
Abstract
Background
The ABCD-GENE (Age, Body Mass Index, Chronic Kidney Disease, Diabetes Mellitus, and Genotyping) score is a tool used to identify increased thrombotic risk in clopidogrel-treated patients. We evaluated the association between a low ABCD-GENE score (<10) and Bleeding Academic Research Consortium (BARC)-defined bleeding among prasugrel or ticagrelor and clopidogrel-treated patients.
Methods
This was an IRB-approved retrospective cohort study of patients who underwent percutaneous coronary intervention (PCI) and CYP2C19 genotyping. The primary outcome was time to first bleed of any severity within 1 year. Time to first major bleed, defined by BARC 3a, 3b, 3c, or 5 criteria, and major adverse cardiovascular events (MACE) were secondary outcomes. BARC bleeding events were compared between prasugrel or ticagrelor and clopidogrel-treated patients and stratified by the ABCD-GENE score threshold of ≥10. Kaplan-Meier and multivariable Cox proportional hazards model were used for time-to-event analyses.
Results
Of 2547 patients, 1760 were in the low score group, and 787 were in the high score group. Kaplan-Meier analysis showed that any bleeding (P = .008) and major bleeding (P = .015) were less for those with a low score compared to a high score. Among those in the low score group, any bleeding (P < .001) and major bleeding (P = .022) were lower with clopidogrel versus prasugrel or ticagrelor. However, the ABCD-GENE score was not independently associated with bleeding in the Cox model. No difference in MACE was observed by treatment in the low score group.
Conclusions
The ABCD-GENE score was associated with BARC bleeding, yet other variables had a greater impact such as history of GI bleed, anticoagulation, P2Y12 inhibitor, and age. Patients with a low score who received prasugrel or ticagrelor had more bleeding versus clopidogrel. Our findings support further evaluation of the ABCD-GENE score as a tool for guided P2Y12 inhibitor de-escalation post-PCI.
Introduction
Optimizing antiplatelet therapy post-percutaneous coronary intervention (PCI) can be challenging since factors associated with thrombosis and bleeding may both be present. 1 Precision medicine approaches with antiplatelet therapy can help to improve the risk-benefit tradeoff between safety and effectiveness.2,3 Genetic variability in the CYP2C19 gene explains part of the diminished clopidogrel response seen in some patients.4,5 However, it is important to also consider other factors that affect pharmacodynamics. 6 ABCD-GENE (Age, Body Mass Index, Chronic Kidney Disease, Diabetes Mellitus, and Genotyping) is a score that integrates these variables to provide improved accuracy in predicting high platelet reactivity (HPR) versus their individual components. 7 A 2024 consensus statement on platelet function and genetic testing in PCI advises that integrating clinical variables with genetic data should be considered to increase the accuracy in predicting HPR in clopidogrel-treated patients. 8 For example, in the acute coronary syndrome (ACS) population at high bleeding and ischemic risk, a guided approach leading to selective de-escalation among clopidogrel responders can be considered to reduce bleeding risk without a tradeoff in efficacy. 8
In previous studies, bleeding was not predicted by ABCD-GENE based on conventional definitions such as the Global Use of Strategies to Open Occluded Arteries (GUSTO), which evaluated moderate, severe, or life-threatening bleed events.7,9,10 Understanding whether ABCD-GENE can predict bleeding as assessed by the Bleeding Academic Research Consortium (BARC) score would further its value in guiding de-escalation. 11 This becomes especially important considering that clopidogrel is more affordable and better tolerated than prasugrel or ticagrelor, particularly in the elderly population.12,13 Therefore, we leveraged among the largest cohorts of CYP2C19-genotyped PCI patients in the United States and sought to explore potential associations between the ABCD-GENE score and BARC bleeding. We specifically aimed to evaluate those patients with a low ABCD-GENE score (<10) and the impact on bleeding between treatment with prasugrel or ticagrelor and clopidogrel.
Methods
Study Design and Participants
We conducted a retrospective, single-center, cohort study of adult patients who underwent PCI between December 2015 and October 2020 and who were followed for 1-year post-index visit. Patients had a CYP2C19 genotype test result reported in the electronic health record (EHR). Excluded patients had a liver or allogeneic stem cell transplant before or during the study period, or if P2Y12 inhibitor therapy at the time of the primary outcome was not documented. This study was part of our PreCISE-Rx (Pharmacogenomics-guided Care to Improve the Safety and Effectiveness of Medications) program. 14 The study adhered to the principles of the Declaration of Helsinki and was approved by the institutional review board of the University of Pittsburgh with waiver of informed consent.
Pharmacogenomics Service
Our institution's post-PCI order set and pathway includes an opt-out CYP2C19 genotyping to help guide P2Y12 inhibitor selection. The laboratory assay (GenMark Diagnostics, Carlsbad, CA) detects CYP2C19 *2, *3, *4, *5, *6, *7, *8, *9, *10, and *17 and returns the diplotype and the interpretation as a genetically predicted phenotype (ie, CYP2C19 Poor Metabolizer) to the EHR. A clinical pharmacist provides a recommendation documented in the EHR for P2Y12 inhibitor selection that considers both genetic and clinical factors. Recommendations are provided for both escalation and de-escalation of P2Y12 inhibitor based on the presence of a loss of function (LOF) allele, defined as either decreased function (DF) or no function (NF), and when clinically appropriate based on Clinical Pharmacogenetic Implementation Consortium (CPIC) guidelines.8,15 However, the ultimate prescribing decision was based upon the provider's discretion.
Data Collection
Retrospective data collection was managed with the use of a secure, web-based software that supports data capture with audit trails for data tracking, automated export processes, and interoperability with external sources [Research Electronic Data Capture (REDCap®), Nashville, TN].16,17 A trained research nurse collected baseline and follow-up data for all patients.
Data collection at baseline included: demographic, clinical, procedural, laboratory, and genetic variables. We captured P2Y12 inhibitor use prior to admission, during PCI, at discharge, and with each clinic or inpatient hospital visit during the study period. Follow-up visits were defined as inpatient or outpatient encounters during which there was a patient evaluation with a healthcare professional. Therefore, clinical outcomes and medication changes could be recorded.
