
Abstract
Despite contemporary management, patients with coronary artery disease (CAD) remain at high risk for thrombotic events. Several randomized controlled trials have evaluated the use of direct oral anticoagulants (DOACs) in patients with CAD, including in the setting of acute coronary syndrome (ACS) and stable CAD, and in patients with concomitant atrial fibrillation. Trials of apixaban and dabigatran in patients with ACS demonstrate no benefit with an increased risk of bleeding. Conversely, rivaroxaban at a reduced dose of 2.5 mg twice daily reduced thrombotic events and all-cause mortality when added to dual antiplatelet therapy in patients with ACS. Similarly, the addition of low-dose rivaroxaban to acetylsalicylic acid reduced the risk of thrombotic events in patients with stable CAD. However, the addition of a DOAC to antiplatelet therapy increased the risk of major bleeding. In patients with atrial fibrillation undergoing percutaneous coronary intervention, dual-pathway or low-dose triple therapy regimens including dabigatran or rivaroxaban reduced bleeding risk compared to traditional warfarin-based triple therapy, although it remains unclear whether these regimens preserve antithrombotic efficacy. DOAC–based antithrombotic regimens prove useful in patients with CAD in various settings; however, careful selection of patients and regimens per trial protocols are critical to achieving net benefit.
Introduction
Ischemic heart disease persists as the leading cause of mortality worldwide. 1 Antiplatelet agents are the cornerstone of secondary prevention, and guidelines recommend lifelong use of acetylsalicylic acid (ASA) in all patients with coronary artery disease (CAD) and dual antiplatelet therapy (DAPT) in patients following acute coronary syndrome (ACS) or percutaneous coronary intervention (PCI). 2,3 Despite the use of high-potency DAPT, patients with recent ACS remain at very high short-term risk for thrombotic events, with rates of major adverse cardiovascular events of approximately 10% at 1 year. 4,5 Moreover, extending DAPT beyond 1 year in patients with previous ACS or PCI provides minimal additional thrombotic protection and does not reduce the risk of death. 6,7
Five direct oral anticoagulants (DOACs) are now available in North America: apixaban, betrixaban, dabigatran, edoxaban, and rivaroxaban. By selectively targeting the coagulation cascade to decrease thrombus formation and propagation, these agents may provide an additional therapeutic target for secondary prevention in patients with CAD with advantages over use of a vitamin K antagonist (VKA). This article provides a review of the efficacy, safety, and place in therapy of DOACs in CAD.
Historical Role and Mechanistic Basis for Oral Anticoagulants in CAD
There has long been an interest in a possible additive antithrombotic effect of anticoagulants in CAD. Thrombin is implicated in the thrombus formation that causes myocardial infarction (MI) by activating fibrin, as well as promoting platelet aggregation and activation. 8 VKAss and factor Xa inhibitors (apixaban, betrixaban, edoxaban, and rivaroxaban) work by limiting thrombin generation, while thrombin inhibitors (dabigatran) directly inhibit thrombin enzymatic activity.
VKAss, such as warfarin, were the first oral anticoagulants to be evaluated in randomized controlled trials (RCTs) of secondary prevention in patients with CAD, alone or with ASA. These trials generally had high risk of bias due to lack of blinding, high discontinuation rates, and variable attainment of therapeutic anticoagulation. Anand and Yusuf conducted a meta-analysis of 37 trials (n = 37 984) with duration ≥3 months, published between 1960 and 2003, excluding coronary stent trials. 9,10 Reviewers evaluated thrombotic and bleeding outcomes, stratified by trials targeting international normalized ratio (INR) <2.0 versus ≥2.0. This study provided several insights regarding oral anticoagulants in CAD. First, VKA monotherapy with target INR ≥2.0 reduced thrombotic outcomes more than ASA monotherapy (odds ratio [OR]: 0.79, 95% confidence interval: 0.67-0.94), but increased major bleeding (OR: 2.1, 1.7-2.7). Second, adding anticoagulation (target INR ≥2.0) to ASA further reduced thrombotic events versus ASA monotherapy (OR: 0.88, 0.80-0.97) and increased major bleeds (OR: 1.74, 1.39-2.17). Similarly, a meta-analysis limited to patients with recent ACS observed that adding warfarin (target INR: 2.0-3.0) to ASA reduced thrombotic events (OR: 0.73, 0.63-0.84) and increased major bleeding (OR: 2.32, 1.63-3.29). 11 Although adding a VKA to ASA reduced thrombotic events, the increase in major bleeds, difficulties with treatment adherence, and frequency of testing and maintenance of therapeutic INR precluded widespread use.
