
Abstract
Background:
Limited data are available regarding real-world prescribing in patients with an indication for oral anticoagulation (OAT) who undergo percutaneous coronary intervention (PCI). Most current guidelines recommend a period of triple therapy with OAT and dual antiplatelet (DAPT) agents over dual therapy with an OAT and DAPT but the clinical benefit is still unclear giving rise to limited evidence-based recommendations.
Aim:
To analyze the appropriateness of OAT and anti-platelet strategies post PCI in a real-world cohort of patients in 2 academic teaching hospitals.
Methods and Results:
In total, 103 patients were retrospectively analyzed. As the initial 3 month stragey, 97 patients (94.2%) received triple therapy, 4 received Dual Therapy (3.9%) and 2 received DAPT (1.9%). Patients with predominant bleeding risk were significantly less likely to receive triple therapy (75% vs. 95.7% vs. 95.8%, P < 0.05). Apixaban was the most common OAT (65.7%) which in most cases was prescribed at an inappropriately reduced dose of 2.5 mg BD (80.4%). The MACE, bleeding and all-cause mortality rates did not differ significantly between groups.
Discussion:
Our study demonstrates the widespread use of triple therapy for the first 3 months of treatment in 2 Irish academic hospitals. DOACs were prescribed in most cases at reduced doses not currently known to prevent stroke. This study highlights the need for more explicit management algorithms to improve evidence-based management in this area.
Introduction
It is estimated that 10% of patients undergoing percutaneous coronary intervention (PCI) have a concurrent indication for oral anticoagulation therapy (OAT), predominantly atrial fibrillation. 1 This presents a clinical dilemma where the physician must balance the bleeding risk of dual antiplatelet therapy (DAPT) and OAT while trying to provide adequate stroke prophylaxis and prevent stent thrombosis. The WOEST trial was the first study to randomize 573 patients to receive dual or triple therapy using warfarin as the OAT. 2 After a median follow-up of 358 days, ischemic events were lower with dual therapy compared with triple therapy (11.1% vs. 17.6%), as was the secondary end point of all-cause death (2.5% vs. 6.3%). Subsequently, a Danish group published results of a real-life nationwide retrospective registry of 12,165 patients that supported the findings in the WOEST trial. 3 At 1 year, there was no increased risk of recurrent coronary events for dual therapy (HR: 0.69; 95% CI: 0.48 to 1.00) relative to triple therapy, and bleeding risk was also nonsignificantly lower for VKA plus clopidogrel (HR: 0.78, 95% CI: 0.55 to 1.12). There are 6 clinical randomized control trials (RCTs) in this area which suggest that dual therapy with 1 antiplatelet agent and OAT may be preferable to triple therapy with DAPT and OAT. 2,4 -8 These studies primarily provide data about bleeding risk as they are not statistically powered to detect thromboembolic risk. A recent meta-analysis of these RCTs found that treatment with dual therapy reduces clinically significant bleeding by 47% compared to triple therapy. 9 However, current guidelines do not provide direct recommendual therapyions regarding the use or dual therapy, triple therapy or DAPT in this patient population. 10 -14 In Europe, the European Society of Cardiology (ESC) recommend at least 1 month of triple therapy for all patients in this group but does concede that dual therapy may be more appropriate in certain cases. 15 The nebulous nature of these guidelines may lead to increased heterogeneity among prescribers when treating such patients. A recent analysis of the American College of Cardiology’s (ACC) National Cardiovascular Data Registry found that if 2 practices were selected at random they would differ in their likelihood of prescribing triple therapy for an identical patient by a factor of nearly 3. 16
In this study, we sought to investigate the prescribing practice of physicians for patients with an indication for OAT that undergo PCI in 2 tertiary Irish centers.