Clinical Assessment
The primary outcome was time to first bleed of any severity within 1 year of the index PCI. The time to first major bleed, defined by BARC 3a, 3b, 3c, or 5 criteria, was a secondary outcome. BARC 1 includes non-actionable bleeding that does not cause the patient to seek medical care for the bleed. BARC 2 is actionable bleeding that causes non-surgical intervention, hospitalization, or further evaluation. BARC 3a, 3b, 3c and 5 encompassed major bleeding. BARC 3a includes a hemoglobin drop between 3 and <5 g/dL or need for transfusion. BARC 3b includes any surgical intervention to control bleeding, use of vasoactive agents, or a hemoglobin drop of >5 g/dL. BARC 3c includes intracranial hemorrhage or intraocular bleed compromising vision. BARC 5 is death due to bleeding. BARC 4, coronary artery bypass graft-related bleeding, was excluded from our study analysis. 11 Additionally, bleeding events secondary to trauma were excluded from our analysis. Major adverse cardiovascular events (MACE) defined as all-cause mortality, myocardial infarction, or ischemic stroke was also a secondary outcome.
For clinical outcomes, patients were censored when lost to follow-up or if they discontinued the P2Y12 inhibitor. Treatment assignment was based on P2Y12 inhibitor use on the event or censor date. CYP2C19 genotypes were grouped into patients who were LOF allele carriers (CYP2C19 Poor Metabolizers/Likely Poor Metabolizers or Intermediate Metabolizers/Likely Intermediate Metabolizers) and those who were not LOF allele carriers (CYP2C19 Normal, Rapid, and Ultra-rapid Metabolizers).
Data Analysis
The ABCD-GENE score was calculated from patient-specific variables at index PCI. Clinical factors included: age >75 years (+4 points), body mass index >30 kg/m2 (+4 points), chronic kidney disease with estimated glomerular filtration rate <60 mL/min/1.73 m2 determined from the chronic kidney disease (CKD)-EPI equation (+3 points), and diabetes mellitus (+3 points). Genetic factors included: 1 (+6 points) or 2 (+24 points) CYP2C19 LOF alleles.7,18 Baseline characteristics were compared between prasugrel or ticagrelor and clopidogrel-treated patients across ABCD-GENE score strata. The individual components of the ABCD-GENE score were also reported between the P2Y12 inhibitor groups.
The primary analysis compared any BARC bleeding between prasugrel or ticagrelor and clopidogrel-treated patients stratified by the ABCD-GENE score threshold of ≥10. Secondary analyses included BARC major bleeding and MACE between prasugrel or ticagrelor and clopidogrel groups by ABCD-GENE score. Univariate analyses of associations between the ABCD-GENE strata (≥10 vs <10) and bleeding were also reported. A Kaplan-Meier analysis and multivariable Cox proportional hazards model were used for unadjusted and covariate-adjusted time-to-event analyses, respectively. Covariates considered for the Cox model included: ABCD-GENE score (high vs low), age, history of gastrointestinal bleeding, concomitant anticoagulation therapy prior to index PCI, P2Y12 inhibitor (prasugrel or ticagrelor vs clopidogrel), history of intracranial hemorrhage (ICH), and PCI indication (ACS vs non-ACS). The covariates used in the Cox regression model were based on those described in a previous study by our group. 14 We also conducted Kaplan-Meier analyses for our bleeding definitions, and for the subgroup of those with a low ABCD-GENE score, after exclusion of patients who received post-PCI anticoagulation. A log-rank test was used to test equality of survivor functions between treatment groups in unadjusted analyses. A univariate Cox regression was used to generate unadjusted hazard ratios (HRs). Adjusted hazard ratios (aHRs) were reported for differences between treatment groups in the multivariable Cox proportional hazards model. Differences in discontinuation rates were compared using Chi-square or Fisher's exact tests, as appropriate. All data pre-processing and statistical analyses were conducted through the COMPASS platform. [Compass v1.28.0, Cipherome Inc. (2025), Computer software, https://compass.cipherome.com/].
Results
Patient Characteristics
The characteristics and demographics of the 2547 patients included in the study are shown in Table 1. Patients were split into 2 groups, those with an ABCD-GENE score < 10 (n = 1760) and those with an ABCD-GENE score ≥ 10 (n = 787). Within those groups, patients were treated with either clopidogrel or prasugrel or ticagrelor. Many of the patients were middle age, White males with atrial fibrillation, heart failure, hypertension, and diabetes as the most common medical conditions. Many patients also presented with ACS as the indication for PCI and received drug-eluting stents.
Baseline Demographic and Clinical Characteristics.

Values are median (Q1-Q3) or n (%). Baseline variables compared between P2Y12 inhibitor groups (ALT vs clopidogrel) for each score stratum (ABCD-GENE scores <10 and ≥10) using the Student's t-test, Mann-Whitney U, or chi-square test as appropriate. SI conversion factors: To convert serum creatinine to milligrams per liter, multiply by 10; hemoglobin to grams per liter, multiply by 10. ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; BMS, bare-metal stent; CAD, coronary artery disease; DES, drug-eluting stent; eGFR, estimated glomerular filtration rate; GI, gastrointestinal; Hb, hemoglobin; Hct, hematocrit; ICH, intracranial hemorrhage; MI, myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; PPI, proton pump inhibitor; Scr, serum creatinine; STEMI, ST-segment-elevation myocardial infarction.
The individual components of the ABCD-GENE score for both groups are detailed in Table 2. Within the ABCD-GENE score < 10 group, the median score was 4, with a total of 104 patients (18.1%) who had 2 LOF alleles treated with prasugrel or ticagrelor. No patients with 2 LOF alleles received clopidogrel. A total of 598 patients had 1 LOF allele; 470 (81.9%) received prasugrel or ticagrelor and 128 (10.8%) were treated with clopidogrel. Within the ABCD-GENE score ≥ 10 group, patients treated with prasugrel or ticagrelor had a median score of 12 and those treated with clopidogrel had a median score of 11. In these groups, a total of 165 patients (71.2%) had 2 LOF alleles and 340 patients (72.2%) had at least 1 LOF allele. The majority of patients (64.8%) with 2 LOF alleles received prasugrel or ticagrelor, however, a relatively low proportion of patients (21.9%) with 1 LOF allele received prasugrel or ticagrelor.