Adding DOACs to DAPT in ACS
Five trials have evaluated the addition of DOACs to antiplatelet therapy in patients post-ACS. Table 1 summarizes key characteristics of these trials.
Summary of Randomized Controlled Trials Evaluating Direct Oral Anticoagulants in Patients After Acute Coronary Syndrome.

Abbreviations: ACS, acute coronary syndrome; bid, twice daily; CrCl, creatinine clearance; DOAC, direct oral anticoagulant; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction.
a Denotes a statistically significant difference versus control (P < .05).
b Includes prior PCI or coronary artery bypass grafting surgery.
The phase 2, double-blind Apixaban for Prevention of Acute Ischemic and Safety Events (APPRAISE) trial randomized clinically stable patients between 18 and 90 years of age within 7 days of ACS to 1 of 4 doses of apixaban or placebo. 12 To be eligible, patients required ≥1 additional high-risk characteristic, including age ≥65 years, elevated cardiac enzymes, ST-segment deviation, prior MI within 12 months, nonrevascularized multivessel CAD, cerebrovascular disease, peripheral vascular disease, heart failure or reduced ejection fraction, diabetes, or “mild-to-moderate” renal insufficiency. Key exclusion criteria included indication for ongoing anticoagulation, planned invasive procedure, severe renal insufficiency (not defined), active bleeding, anemia, and physician-determined high bleeding risk. The primary outcome was International Society on Thrombosis and Hemostasis (ISTH) major (fatal, symptomatic in a critical organ, that causes a ≥2 g/dL fall in hemoglobin or requires transfusion of ≥2 units of blood) or clinically relevant nonmajor (leads to hospital admission or medical care) bleeding. The secondary outcome was a composite of cardiovascular death, MI, severe recurrent ischemia, or ischemic stroke. The groups randomized to doses of 10 mg twice daily and 20 mg daily stopped the trial early due to excess bleeding. Apixaban produced a dose-dependent increase in bleeding compared to placebo (2.5 mg twice daily vs placebo, hazard ratio [HR]: 1.78, 95% CI: 0.91-3.48; 10 mg daily vs placebo, HR 2.45, 1.31-4.61), with a number needed to treat to harm (NNH) of 21 at 26 weeks for the 10 mg/d dose. Rates of the secondary ischemic outcome did not differ between groups (HR: 0.73, 0.44-1.19 for 2.5 mg twice daily vs placebo; HR: 0.61, 0.35-1.04 for 10 mg twice daily vs placebo).
The follow-up phase 3, double-blind APPRAISE-2 trial randomized patients ≥18 years of age within 7 days of ACS to apixaban or placebo. 13 To be eligible, patients required ≥2 additional high-risk characteristics, including age ≥65 years, prior MI within 5 years, no revascularization after the index event, cerebrovascular disease, peripheral vascular disease, heart failure or reduced ejection fraction, diabetes, or creatinine clearance (CrCl) <60 mL/min. Key exclusion criteria included indication for ongoing anticoagulation, CrCl <20 mL/min, active bleeding, or physician-determined high bleeding risk. The primary efficacy outcome was a composite of cardiovascular death, MI, or ischemic stroke. The primary safety outcome was Thrombolysis in Myocardial Infarction (TIMI) major bleeding, defined as fatal bleeding, intracranial hemorrhage, or overt bleeding with a reduction in hemoglobin ≥5 g/dL or hematocrit ≥15%. The trial was stopped prematurely for harm without benefit. Apixaban increased the risk of bleeding compared to placebo (NNH: 125; HR 2.59, 1.50-4.46) without significantly improving efficacy outcomes (HR: 0.95, 0.80-1.11). Furthermore, apixaban did not reduce the risk of any secondary efficacy end point, whereas it increased the risk of all secondary bleeding outcomes. Subgroup analyses demonstrated harm with apixaban whether added to DAPT or ASA alone. 14
The phase 2, double-blind Randomized Dabigatran Etexilate Dose Finding Study in Patients with Acute Coronary Syndromes Post Index Event with Additional Risk factors for Cardiovascular Complications Also Receiving Aspirin and Clopidogrel (RE-DEEM) trial randomized patients ≥18 years of age within 14 days of ACS to 1 of 4 doses of dabigatran or placebo, added to DAPT. 15 Patients required ≥1 high-risk characteristic similar to those used in APPRAISE-2. Key exclusion criteria included high bleeding risk (eg, major surgery in the previous month, history of severe bleeding, peptic ulcer within 30 days), uncontrolled hypertension, and CrCl <30 mL/min. The primary outcome was the incidence of ISTH major or clinically relevant minor bleeding. The secondary outcome was the composite of cardiovascular death, nonfatal MI, or nonhemorrhagic stroke. Dabigatran produced a dose-dependent increase in the primary bleeding outcome versus placebo (HR: 1.77, 0.70-4.50 for 50 mg; HR: 2.17, 0.88-5.31 for 75 mg; HR 3.92, 1.72-8.95 for 110 mg; HR 4.27, 1.86-9.81 for 150 mg). The corresponding NNH was 18 for the 2 higher doses versus placebo at 6 months. The trial was underpowered for efficacy outcomes, and no phase 3 study was conducted based on these findings.
