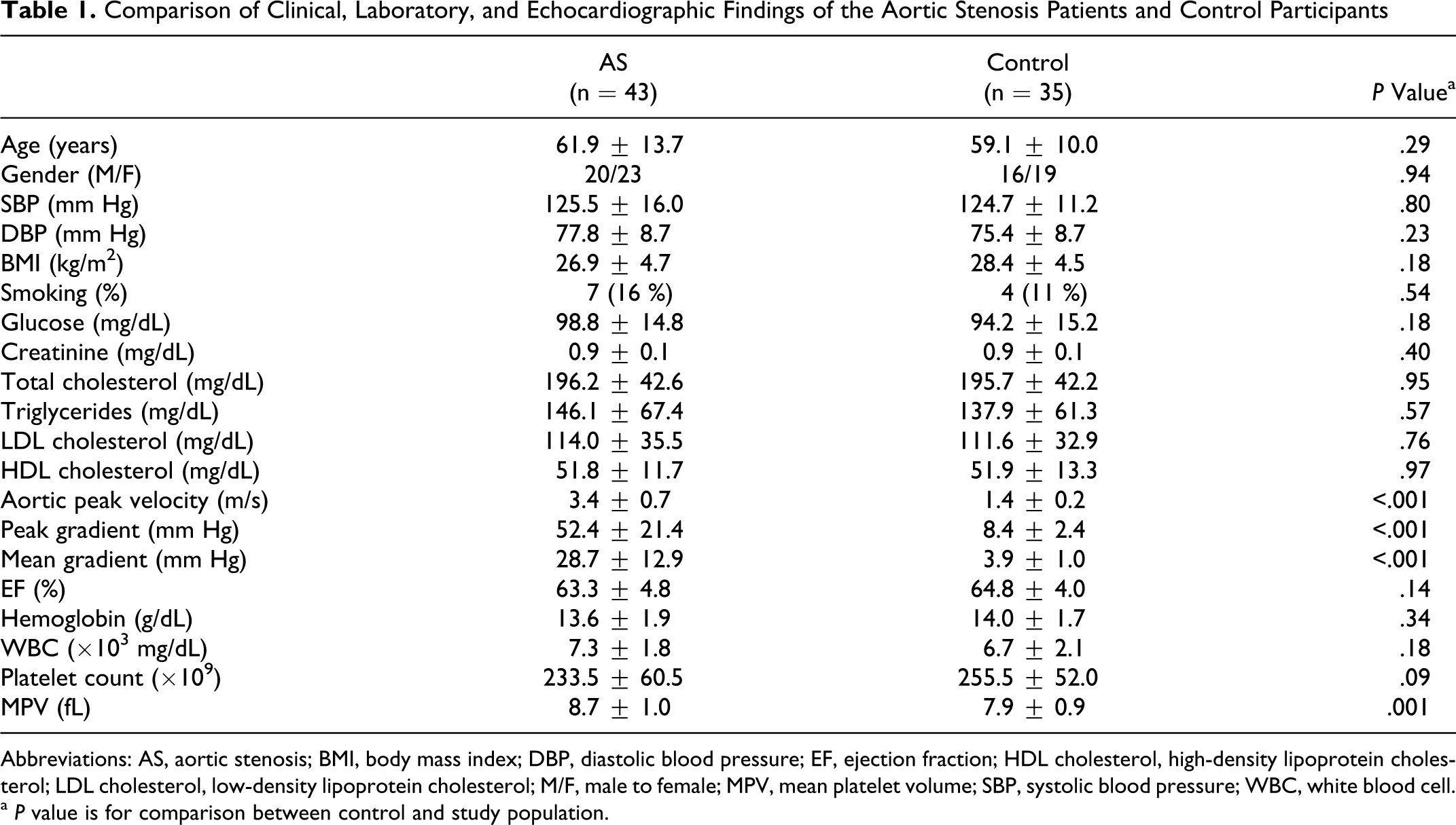
Abbreviations: AS, aortic stenosis; BMI, body mass index; DBP, diastolic blood pressure; EF, ejection fraction; HDL cholesterol, high-density lipoprotein cholesterol; LDL cholesterol, low-density lipoprotein cholesterol; M/F, male to female; MPV, mean platelet volume; SBP, systolic blood pressure; WBC, white blood cell.
a P value is for comparison between control and study population.