ABCD-GENE Score and Individual Components.
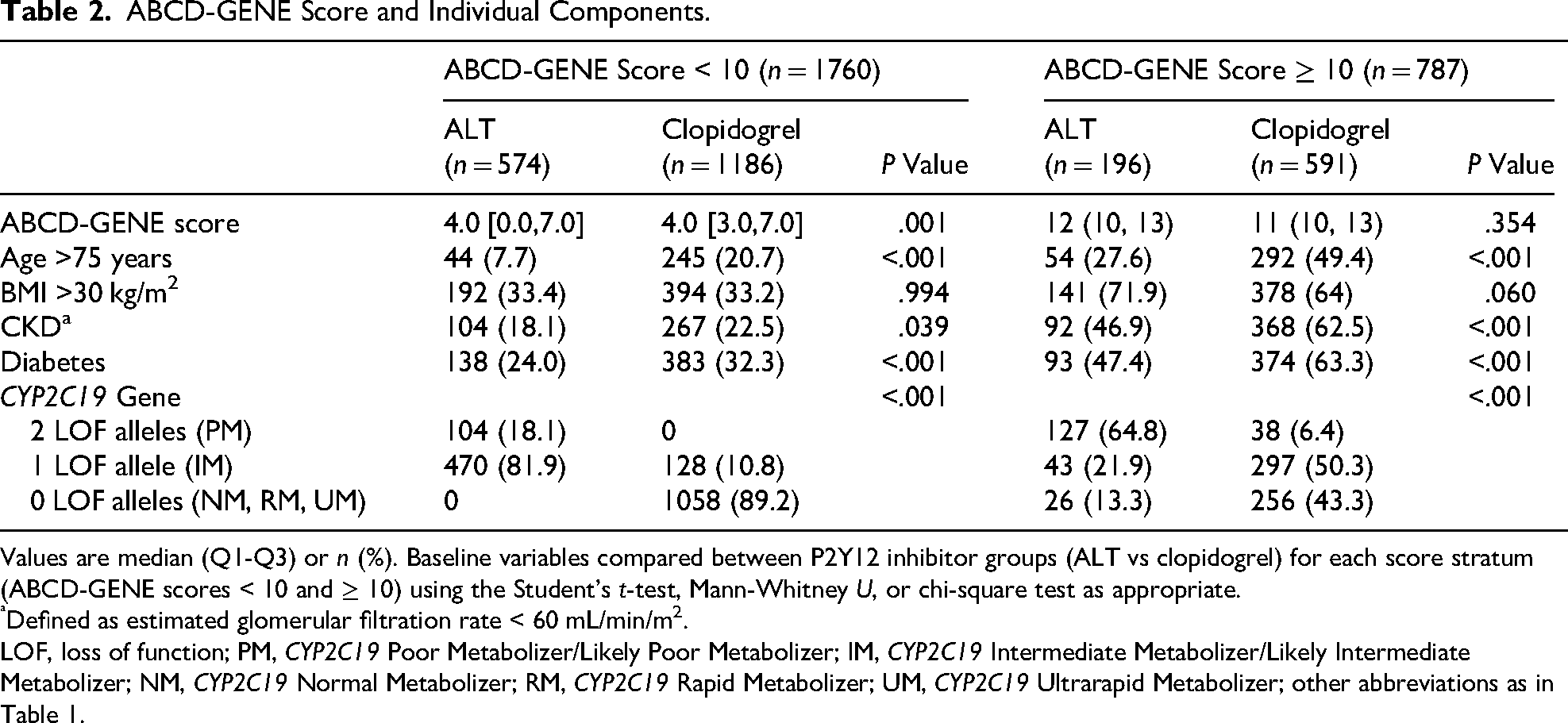
Values are median (Q1-Q3) or n (%). Baseline variables compared between P2Y12 inhibitor groups (ALT vs clopidogrel) for each score stratum (ABCD-GENE scores < 10 and ≥ 10) using the Student's t-test, Mann-Whitney U, or chi-square test as appropriate.
Defined as estimated glomerular filtration rate < 60 mL/min/m2.
LOF, loss of function; PM, CYP2C19 Poor Metabolizer/Likely Poor Metabolizer; IM, CYP2C19 Intermediate Metabolizer/Likely Intermediate Metabolizer; NM, CYP2C19 Normal Metabolizer; RM, CYP2C19 Rapid Metabolizer; UM, CYP2C19 Ultrarapid Metabolizer; other abbreviations as in Table 1.
Clinical Outcomes
Association of ABCD-GENE with Bleeding at 1-Year After PCI
The results of the primary outcome of time to first bleed of any severity within 1 year of PCI are depicted in Table 3. More patients experienced any bleeding in the ABCD-GENE high score group compared to the low score group (41% vs 36.5%; P = .034). The results of the secondary outcome of time to first major bleed are depicted in Table 4. More patients also experienced major bleeding in the high score versus low score group (17.7% vs 14.8%), however, this difference was not significant (P = .073). Among the subgroup of patients who received an oral anticoagulant at discharge, any bleeding was more frequent compared to those who did not receive an anticoagulant post-PCI (56.8% vs 32.5%). Additionally, major bleeding was more frequent in those on an anticoagulant post-PCI versus without (25.5% vs 12.7%).
Association of ABCD-GENE Score With Any Bleeding at 1-Year After PCI.