In contrast to the above trials, results with rivaroxaban were more favorable. The phase 2, double-blind Anti-Xa Therapy to Lower cardiovascular events in addition to Aspirin with or without thienopyridine therapy in Subjects with Acute Coronary Syndrome-Thrombolysis In Myocardial Infarction (ATLAS ACS-TIMI) 46 trial randomized patients 18 to 75 years of age within 7 days of ACS to 1 of several rivaroxaban regimens or placebo, stratified by use of ASA alone (stratum 1) or DAPT (stratum 2), which was at the treating physician’s discretion. 16 Key exclusion criteria included hemoglobin <100 g/L, platelet count <90 000/µL, or history of intracranial hemorrhage. The primary safety outcome was TIMI major or minor bleeding or bleeding requiring medical attention. The primary efficacy outcome was a composite of death, MI, stroke, or severe recurrent ischemia requiring revascularization. Rivaroxaban produced a dose-dependent increase in bleeding in both strata (HR ranging from 0.81 to 6.69), which was significantly higher than placebo with all doses except 2.5 mg twice daily. Bleeding did not differ between once-daily (12.1%) or twice-daily dosing (11.3%, P = .52). Bleeding rates were higher in the DAPT stratum (eg 3.8% vs 1.7% in the ASA stratum in pooled placebo groups). Efficacy did not significantly differ between any dose of rivaroxaban and placebo (pooled HR: 0.79, 0.60-1.05).
Based on these results, the phase 3, double-blind ATLAS ACS 2-TIMI 51 trial randomized patients ≥18 years of age within 7 days of ACS to 1 of 2 low-dose regimens of rivaroxaban or placebo, added to DAPT. 17 Patients required ≥1 additional high-risk characteristic, including age ≥55 years, prior MI, or diabetes. Key exclusion criteria included high risk of bleeding (eg, prior intracranial hemorrhage, recent gastrointestinal bleed), CrCl <30 mL/min, or indication for oral anticoagulation. The primary efficacy outcome was a composite of cardiovascular death, MI, or any stroke, and the primary safety outcome was non-coronary artery bypass graft (CABG) TIMI major bleeding. Both doses of rivaroxaban significantly reduced the risk of the primary efficacy outcome compared to placebo (HR: 0.84, 0.72-0.97 for 2.5 mg; HR: 0.85, 0.73-0.98 for 5 mg), corresponding to numbers need to treat to benefit (NNTs) of 63 and 53, respectively, at a median of 13.1 months. Notably, rivaroxaban 2.5 mg twice daily also reduced the risk of all-cause mortality (NNT: 63; HR: 0.68, 0.53-0.87) and stent thrombosis (NNT: 143; HR: 0.65, 0.45-0.94) versus placebo. Conversely, the higher rivaroxaban dose significantly reduced MI compared to placebo (NNT: 59; HR: 0.79, 0.65-0.97), but not stent thrombosis or the other components of the primary outcome. Both rivaroxaban doses increased the risk of the primary bleeding outcome (HR: 3.46, 2.08-5.77 for 2.5 mg; HR: 4.47, 2.71-7.36 for 5 mg), with respective NNHs of 84 and 56. The primary bleeding outcome did not differ significantly between the 2 rivaroxaban doses; however, rates of fatal bleeding, bleeding requiring medical attention, and minor bleeding were all significantly lower with the lower versus higher dose.