Methods
Study Design and Population
This was a multi-center retrospective observational analysis of patients with an indication for OAT who underwent PCI between 01 January 2017 and 31 December 2017. We identified patients through the PCI databases of 2 Irish tertiary centers (Cork University Hospital, Wilton, Cork and Tallaght University Hospital, Tallaght, Dublin). We included patients with both stable coronary artery disease (CAD) and acute coronary syndrome (ACS) who underwent both drug-eluting stent (DES) as well as bare-metal stent (BMS) placement. Patients were screened with the following inclusion and exclusion criteria:
Inclusion criteria: Subjects must be >18 years Must have undergone a PCI with stent placement Documented indication for oral anticoagulation
Exclusion criteria: Major bleeding within 30 days of PCI with stent placement Contraindications to use of VKAs, ASA or P2Y12 platelet inhibitors Pregnant or breastfeeding woman
Data Collection
For analysis, patients were divided into 3 groups by clinical risk: Bleeding-risk predominant (HASBLED > CHA2DS2VaSc), Equipoise risk (HASBLED = CHA2DS2VaSc) and Ischemic risk predominant (CHA2DS2VaSc > HASBLED). Baseline, demographic, clinical, laboratory and technical data was collected for all patients using our IT system and a database was formed. For analysis, patients had to be treated with one of 3 different treatment regimens: (1) a dual therapy consisting of a P2Y12 inhibitor alone in addition to OAT or (2) a triple therapy consisting of aspirin and a P2Y12 inhibitor in addition to OAT or (3) a DAPT consisting of aspirin and a P2Y12 inhibitor. Each of these individual strategies were then assessed to determine if they were appropriate as per the ESC 2017 focused update on DAPT in CAD. The following criteria were assessed for in the study as per the guidelines: Assessment of ischemic and bleeding risks using validated risk predictors (CHADS VASc, HAS-BLED). Shortest duration of triple therapy possible; Dual therapy to be considered instead of triple therapy. Use of NOACs preferably to VKA. If vitamin K antagonists (VKA) used, consider target INR in lower part of target range with maximization of time in therapeutic range (TTR). Clopidogrel to be used as the P2Y12 inhibitor of choice. Lower dose aspirin (<100 mg daily). Routine use of proton pump inhibitors (PPIs).
Consideration of the lower NOAC regimen tested in approval studies and apply other NOAC regimens based on drug specific criteria for drug accumulation.
Statistical Analysis
Variables are presented as the mean +/- standard deviation (SD) or numbers (percentages). Continuous variables were compared across groups using one-way analysis of variance (ANOVA). Categorical variables were compared using the Chi-square test or Fisher’s exact test as appropriate. All reported P-values are 2-tailed with P-values less than 0.05 considered statistically significant. Analyses were performed using the software package SPSS Statistics 24 (IBM, SPSS, Inc.).
Results
Baseline Demographics
The population consisted of 103 patients. Of these patients, 8 (7.8%) had a HASBLED score greater than their CHA2DS2VASc score (Bleeding Risk Predominant), 47 (45.6%) had equal scores (Equipoise Risk) and 48 (46.6%) had a CHA2DS2VASc greater than their HASBLED score (Ischemic Risk Predominant). The baseline characteristics differed between groups. As shown in Table 1 there were significantly more males in the bleeding and equipoise groups compared with the ischemic risk (100% vs. 93.6% vs. 66.7%, P < 0.001). As expected the ischemic group had significantly more current smokers (12.5% vs. 44.7% vs. 62.5%, P < 0.05), a greater likelihood of complex PCI (12.5% vs. 25.5% vs. 54.2%, P < 0.05) with an overall higher CHA2DS2VASc score (1.9 vs. 2.6 vs. 3.7, P < 0.001) compared to the other 2 groups.
Baseline Characteristics.