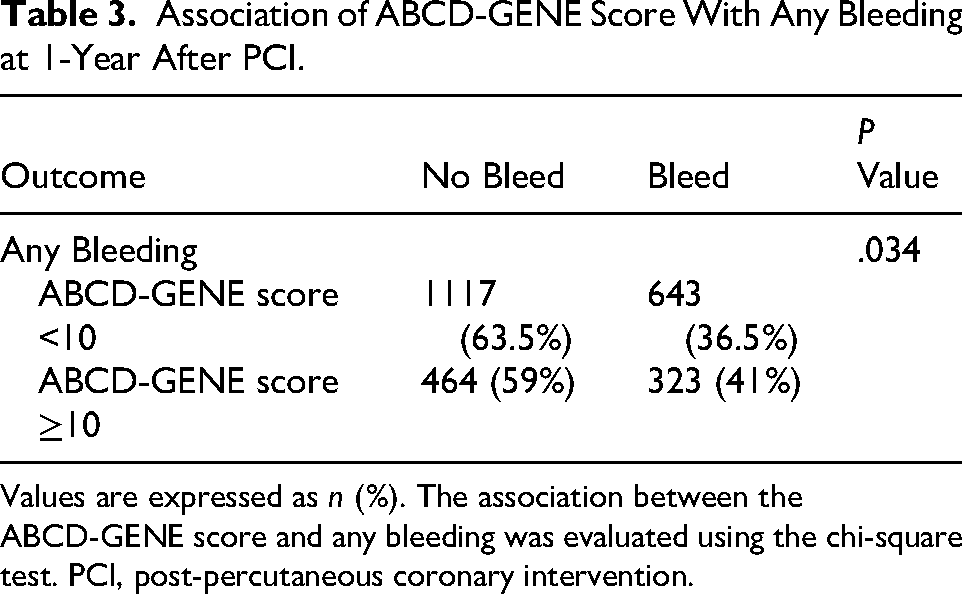
Values are expressed as n (%). The association between the ABCD-GENE score and any bleeding was evaluated using the chi-square test. PCI, post-percutaneous coronary intervention.
Association of ABCD-GENE Score With Major Bleeding at 1-Year After PCI.
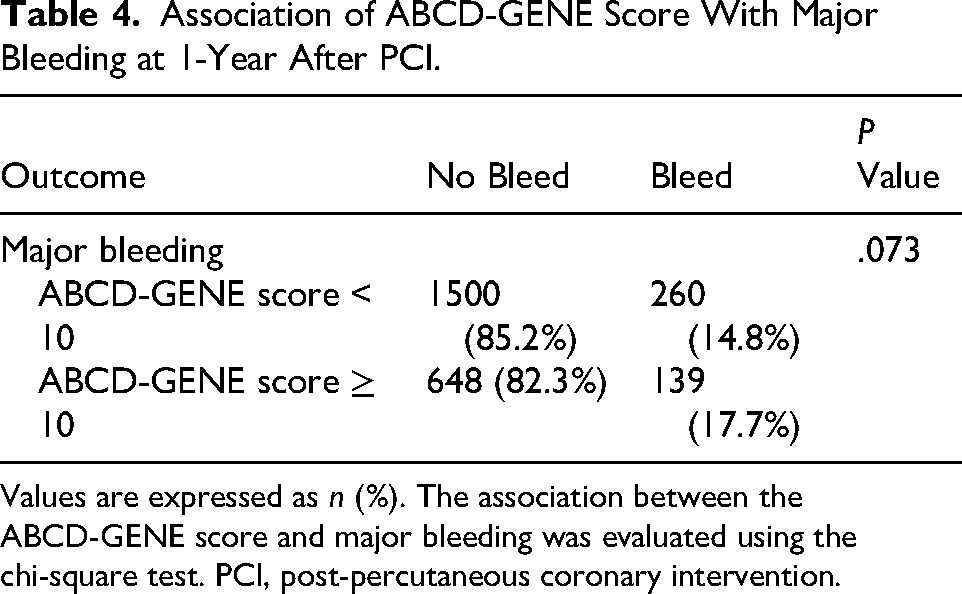
Values are expressed as n (%). The association between the ABCD-GENE score and major bleeding was evaluated using the chi-square test. PCI, post-percutaneous coronary intervention.
Figures 1 and 2 show the Kaplan-Meier curve stratified by ABCD-GENE score for any bleeding and major bleeding, respectively. The probability of any bleeding events was lower in the ABCD-GENE score <10 group versus the ABCD-GENE score ≥ 10 group (P = .008). Cox proportional hazards model of covariates were ABCD-GENE score (aHR 1.02, 95% CI 0.89-1.17, P = .74), age (aHR 1.02, 95% CI 1.02-1.03, P < .001), history of GI bleeding (aHR 1.94, 95% CI 1.56-2.41, P < .001), anticoagulation prior to index visit (aHR 1.60, 95% CI 1.35-1.90, P < .001), P2Y12 inhibitor (aHR 1.82, 95% CI 1.58-2.09, P < .001), history of ICH (aHR 1.15, 95% CI 0.75-1.76, P = .52), and PCI indication (aHR 0.80, 95% CI 0.70-0.91, P < .001).