Finally, the US Food and Drug Administration did not approve rivaroxaban for secondary prevention post-ACS due to concerns regarding a high rate of missing data in ATLAS ACS 2-TIMI 51 and lack of a dose–response gradient for efficacy. 18 This decision was further justified on the basis of other negative DOAC trials; however, the key difference between ATLAS ACS 2-TIMI 51 and other trials of DOACs in ACS was the use of low-dose regimens of rivaroxaban, with the 2.5 mg twice-daily dose being equivalent to 25% of the dose indicated for stroke prevention in atrial fibrillation. A network meta-analysis suggested that DAPT with ASA plus ticagrelor had a better risk–benefit profile than the combination of a DOAC with ASA plus clopidogrel. 19 As prasugrel and ticagrelor replaced clopidogrel as the standard of care in DAPT regimens, interest in adding a DOAC to DAPT in the first year after ACS dwindled.
Substituting a DOAC for ASA in ACS
Although trials evaluating P2Y12 inhibitors in ACS to date have required concomitant ASA, emerging basic science and preliminary trials suggest that ASA may be omitted, particularly with the more potent agents. 20 For instance, mechanistic studies have demonstrated that prasugrel and ticagrelor inhibit thromboxane A2 production to a similar degree to ASA and that the addition of ASA did not further inhibit platelet aggregation. 20 These observations led to the hypothesis that ASA may be of limited benefit in combination with a P2Y12 inhibitor and that substitution with a DOAC may be more effective.
The GEMINI-ACS-1 trial assessed the impact of replacing ASA with low-dose rivaroxaban (key points summarized in Table 1). 21 In this double-blind, phase 2 safety RCT, investigators randomized patients ≥18 years of age within 10 days of ACS hospital admission receiving clopidogrel or ticagrelor to either rivaroxaban 2.5 mg twice daily (dual-pathway) or ASA 100 mg daily (DAPT) for a minimum of 6 months. As in ATLAS ACS-2 TIMI 51, additional inclusion criteria included age ≥55 years, prior MI, or diabetes. Key exclusion criteria were the same as ATLAS ACS-2 TIMI 51, with the addition of CrCl <20 mL/min. The primary outcome was TIMI non-CABG-related bleeding or bleeding requiring medical attention. The composite of cardiovascular death, MI, stroke, or definite stent thrombosis was an exploratory secondary ischemic outcome. Patients received the study drug for a median of 291 days and were followed for a median of 326 days. Bleeding risk was similar with rivaroxaban and ASA (HR: 1.09, 0.80-1.50). Alternate bleeding definitions generally demonstrated similar findings; however, rivaroxaban increased the risk of ISTH major bleeding compared to ASA (NNH: 100; HR: 1.83, 1.01-3.31). There was no significant difference in the ischemic outcome (HR: 1.06, 0.77-1.46). Relative risk estimates were similar whether patients received clopidogrel or ticagrelor.
GEMINI-ACS-1 did not demonstrate an advantage of a dual-pathway regimen over DAPT in patients with ACS. Although efficacy was comparable, this trial was underpowered to rule out major differences in ischemic outcomes, and there was an increase in ISTH major bleeding with the dual-pathway regimen.
Direct Oral Anticoagulants in Stable CAD
In the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trial, investigators randomized 27 395 patients ≥18 years of age with CAD and/or peripheral artery disease (PAD) in a double-blind manner to rivaroxaban 5 mg twice daily, ASA 100 mg daily, or dual-pathway therapy with rivaroxaban 2.5 mg twice daily plus ASA 100 mg daily. 