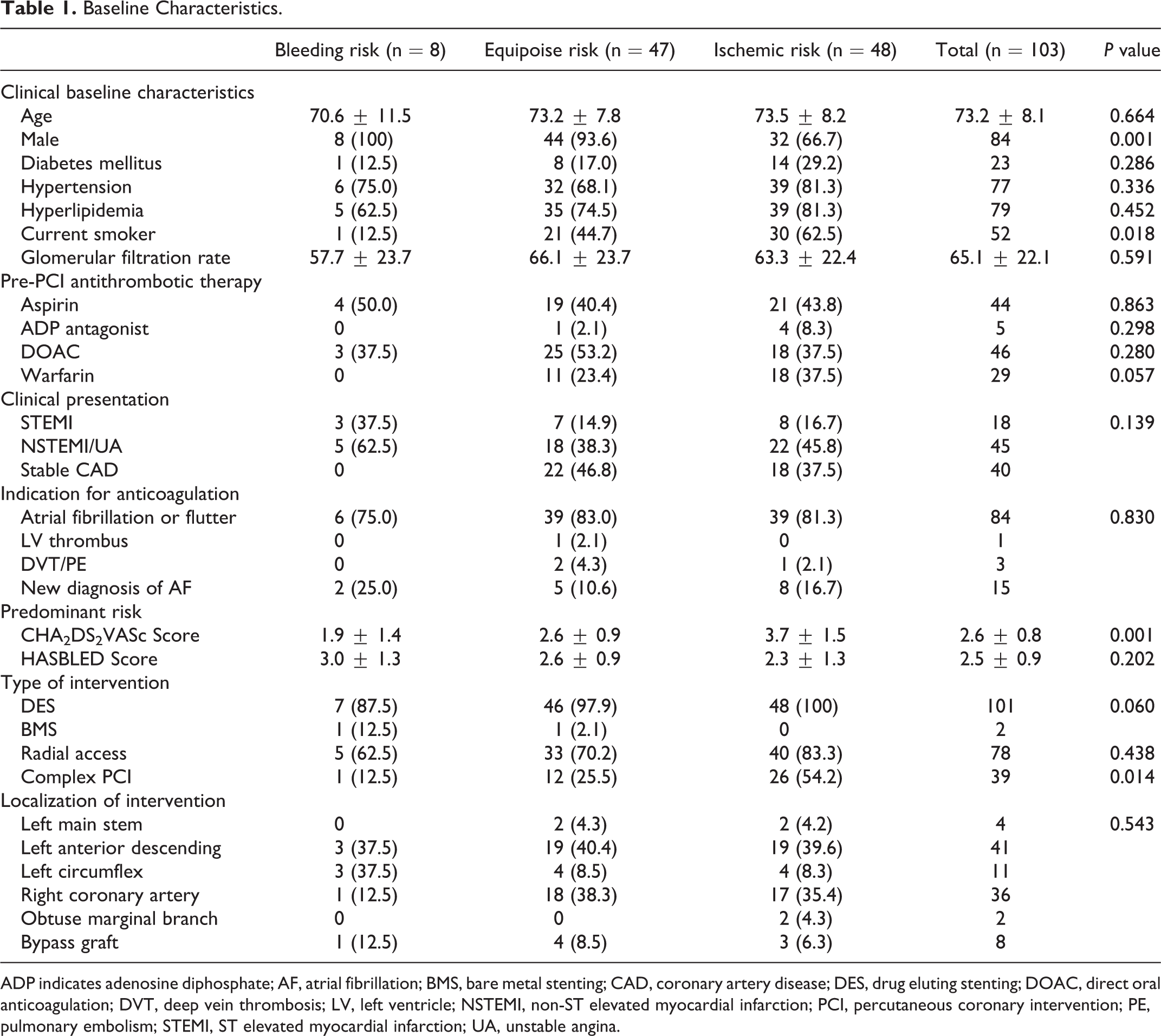
ADP indicates adenosine diphosphate; AF, atrial fibrillation; BMS, bare metal stenting; CAD, coronary artery disease; DES, drug eluting stenting; DOAC, direct oral anticoagulation; DVT, deep vein thrombosis; LV, left ventricle; NSTEMI, non-ST elevated myocardial infarction; PCI, percutaneous coronary intervention; PE, pulmonary embolism; STEMI, ST elevated myocardial infarction; UA, unstable angina.