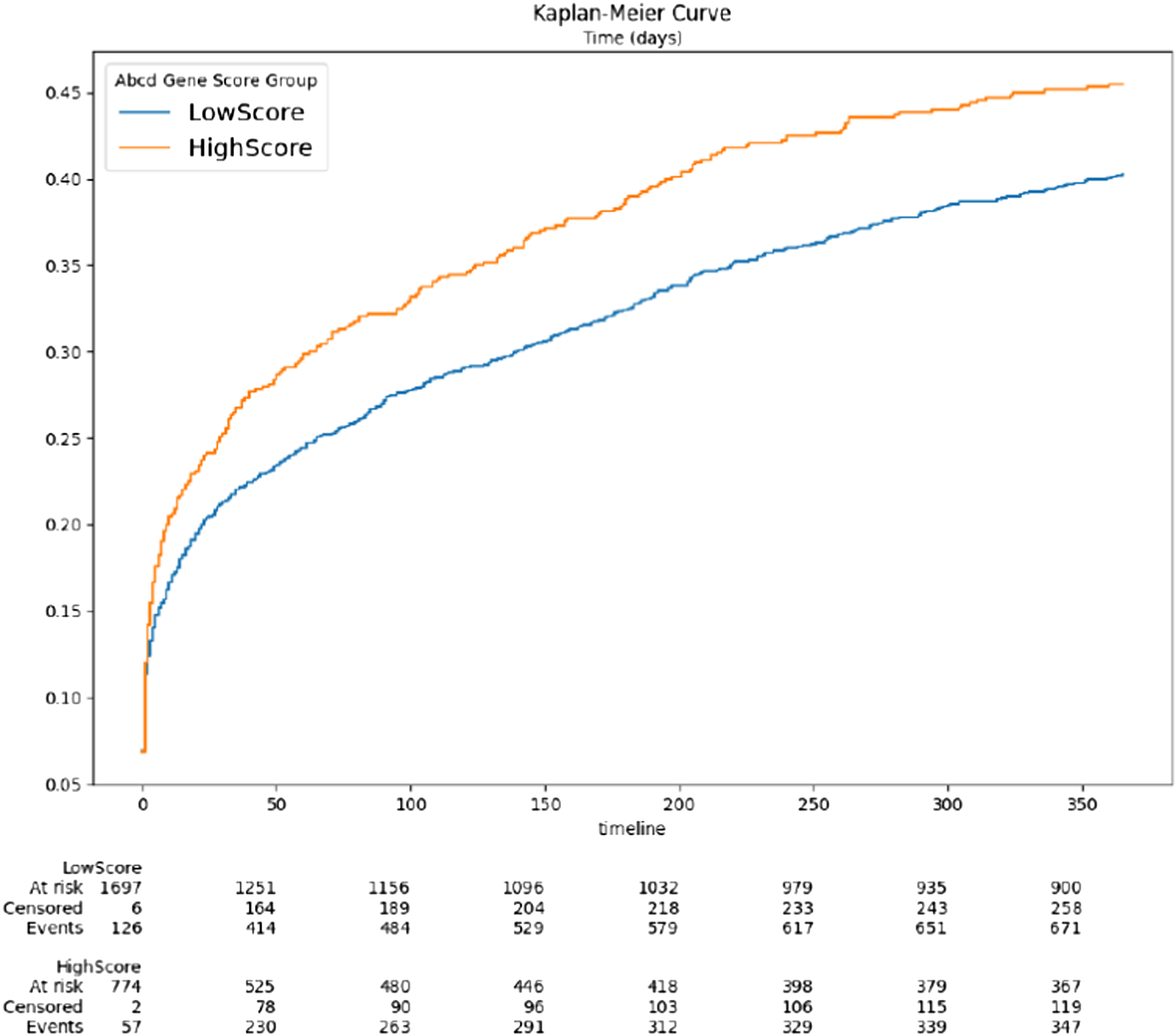
Kaplan-Meier curve of any bleeding stratified by ABCD-GENE score.

Kaplan-Meier curve of major bleeding stratified by ABCD-GENE score.
The probability of major bleeding was also lower in patients with an ABCD-GENE score <10 (P = .015). Cox proportional hazards model of covariates were ABCD-GENE score (aHR 1.04, 95% CI 0.84-1.28, P = .72), age (aHR 1.02, 95% CI 1.01-1.03, P = .001), history of GI bleeding (aHR 3.10, 95% CI 2.33-4.12, P < .001), anticoagulation prior to index visit (aHR 1.65, 95% CI 1.27-2.13, P = .001), P2Y12 inhibitor (aHR 1.75, 95% CI 1.40-2.17, P < .001), history of ICH (aHR 1.37, 95% CI 0.75-2.50, P = .31), and PCI indication (aHR 0.87, 95% CI 0.71-1.07, P = .20). After excluding patients who received post-PCI anticoagulation, we found that both any bleeding and major bleeding remained significantly higher in the ABCD-GENE high score group (Supplemental Figures 1 and 2).
In Figure 3, the Kaplan-Meier curves for any bleeding in patients with low ABCD-GENE score stratified by treatment showed that events were lower in those treated with clopidogrel versus prasugrel or ticagrelor (P < .001). Cox proportional hazards model of covariates were P2Y12 inhibitor (aHR 1.90, 95% CI 1.60-2.25, P < .001), age (aHR 1.02, 95% CI 1.01-1.03, P < .001), history of GI bleeding (aHR 2.00, 95% CI 1.50-2.65, P < .001), history of ICH (aHR 1.05, 95% CI 0.61-1.83, P = .85), anticoagulation prior to index visit (aHR 1.64, 95% CI 1.31-2.04, P < .001), and PCI indication (aHR 0.75, 95% CI 0.64-0.89, P < .001).

Kaplan-Meier curve of any bleeding with low ABCD-GENE score stratified by treatment.
Similarly, the Kaplan-Meier curve for major bleeding with low ABCD-GENE score stratified by treatment, depicted in Figure 4, showed that event rates were significantly lower among the patients treated with clopidogrel (P = .022). Cox proportional hazards model of covariates were P2Y12 inhibitor (aHR 1.72, 95% CI 1.32-2.26, P < .001), age (aHR 1.02, 95% CI 1.01-1.03, P = .004), history of GI bleeding (aHR 3.34, 95% CI 2.32-4.80, P < .001), history of ICH (aHR 1.26, 95% CI 0.59-2.69, P = .56), anticoagulation prior to index visit (aHR 1.65, 95% CI 1.18-2.31, P = .003), and PCI indication (aHR 0.84, 95% CI 0.65-1.08, P = .17). After excluding patients who received post-PCI anticoagulation, we found that any bleeding remained significantly higher with prasugrel or ticagrelor in the low ABCD-GENE score group. However, major bleeding did not differ between treatment groups in the low score group (Supplemental Figures 3 and 4). Finally, in Figure 5 the Kaplan-Meier curve showed that there was no difference in MACE among patients with low ABCD-GENE score stratified by treatment (P = .639).