22 Furthermore, patients not already on a proton pump inhibitor (PPI) at baseline were also randomized to pantoprazole versus placebo. To be eligible, patients with CAD also required ≥1 of the following: age ≥65 years, atherosclerosis in ≥2 vascular beds, or ≥2 additional high-risk characteristics (current smoker, diabetes, estimated glomerular filtration rate [eGFR] <60 mL/min, or nonlacunar stroke). Key exclusion criteria were indication for ongoing antithrombotic therapy beyond ASA, high bleeding risk according to clinician discretion, stroke within 1 month, prior hemorrhagic or lacunar stroke, severe heart failure, or eGFR <15 mL/min. The primary efficacy outcome was a composite of cardiovascular death, MI, or stroke. The primary safety outcome was modified ISTH major bleeding consisting of bleeding that was fatal, symptomatic into a critical organ, into a surgical site requiring reoperation, or that led to hospitalization. At baseline, 91% had CAD, 62% had a prior MI on average 7 years prior to enrollment, 27% had PAD, and 36% received a PPI. The trial was stopped early for efficacy at a mean follow-up of 23 months. The dual-pathway regimen reduced the composite efficacy outcome versus ASA alone (NNT: 77; HR: 0.76, 0.66-0.86), as well as stroke (NNT: 143; HR: 0.58, 0.44-0.76). Notably, the dual-pathway regimen also reduced the risk of all-cause mortality compared to ASA alone (NNT: 143; HR: 0.82, 0.71-0.96, P = .01), though this did not meet the conservative threshold for statistical significance of P < .0025 adjusted for multiple comparisons. Rivaroxaban monotherapy was not more efficacious than ASA alone (HR: 0.90, 0.79-1.03). Both rivaroxaban-based regimens increased the risk of the primary bleeding outcome compared to ASA alone (NNH: 84; HR: 1.70, 1.40-2.05 for dual-pathway; NNH: 112; HR: 1.51, 1.25-1.84 for rivaroxaban), which was mainly driven by a greater risk of gastrointestinal bleeding. The dual-pathway regimen did not significantly increase symptomatic intracranial hemorrhage or fatal bleeds over ASA alone (HR: 1.23, 0.76-2.01). Results were virtually identical in the CAD-only subgroup and consistent in subgroup analyses based on prior MI, prior PCI, and number of risk factors. 23
COMPASS demonstrated that adding low-dose rivaroxaban to ASA in high-risk patients with CAD effectively reduces thrombotic outcomes at the expense of more bleeding. This largely mirrors data from warfarin meta-analyses and rivaroxaban in ACS, albeit with a better benefit–risk profile with less intensive laboratory monitoring requirements. To achieve these positive outcomes, it is imperative for clinicians to consider this therapy only for patients with stable CAD with high residual thrombotic risk, low risk of bleeding, and high motivation to adhere to the twice-daily regimen, as included in this trial.
Direct Oral Anticoagulants in Patients With Atrial Fibrillation (AF) Undergoing PCI
AF is a common comorbidity among patients with CAD that presents a challenge in selecting the ideal antithrombotic regimen, particularly for those undergoing PCI. Warfarin is superior to DAPT (ASA plus clopidogrel) in preventing stroke and systemic embolism in AF, as demonstrated in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events-Warfarin (ACTIVE-W) study of patients with a mean CHADS2 score of 2. 24 Conversely, targeting platelets (particularly with a P2Y12 inhibitor) appears to be more important in coronary protection. A meta-analysis comparing warfarin plus ASA to DAPT in patients undergoing elective bare-metal stent implantation demonstrated a lower risk of thrombotic events with DAPT at 30 days (NNT: 22; relative risk: 0.41, 0.25-0.89). 25 As a result, clinicians have historically prescribed triple therapy (ASA plus P2Y12 inhibitor plus warfarin with a target INR 2.0-3.0) for patients with AF undergoing PCI or with recent ACS, which resulted in an annual risk of major bleeding as high as 14%, representing an approximate doubling of risk versus DAPT or a dual-pathway regimen. 26,27 The What is the Optimal antiplatElet and anticoagulant therapy in patients with oral anticoagulation and coronary StenTing (WOEST) trial (n = 573) provided proof-of-concept data that using a dual-pathway regimen consisting of warfarin plus clopidogrel could reduce the risk of bleeding while potentially preserving thrombotic efficacy in patients with an indication for long-term anticoagulation undergoing PCI. 28 Notably, however, WOEST was underpowered for outcomes other than a composite of major and minor bleeding.