Initial Anti-Thrombotic Strategy
Across the total population 97 patients (94.2%) were initially prescribed triple therapy. Patient with a greater ischemic risk were more likely to be prescribed triple therapy compared to those with a higher bleeding risk (75% vs. 95.7% vs. 95.8%, P < 0.05). In terms of OAT, DOACs were prescribed more commonly than warfarin (67.9% vs. 30.1%) but there was no statistically significant difference in likelihood of prescription between the 3 groups. Apixaban was the most commonly prescribed DOAC (46/70 patients, 64.7%) and significantly more patients were prescribed the reduced 2.5 mg twice daily dose if they were in the bleeding risk or equipoise risk group (50.0% vs. 44.7% vs. 25.0%, P < 0.05). The overall duration of triple therapy was most commonly 3 months across the entire population (43/97 patients, 44.3%). As shown in Figure 1, the duration of triple therapy differed significantly between groups with patients in the bleeding risk group more likely to be prescribed 1 month of triple therapy (66.7% vs. 17.8% vs. 26.1%, P < 0.05) and those with equipoise risk more likely to be prescribed 3 months (16.7% vs. 64.4% vs. 28.3%, P < 0.05). PPIs were prescribed for 86 patients (83.5%) and there was no significant difference between groups. Only 4 patients were prescribed dual therapy and 2 patients DAPT as an initial anti-thrombotic strategy. Of note, independent of CHA2DS2VASc score patients with a HASBLED score ≥ 4 were as likely to be prescribed triple therapy (95.0% vs. 93.9%, P = 0.399) for a shorter 1 month duration (45.0% vs. 20.5%, P < 0.05) and more likely to be prescribed warfarin (50.0% vs. 25.3%, P < 0.05) as compared to patients with a HASBLED score ≤ 3. Independent of HASBLED score, patients with CHA2DS2VASc score ≥ 4 were as likely to be prescribed triple therapy (100% vs. 91.5%, P = 0.344), and more likely to be prescribed warfarin (59.4% vs. 16.9%, P < 0.001) as compared to patients with a CHA2DS2VASc score ≤ 3.
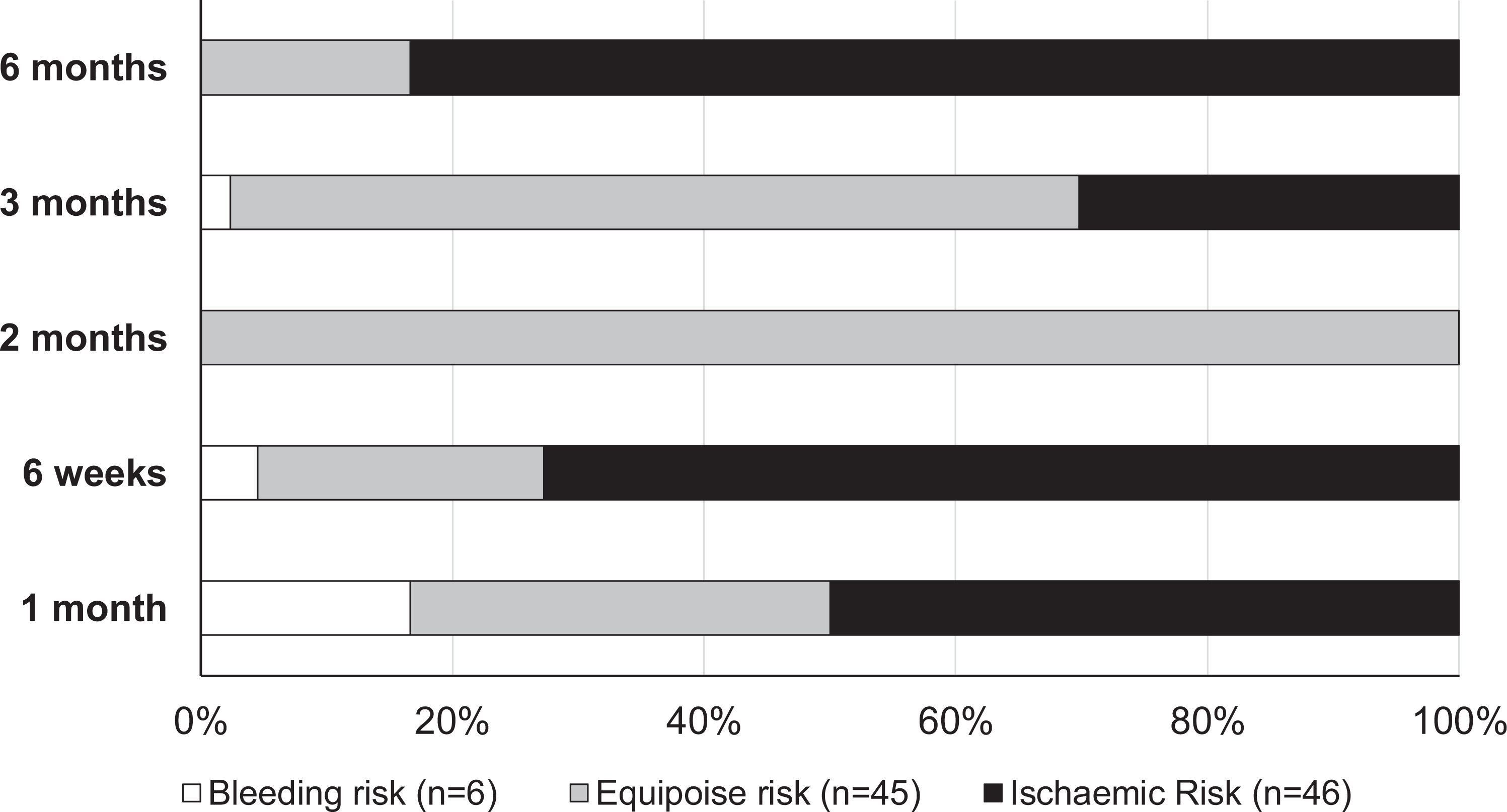
Duration of triple therapy across clinical risk groups.
Subsequent Anti-Thrombotic Strategy