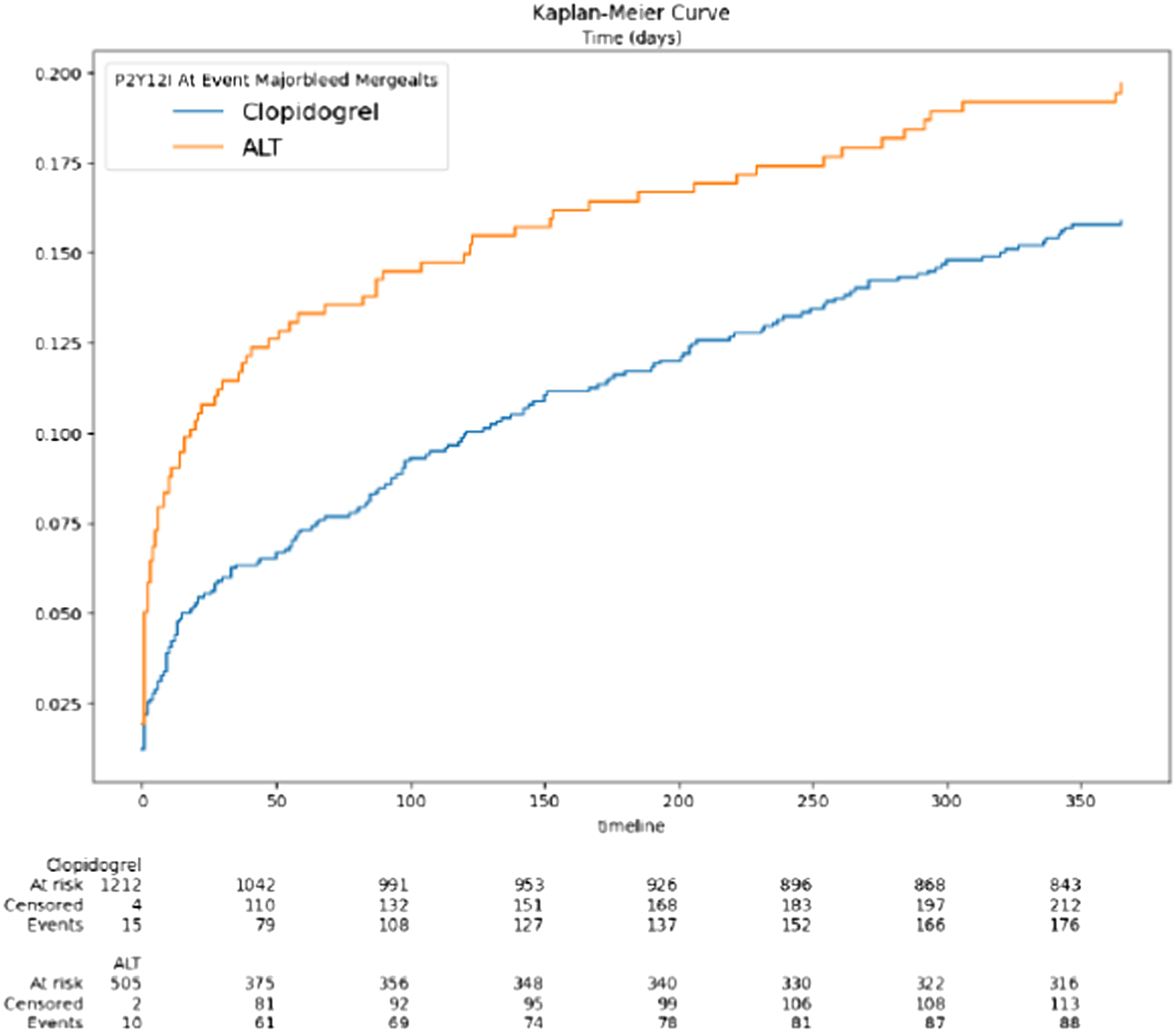
Kaplan-Meier curve of major bleeding with low ABCD-GENE score stratified by treatment.
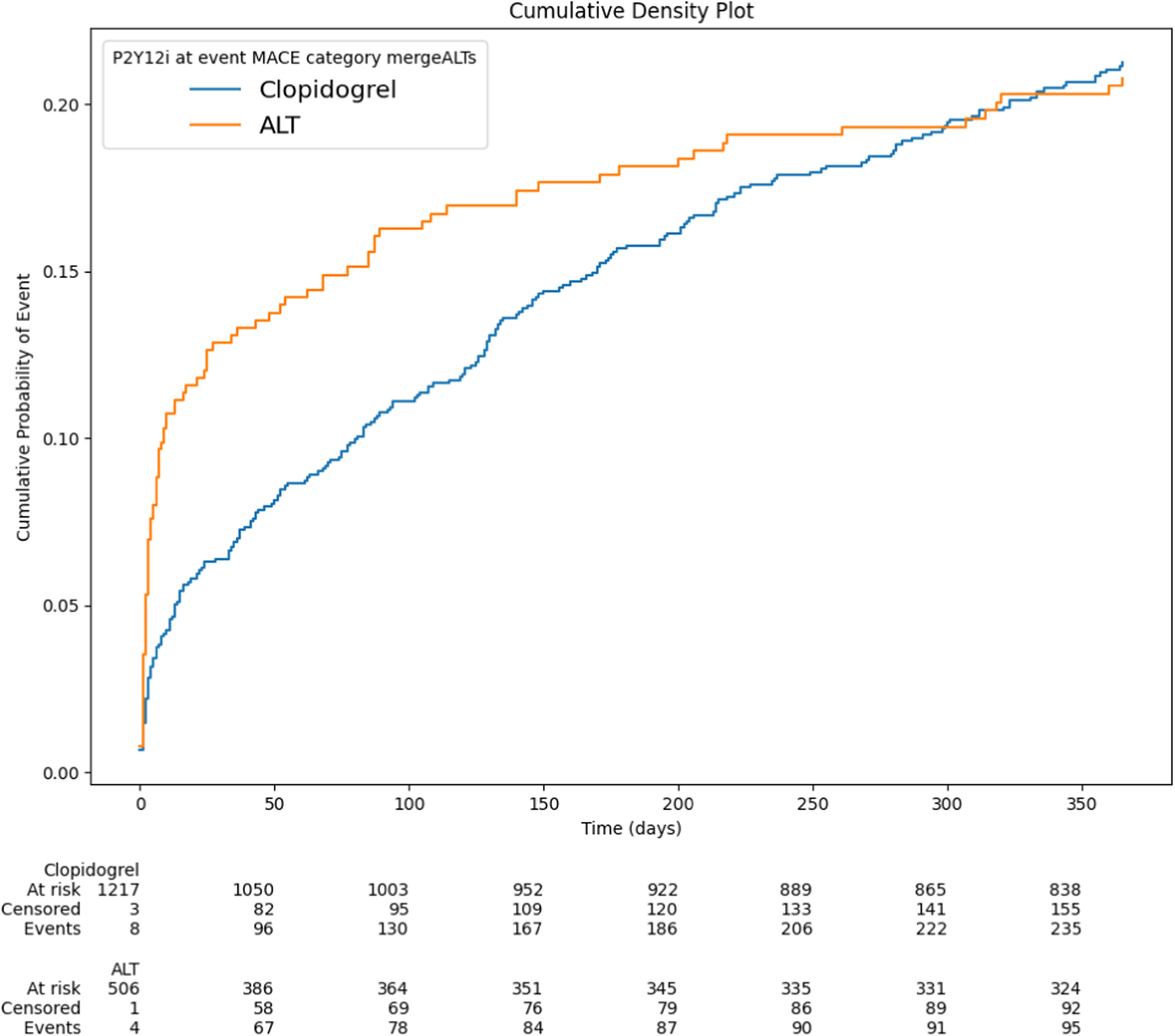
Kaplan-Meier curve of MACE with low ABCD-GENE score stratified by treatment.