Two trials further extended these findings to DOACs, summarized in Table 2. The OPen-Label, Randomized, Controlled, Multicenter Study ExplorIng TwO TreatmeNt StratEgiEs of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects with Atrial Fibrillation who Undergo Percutaneous Coronary Intervention (PIONEER AF-PCI) trial was an open-label RCT that randomized patients ≥18 years of age with nonvalvular AF undergoing PCI with stent placement to 1 of 2 rivaroxaban-based antithrombotic regimens or standard triple therapy. 29 Key exclusion criteria were previous stroke or transient ischemic attack, CrCl <30 mL/min, clinically significant gastrointestinal bleeding within 12 months, or any condition known to increase the risk of bleeding. The primary bleeding outcome was a composite of TIMI major or minor bleeding, and bleeding requiring medical attention. A secondary outcome included major adverse cardiovascular events, defined as cardiovascular death, MI, or stroke. Both rivaroxaban-based regimens reduced the primary bleeding outcome compared to standard triple therapy (NNT: 11; HR: 0.59, 0.47-0.76 for dual-pathway; NNT: 12; HR: 0.63, 0.50-0.80 for low-dose DOAC-based triple therapy). This difference became apparent within the first 30 days and continued to the end of follow-up. Bleeding requiring medical attention, the least severe component of the outcome, accounted for 85% of events and drove this difference. There were no significant differences in the rates of major adverse cardiovascular events (Table 2, P ≥.75), but this trial was underpowered for these outcomes. Notably, a post hoc analysis of PIONEER AF-PCI demonstrated that these rivaroxaban-based regimens also reduced the composite of all-cause mortality or hospitalization (NNT: 15; HR: 0.79, 0.66-0.94 for dual-pathway; NNT: 10; HR: 0.75, 0.62-0.90 for low-dose DOAC-based triple therapy). These differences were driven by a reduction in deaths and hospitalizations related to bleeding or cardiovascular events. 30
Summary of Randomized Controlled Trials Evaluating Direct Oral Anticoagulants in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention.
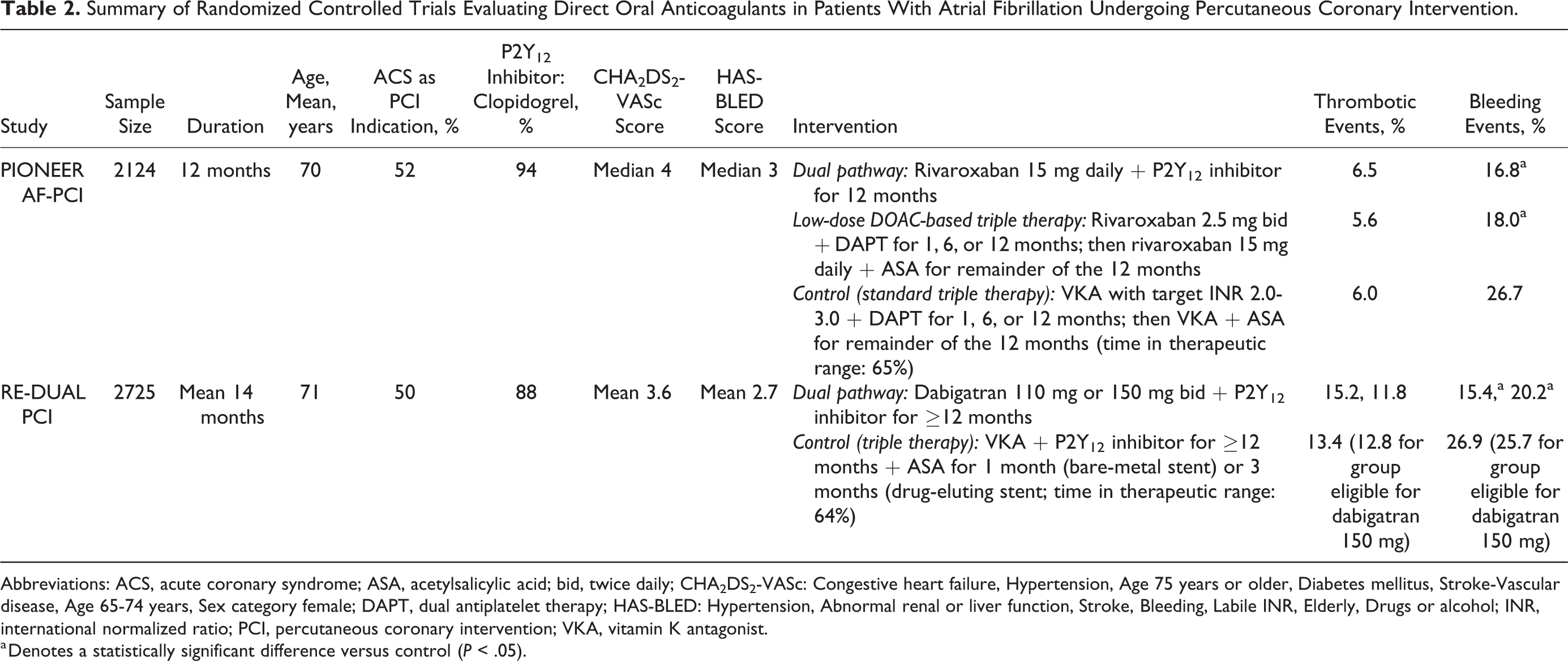
Abbreviations: ACS, acute coronary syndrome; ASA, acetylsalicylic acid; bid, twice daily; CHA2DS2-VASc: Congestive heart failure, Hypertension, Age 75 years or older, Diabetes mellitus, Stroke-Vascular disease, Age 65-74 years, Sex category female; DAPT, dual antiplatelet therapy; HAS-BLED: Hypertension, Abnormal renal or liver function, Stroke, Bleeding, Labile INR, Elderly, Drugs or alcohol; INR, international normalized ratio; PCI, percutaneous coronary intervention; VKA, vitamin K antagonist.