Discussion
In the current study, we examined MPV, an indicator of platelet activation in patients with AS. We found that MPV was significantly higher in patients with AS. To the best of our knowledge, there is no data about MPV in patients with AS.
Systemic thromboembolism is one of the important complications of AS. 1 Previous studies have demonstrated that platelet activation occurs in patients with AS.1–6 Chirkov et al demonstrated that AS, irrespective of the presence and/or absence of coronary artery disease, was associated with platelet hyperaggregability. 4 Dimitrow et al studied the markers of thrombin generation (thrombin–antithrombin complex, prothrombin fragment 1 + 2) and platelet activation (soluble CD40 ligand, β-thromboglobulin, P-selectin) in peripheral blood plasma. 5 They also assessed the extent of atherosclerosis in the carotid and coronary arteries as a potential confounding factor. They found that the mean concentrations of thrombin and platelet markers were higher in the AS group than in the controls, and atherosclerotic lesions detected in the coronary or carotid vessels were not associated with the variables studied.
Several studies have shown that shear stresses in turbulent flow as a result of stenotic valves induce platelet activation.7–10 Association between stenosis and platelet activation has been observed in other groups of valvular heart disease. It has been reported that MPV was higher in patients with mitral stenosis with sinus rhythm. 18 We have also shown that MPV was significantly elevated in patients with mitral stenosis who were in sinus rhythm compared to control participant. 19 The mitral valve stenosis represents a relatively low-gradient stenosis, whereas AS is a high-gradient valvular defect. This indicates that AS will generate even higher blood levels of platelet activation markers.
Mean platelet volume is a simple and easy method of assessing platelet function.11,12 Platelets are heterogeneous in size, density, and reactivity. In comparison to smaller ones, larger platelets have more granules, aggregate more rapidly with collagen, have higher thromboxane A2 level, and express more glycoprotein Ib and IIb/IIIa receptors.13–15 Because larger platelets are metabolically more active, platelet volume may be one of the determinants of platelet function. Large platelets are more prone to adhesion and aggregation.
The increased MPV has been noted in a number of situations, such as smoking, 20 diabetes mellitus, 21 obesity, 22 hypertension, 23 and increased cholesterol. 24 However, there was no significant difference between AS patients and control group with respect to body mass index, systolic blood pressure, diastolic pressure, the percentages of smoking, and the levels of glucose and cholesterol in the current study. So we could say that MPV values were higher in patients with AS, regardless of these factors.
The reason for increased MPV in stenotic valvular heart disease is controversial. It is considered to be caused by platelet activation due to shear stresses in turbulent flow as a result of stenotic valves, together with other factors and the presence of circulating platelet activation stimulators. 25 Aortic valve sclerosis is characterized by fibrocalcification or thickening in aortic valve without causing significant narrowing and in which the pathology resembles atherosclerotic coronary heart disease. Recently, Sucu et al reported that platelet-production indices including MPV and platelet distribution weight (PDW) were increased in patients with aortic valve sclerosis. 26 Aortic valve fibrocalcification or thickening itself occurring in AS might also have a direct role in the increase of MPV apart from shear stresses in turbulent flow as a result of stenotic valve.
Our study has some limitations. First, the number of patients was small mostly due to numerous exclusion criteria. Second, our analysis was based on a simple baseline determination at single time point that may not reflect the patient status over long periods.
In conclusion, we have shown that MPV was significantly elevated in patients with AS compared to control participant. Because larger platelets are metabolically more active, MPV might be one of the determinants of platelet function and large platelets are more prone to adhesion and aggregation. Elevated MPV values may indicate that patients with AS have a higher risk of systemic thromboembolism due to increased platelet activation. We suggest that patients with high MPV values might benefit from antiplatelet therapy. Further prospective studies are mandatory to establish the pathophysiological and clinical significance of increased MPV in patients with AS.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.