We conducted an exploratory analysis of bleeding based on BARC type. BARC 1 represented 46.5% of all bleeding events, followed by BARC 2 (40.2%), BARC 3 (12.9%), and BARC 5 (0.4%). A sensitivity analysis showed the impact of each type of bleeding on the overall outcomes: BARC 1 (aHR 2.07 [95% CI, 1.69-2.52]; P < .001), BARC 1 or 2 (aHR 1.89 [95% CI 1.59-2.25]; P < .001, BARC 2, 3, or 5 (aHR 1.43 [95% CI 1.17-1.75]; P < .001) and BARC 3 or 5 (aHR 1.59 [95% CI 1.10-2.30]; P = .015).
Discussion
In this large, real-world study of patients who underwent PCI and were genotyped for CYP2C19, we demonstrated that the ABCD-GENE score was associated with any bleeding but not major bleeding based on univariate analyses. Having a high score was associated with more bleeding (any and major) based on Kaplan-Meier analysis, however, it was not significant when analyzed via the Cox model. This discordance may be explained by the fact that other variables in our model had a larger impact on bleeding, such as the use of prasugrel or ticagrelor, history of GI bleeding, pre-PCI anticoagulation, and age. Conversely, ACS indication was associated with a lower likelihood of bleeding. Previous studies did not show a significant association between ABCD-GENE and bleeding, although the definitions used relied on more historical definitions that captured larger bleeds.7,9,19 We used the more contemporary BARC definition and showed that nuisance (BARC 1) and minor (BARC 1 or 2) bleeding were the most common and had the greatest impact on the bleeding outcomes in the study. However, other bleeding types such as clinically relevant (BARC 2, 3, or 5) and major (BARC 3 or 5) bleeding also had significant, albeit attenuated, associations with the overall bleeding outcomes.
A clinically relevant observation from our study is that patients with a low ABCD-GENE score had significantly more bleeding (any and major) with prasugrel or ticagrelor versus clopidogrel. Approximately 70% of our study population had a low score, yet more than 30% received prasugrel or ticagrelor therapy. Within this cohort, we found no difference in MACE. These observations bolster the clinical argument to de-escalate therapy in patients with a low ABCD-GENE score who are receiving prasugrel or ticagrelor with the goal to lower bleeding risk.3,8 Figure 6 shows the potential utility of ABCD-GENE and our key findings within the context of a proposed clinical pathway. Our results are supported by an analysis of ACS registry patients from the Netherlands that compared genotype-guided de-escalation to standard care (predominant ticagrelor use). The authors found that BARC bleeding (2, 3, or 5) was approximately 30% lower in the genotype-guided group without a difference in ischemic events versus standard care. 20
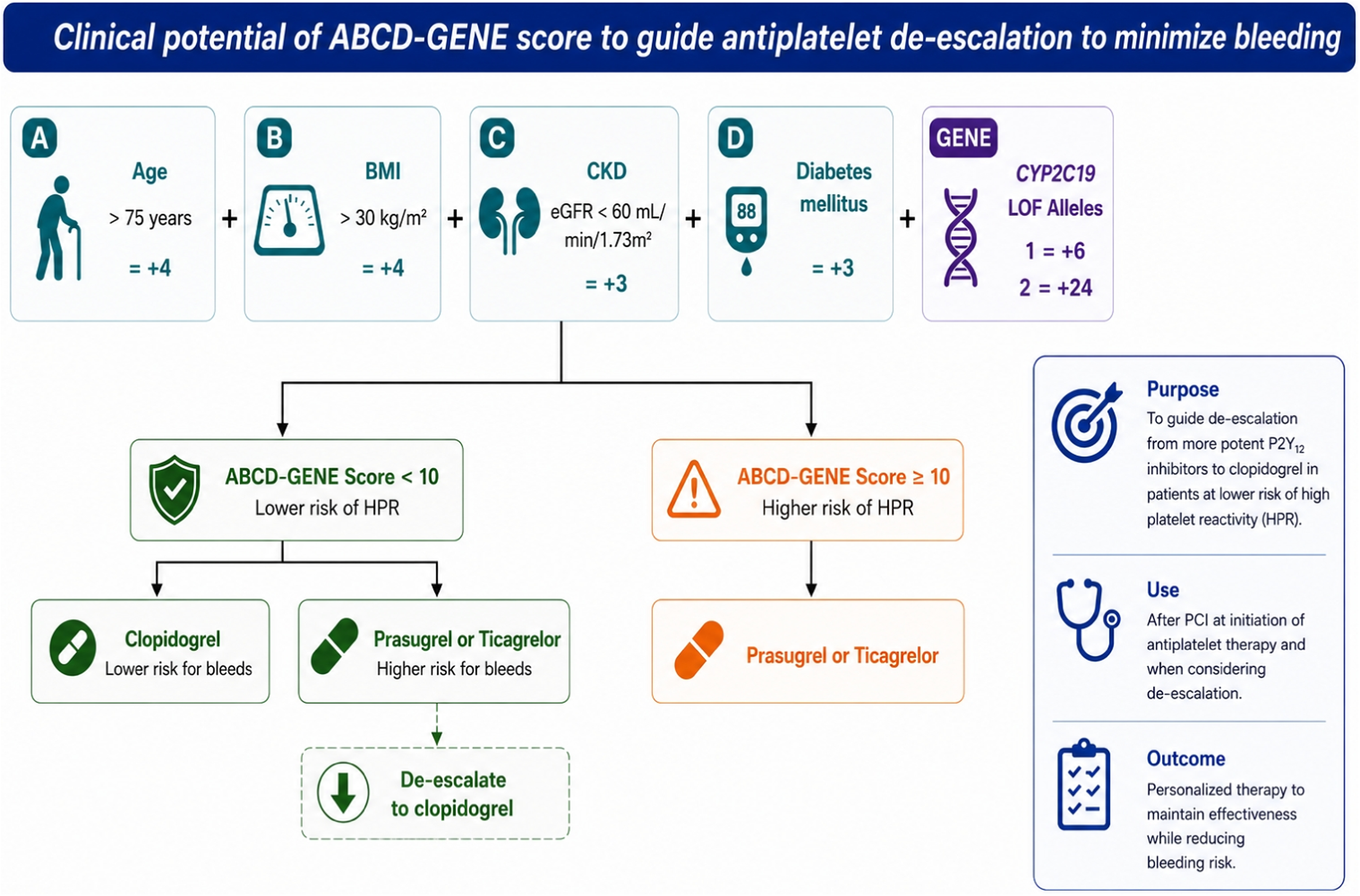
Clinical potential of ABCD-GENE score to guide antiplatelet de-escalation to minimize bleeding. BMI, body mass index; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; LOF, loss-of-function; HPR, high on-treatment platelet reactivity; PCI, percutaneous coronary intervention.