a Denotes a statistically significant difference versus control (P < .05).
The Randomized Evaluation of Dual Antithrombotic Therapy with Dabigatran versus Triple Therapy with Warfarin in Patients with Nonvalvular Atrial Fibrillation Undergoing Percutaneous Coronary Intervention (RE-DUAL PCI) trial extended these findings to dabigatran. 31 RE-DUAL PCI randomized patients ≥18 years of age with nonvalvular AF enrolled within 5 days of PCI with stent placement in an open-label manner to dual-pathway therapy with dabigatran, or warfarin-based triple therapy. Key exclusion criteria were CrCl <30 mL/min and high bleeding risk (eg, within 1 month of major surgery or gastrointestinal hemorrhage). Elderly patients outside of the United States were not eligible for the dabigatran 150 mg twice-daily regimen according to national product monographs in those countries (≥70 years in Japan, ≥80 years elsewhere). The primary outcome was ISTH major or clinically relevant nonmajor bleeding. The key secondary outcome was a composite of thromboembolic events (MI, stroke, or systemic embolism), death, or unplanned coronary revascularization. RE-DUAL was a noninferiority trial that required the upper end of the 95% CI for HR to fall below 1.38 for safety and efficacy to conclude noninferiority. Dual-pathway therapy with dabigatran 150 mg twice daily reduced the risk of the primary bleeding outcome compared to triple therapy (NNT: 19; HR: 0.72, 0.58-0.88) and significantly reduced ISTH major bleeding (NNT: 36; HR: 0.64, 0.43-0.94). This difference occurred in the first 90 days (when patients in the triple therapy group were still receiving ASA) and persisted after ASA discontinuation. This dual-pathway regimen also demonstrated noninferiority to triple therapy for the key secondary efficacy outcome (HR: 0.89, 0.67-1.19). Dual-pathway therapy with dabigatran 110 mg twice daily reduced the primary bleeding outcome compared to triple therapy (NNT: 9; HR: 0.72, 0.58-0.88); however, it did not meet the criteria for noninferiority for efficacy (HR: 1.13, 0.90-1.43). Furthermore, rates of death (5.6% vs 4.9%), MI (4.5% vs 3.0%), and definite stent thrombosis (1.5% vs 0.8%) were all numerically higher with dabigatran 110 mg twice daily compared to triple therapy. Although the trial was not powered to identify a statistically significant difference in efficacy outcomes, this trend was consistent with prior studies showing a greater risk of MI with dabigatran compared to warfarin. 32,33
Overall, the above trials support the role of reducing the intensity of antithrombotic regimens from standard triple therapy in patients with AF undergoing PCI. A meta-analysis of these trials confirmed these findings. 34 Dual-pathway regimens including rivaroxaban 15 mg daily or dabigatran 150 mg twice daily plus clopidogrel or rivaroxaban 2.5 mg twice daily plus DAPT reduce the risk of clinically relevant bleeding, and perhaps deaths and rehospitalizations. A regimen of warfarin plus clopidogrel for up to 12 months as tested in the WOEST trial represents another reasonable option, particularly for patients with CrCl <30 mL/min or other contraindications to a DOAC. 28 Notably, trials to date have not compared DOAC-based to warfarin-based dual-pathway regimens. Although none of these trials had sufficient power to demonstrate equivalence of antithrombotic efficacy compared to triple therapy, differences are likely small and insufficient to counterbalance the substantial reduction in bleeding. Conversely, a dual-pathway regimen including dabigatran 110 mg twice daily is likely insufficient to prevent coronary events and should be avoided.