The most common subsequent strategy was dual therapy (96/103 patients, 93.2%). The decision to switch to dual therapy after initial therapy did not differ between groups (75% vs. 95.7% vs. 93.8%, P = 0.143). The most commonly prescribed antiplatelet agent was aspirin (60/96 patients, 62.5%) which was prescribed more commonly in the ischemic risk group (12.5% vs. 51.1% vs. 72.9%, P < 0.05). Clopidogrel was prescribed for the remaining 36 patients on dual therapy (37.5%) which was more commonly prescribed in the bleeding risk group (62.5% vs. 44.7% vs. 20.8%, P < 0.05). Patients with a CHA2DS2VASc ≥ 4 were as likely to be prescribed dual therapy (91.6% vs. 96.9%, P = 0.583) compared to patients with a score ≤ 3. In comparison, patients with a HASBLED score ≥ 4 were as likely to be prescribed dual therapy (95.0% vs. 92.8%, P = 0.713) compared to patients with a score ≤ 3.
Strategy at 1 Year
The most common strategy 1 year post PCI was single OAT (50/100 patients, 50%) which was more commonly prescribed for those in the bleeding risk and equipoise groups (62.5% vs. 63.8% vs. 31.3%, P < 0.05). Those with a greater ischemic risk were more likely to continue dual therapy after 1 year (12.5% vs. 29.8% vs. 52.1%, P < 0.05). Three patients were prescribed DAPT after 1 year and 7 patients continued single antiplatelet agents. Patients with a CHA2DS2VASc ≥ 4 were as likely to be prescribed a single OAT (31.3% vs. 56.4%, P = 0.211) compared to patients with a score ≤ 3. In comparison, patients with a HASBLED score ≥ 4 were as likely to be prescribed a single OAT (25.0% vs. 54.2%, P = 0.349) compared to patients with a score ≤ 3.
Direct Oral Anticoagulant Prescribing
Overall 67.9% (70/103) of patients were prescribed DOACs as part of their treatment regimen. The most commonly prescribed DOAC was apixaban (46/70 patients, 65.7%), followed by rivaroxaban (20/70 patients, 28.6%). Dabigatran and Edoxaban accounted for the remaining 4 cases. In terms of dosing 80.4% of apixaban prescriptions were dosed at 2.5 mg BD (37/46 patients) while 63.1% of rivaroxaban prescriptions were dosed at 15 mg OD (13/20 patients). Dose reductions were considered inappropriate in 75.0% of apixaban prescriptions and 7.6% of rivaroxaban prescriptions. Inappropriate dose reductions did not differ significantly between risk predominance groups (50.0% vs. 64.3% vs. 61.1%, P = 0.069). Overall, 62.0% of DOAC dose reductions were considered inappropriate as per current guidelines. Inappropriate dose reductions were not independently predicted by HASBLED (P = 0.588) and CHA2DS2VASc (P = 0.314) Scores.