ABCD-GENE was previously shown to identify patients in whom clopidogrel should be avoided on the basis of having HPR and increased risk for MACE with a higher score (≥10). 7 Its use was further validated in a real-world setting by demonstrating that a higher score was associated with increased atherothrombotic risk among clopidogrel-treated patients. 19 In a separate analysis, atherothrombotic events did not differ between clopidogrel versus prasugrel or ticagrelor regardless of ABCD-GENE score. However, event rates appeared to be lower among those with prasugrel or ticagrelor and CYP2C19 LOF allele carriers regardless of score. Additionally, outcomes did not differ between clopidogrel and prasugrel or ticagrelor in non-LOF allele patients with low ABCD-GENE scores (<10). 9 Our findings add further support to these observations for using a guided de-escalation approach in patients receiving prasugrel or ticagrelor with a low ABCD-GENE score.
The strengths of our study include the fact that we had among the largest populations of PCI-treated patients at a single center who were genotyped for CYP2C19 metabolizer status, and in whom we were able to calculate the ABCD-GENE score. Our study methods included manual data curation which enabled the identification of BARC bleeding. 11 This definition is more contemporary and captures minor and nuisance bleeds, which carry prognostic significance even though they would have been missed using historical bleed definitions.11,21
Study Limitations
The observational nature of this study limited our ability to control for all potential confounders. Decisions about antiplatelet prescribing were left to the individual prescriber, however, recommendations about therapy from our clinical pharmacogenomics service were provided. We acknowledge the imbalance between groups at baseline, including a greater prevalence of ACS and a lower proportion of older patients, concomitant anticoagulation use, and cardiovascular comorbidities in the prasugrel or ticagrelor group. To account for PCI indication as a potential confounder, we evaluated whether or not the patient had ACS in our Cox regression model. We found that ACS was associated with a lower risk of any bleeding in the overall cohort and within the subgroup of those with a low ABCD-GENE score.
Given the biases and the potential for other residual confounders that we could not fully account for, we acknowledge external validity as a limitation from our single-center health system experience. While we were able to capture all encounters within our large integrated care delivery network (45 hospitals), it was not possible to collect all visits that may have occurred at external facilities. We determined variables of interest likely to affect P2Y12 inhibitor selection and bleeding outcome (ie, age, anticoagulation, history of bleeding) and accounted for these in our analyses. While pre-procedure anticoagulation was evaluated in our Cox model, we were unable to ascertain the duration of dual or triple antithrombotic therapy post-discharge. As an exploratory endpoint, we excluded those patients who received post-PCI anticoagulation and found that bleeding remained higher in the ABCD-GENE high score group based on Kaplan-Meier. However, other confounders may have been unaccounted for or were unavailable. Data collection also relied on documentation within the EHR to capture patient encounters, medications, and clinical outcomes post-PCI. Platelet function testing is another tool that could be considered for P2Y12 inhibitor selection; however, this was not collected in our study because it was rarely performed in our practice. Finally, the ABCD-GENE score determination and evaluation for association with bleeding outcomes was conducted retrospectively. Therefore, it was not integrated into clinical decision-making during the patient's index PCI.
Conclusion
The ABCD-GENE score was associated with BARC bleeding, yet other clinical variables had a greater impact in our study such as history of GI bleeding, anticoagulation, P2Y12 inhibitor, and age. Patients with a low score who received prasugrel or ticagrelor had significantly more bleeding compared to clopidogrel. Our observations support further evaluation of the ABCD-GENE score as a tool for guided P2Y12 inhibitor de-escalation post-PCI.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484261457268 - Supplemental material for ABCD-GENE Score and Bleeding in Post-PCI Patients: Implications for Guided De-Escalation of Antiplatelet Therapy
Supplemental material, sj-docx-1-cpt-10.1177_10742484261457268 for ABCD-GENE Score and Bleeding in Post-PCI Patients: Implications for Guided De-Escalation of Antiplatelet Therapy by James C. Coons, PharmD, FCCP, FACC, BCCP, Kathleen Polkowski, PharmD, Linda Prebehalla, BSN, RN, Anson Conrad Smith, MD, and Philip E. Empey, PharmD, PhD in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Author Note
These authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Acknowledgments
We acknowledge Younggyun Lim, PhD, for his expertise and contributions to data analysis and management.
Funding
The authors disclosed receipt of the following financial support for the research of this article: This work was supported by grants from the American Society of Health System Pharmacists; American Heart Association [17MCPRP33400175]; National Institutes of Health [UL1TR001857]; and an anonymous nonprofit organization.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.