Guideline Recommendations and Place in Therapy
Of the relevant North American guidelines, 2,3,35 -38 only the 2012 Canadian Cardiovascular Society (CCS) antiplatelet update provides recommendations relating to the use of DOACs after ACS. These guidelines recommend DAPT with ticagrelor or prasugrel over adding low-dose rivaroxaban to ASA plus clopidogrel and recommend against the use of triple therapy with dabigatran or apixaban. 38
No published guidelines have incorporated the findings from COMPASS. Based on the reduction in thrombotic events and possible reduction in mortality seen in this trial, it would be reasonable to consider adding rivaroxaban 2.5 mg twice daily to ASA 75 to 100 mg/d in patients with stable CAD, ≥1 high-risk feature, low risk of bleeding, and no ongoing indication for DAPT or full-dose anticoagulation once this dosage form becomes available. Approval of this dose and indication by the FDA is pending as of the time of this writing. No evidence has compared low-dose rivaroxaban plus ASA to extending DAPT beyond 1 year after ACS or PCI. However, the results of COMPASS are more compelling than those of trials extending DAPT beyond 1 year, such as the DAPT and Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin (PEGASUS) trials, and clinicians could consider switching to low-dose rivaroxaban plus ASA ≥1 year after ACS or ≥6 months after elective PCI.
The 2018 update to the CCS antiplatelet guidelines provide guidance for patients with concomitant CAD and nonvalvular AF. 39 First, for all combinations including an anticoagulant, the guidelines recommend using a DOAC over warfarin where appropriate. For patients with AF with low thromboembolic risk (CHADS2 = 0 and age <65 years) undergoing PCI, they recommend DAPT only. For patients with AF for whom an anticoagulant is indicated (ie, age ≥65 years or CHADS2 ≥1) who undergo elective PCI without high-risk features, they recommend an anticoagulant plus clopidogrel (without ASA) for up to 12 months, followed by lifelong oral anticoagulation monotherapy. High-risk features include implantation of multiple stents, complex bifurcation lesion, total stent length >60 mm, stenting of chronic total occlusion, multivessel CAD, prior stent thrombosis, current smoker, diabetes, or CrCl < 60 mL/min. For patients with AF requiring anticoagulation plus PCI for ACS or with high-risk features, they recommend initial triple therapy with ASA plus clopidogrel and oral anticoagulation for a duration of up to 6 months depending on thrombotic and bleeding risk, followed by clopidogrel plus oral anticoagulation for the remainder of the first year, and then lifelong anticoagulant monotherapy. This final recommendation to consider up to 6 months of triple therapy was made primarily on the basis of expert opinion, whereas other recommendations were based primarily on PIONEER AF-PCI, RE-DUAL, and WOEST.
For all these scenarios, clinicians should consider the use of a PPI to reduce the risk of gastrointestinal bleeds. None of the reviewed trials mandated use of PPI or other gastroprotection. The ongoing PPI arm of COMPASS will provide estimates of benefits and potential risks of PPI use in patients with stable CAD on ASA, rivaroxaban, or both. 22
Areas of Uncertainty
Although DOACs present new antithrombotic options for patients with CAD, several questions arise. For patients with ACS, it remains to be ascertained whether substituting low-dose rivaroxaban for ASA (dual-pathway therapy) or the addition of low-dose rivaroxaban to ASA plus ticagrelor/prasugrel (high-potency triple therapy) could further enhance efficacy and in whom the benefits would outweigh the increased bleeding risk. Furthermore, the optimal strategy for patients with stable CAD who have completed their first year of DAPT—whether it is a dual-pathway regimen or extended DAPT—is unclear. Finally, there is a need to confirm if dual-pathway therapy is truly as effective as triple therapy in patients with AF undergoing PCI and which—if any—patients may benefit from short-term triple therapy before switching to dual-pathway therapy.
Conclusion
Direct oral anticoagulants have a role in carefully selected patients with CAD. Low-dose rivaroxaban may be a particularly useful adjunct to ASA in patients with stable CAD; however, this must be weighed against an increased risk of major bleeding. Triple therapy with low-dose rivaroxaban (2.5 mg twice daily) plus ASA and clopidogrel and dual-pathway regimens using rivaroxaban 15 mg daily or dabigatran 150 mg twice daily have demonstrated a reduced risk of bleeding versus standard triple therapy in patients with AF undergoing PCI and appear to provide comparable antithrombotic efficacy.
Footnotes
Author Contributions
R. Turgeon contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. M. Ackman contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. H. Babadagli contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. J. Basaraba contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. J. Chen contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. M. Omar contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. J. Zhou contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.