Clinical Outcomes
The MACE rate across the entire population was 12.6% which did not differ significantly between groups (P = 0.650). In Tables 2, 3 and 4 Patients with a HASBLED score greater than 3 had a significantly greater risk of a MACE compared to those with a score below 3 (21.6% vs. 4.1%, P < 0.05). The rate of minor bleeding was 11.6% which did not differ between groups (P = 0.604). There was only one recorded case of major bleeding in the ischemic risk group. In terms of minor bleeding rates there was no effect of PPI use (P = 0.230) or difference between DOACs and warfarin (P = 0.604).
Treatment Strategies in Patients With an indication for OAT Post PCI.

DAPT, dual antiplatelet therapy; OAT, oral anticoagulation therapy; DOAC, direct oral anticoagulant; PCI, percutaneous coronary intervention.
Oral Anticoagulation Therapy Prescriptions.

OAT, oral anticoagulation therapy.
Adverse Event Rates.

MACE indicates major adverse cardiovascular outcome; TIMI, Thrombolysis in Myocardial Infarction.
Discussion
Our retrospective study analyzed the prescribing habits of physicians in Ireland regarding OAT strategies post PCI in patients with a concomitant indication for OAT. Our findings showed that: (1) nearly 95% of patients were prescribed triple therapy post PCI; (2) triple therapy was most commonly prescribed for 3 months; (3) DOACs were prescribed more commonly than VKAs with a preference for low-dose apixaban and (4) dose-reduced DOACs were inappropriately prescribed in 60% of cases.
The initial treatment strategy was predominantly triple therapy (94.2%) followed by dual therapy (3.9%) and then DAPT (1.9%). Those with a higher bleeding risk were significantly less likely to be prescribed triple therapy. In terms of duration, 45% of patients continued triple therapy for 3 months while those with greater bleeding risks had shorter durations of therapy. The European Society of Cardiology (ESC) currently recommends at least 1 month of triple therapy for all AF patient who undergo PCI (Class II b evidence). 13 For those with a low bleeding risk after an ACS with stent placement, triple therapy for 1-6 months should be considered (Class II b). However, the ESC guidelines do recognize that triple therapy must be limited to the shortest possible time period and dual therapy should be considered as an alternative in selected patients. Moreover, the only Class I recommendation given by the American College of Cardiology (ACC) is to limit the duration of triple therapy and prescribe concomitant PPIs in those with a history of gastrointestinal bleeding. 10 PPIs were prescribed in 84% of cases in our cohort which was not influenced by bleeding risk.
Patients were most commonly switched to dual therapy after an initial period of triple therapy which was not influenced by the patients bleeding risk. Aspirin was more commonly co-prescribed than clopidogrel with a greater prescription rate in the ischemic group. This is unexpected given the apparent reduction in ischemic events associated with clopidogrel mono-therapy versus aspirin mono-therapy. 17 -19 It should be noted that the HASBLED scores between the equipoise and ischemic groups did not differ significantly therefore the decision to combine aspirin with OAT over clopidogrel was not driven by bleeding risk. The ESC/EHRA/ACC/AHA guidelines do not make any recommendations regarding the choice of single antiplatelet agent with dual therapy however clopidogrel remains the P2Y12 inhibitor of choice. 12,13
The most common strategy at 1 year was single OAT which occurred in half of all cases in line with the current guidelines. 12,13 This strategy was used most commonly in the bleeding and equipoise risk groups. Patients with a greater risk of ischemic events were significantly more likely to continue dual therapy (13% vs. 30% vs. 52%). Current guidelines do not recommend continuing dual therapy beyond 12 months regardless of ischemic risk. 12,13,20 The current consensus is to continue stroke prevention doses of OAT mono-therapy at 1 year.
As previously described in the PIONEER-AF-PCI trial DOACs demonstrated less clinically significant bleeding events compared with the warfarin group (16.8% vs. 18.0% vs. 26.7%, P < 0.001). Interestingly, the dose of rivaroxaban had no significant effect on bleeding risk (2.1% vs. 1.9%). Following the results of this study most current guidelines recommend DOAC therapy over a VKA. 12,13,20 In our study, DOACs were prescribed at more than twice the rate of warfarin with a significant preference toward apixaban. A reduced dose was prescribed in 80% of apixaban prescriptions and 63% of rivaroxaban prescriptions. The majority of apixaban prescribed (75%) at 2.5 mg BD PO dose were classified as under-dosed based on data from the ARISTOTLE trial and the dosing criteria in the current guidelines (apixaban 5 mg BD or 2.5 mg BD. if at least 2 of the following: age ≥80 years, body weight ≤60 kg or serum creatinine level ≥1.5 mg/dL (133 μmol/L). 12,13,20 -22 Clinical trial data combining OAT with antiplatelet therapy with AF post PCI are available for rivaroxaban, dabigatran and most recently apixaban. 4,6,7 The PIONEER-AF-PCI trial used rivaroxaban doses lower than previously established for stroke prevention which observed no increase in ischemic events however the trial was notably underpowered to detect such events. 7 The RE-DUAL used dabigatran doses at established stroke prevention doses. Thromboembolic events were similar for dual therapy (with dabigatran 110 mg BD or 150 mg BD) or triple therapy with warfarin, although a pooled analysis combining both doses of dabigatran dual therapy demonstrated a modest and non-significant 1.1% absolute increase in thrombotic events or death compared to the triple therapy group. 4 In the AUGUSTUS trial patients were directed to take 5 mg BD or 2.5 mg BD if they met the criteria mentioned above. 6,23 Triple therapy with apixaban demonstrated a 3.9% absolute risk reduction in death or hospitalization when compared with warfarin. The addition of aspirin to OAT was associated with a 7.1% absolute increase in clinically significant bleeding. Thromboembolic events were similar across all treatment arms (randomization 1: apixaban vs. warfarin; randomization 2: aspirin vs. placebo). Notably, however, there was a nonsignificant 0.4% absolute numerical increase in definite/probable stent thrombosis with the omission of aspirin. 6 When comparing the available trial data, the omission of aspirin increases the rate of stent thrombosis (55/5,024, 1.1% vs. 38/4,971, 0.8%) as well as MI (191/5,024, 3.8% vs. 154/4,971, 3.1%). 24 Overall these data provide direct evidence that triple therapy is associated with substantial increases in bleeding without clear clinical benefit when compared to dual therapy and OAT mono-therapy. The reduced dosing of apixaban in our study was likely an attempt to reduce bleeding while on DAPT however it was inappropriate in 4 out of 5 cases. Given the above data use of full dose apixaban in combination with a single antiplatelet agent may be a suitable evidence-based alternative to prevent thromboembolic events and reduce bleeding risk.
We also collected data on MACE rates although we acknowledge that our study is underpowered to detect such rare events. Across the entire population the MACE rate was 12.6%, all-cause mortality rate 9.7%, minor bleeding rate 11.6% with only one recorded case of major bleeding. There no effect of warfarin use on bleeding rate compared to DOACs despite previous clinical data. 4,6,7 The bleeding rates reported in this study were significantly lower than those previously clinical data. The retrospective nature of the study may misrepresent the bleeding rates.
Limitations
Our study had several limitations. Firstly, as mentioned above this data was collected retrospectively it is possible that clinical outcomes such as bleeding rates may not have been detected. Secondly, the widespread use of triple therapy severely limited our ability to assess the efficacy of other initial treatment modalities such as dual therapy. Finally, our study did not assess time in therapeutic range for warfarin which may limit our ability to extrapolate our results to other studies.
Conclusion
In conclusion, our study demonstrates the widespread use of triple therapy in clinical practice in the 2 Irish Hospitals studied. DOACs were prescribed in most cases at reduced doses not currently known to prevent stroke. This was presumably in an attempt to reduce the significant bleeding rates associated with triple therapy. Recent data suggest that treatment with full stroke-prevention dose DOACs in combination with an antiplatelet agent is as effective in preventing thrombotic events while significantly reducing bleeding rates. More direct recommendations from national and international guidelines are required to improve evidence-based anti-thrombotic therapy prescribing in patients with an indication for OAT undergoing PCI.
Footnotes
Authors’ Note
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussion interpretation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.