
Abstract
Introduction:
Supplemental oxygen has been used in the setting of acute myocardial infarction (AMI). Once an official recommendation in the guidelines for the management of acute ST-segment elevation myocardial infarction, it is now mentioned as an intervention to be considered. Data for the use of supplemental oxygen or AMI are limited, and some data have suggested associated harm.
Methods:
We performed a systematic review of the literature and a subsequent meta-analysis of the data to determine the effect of high concentration oxygen versus titrated oxygen or room air in the setting of AMI. The following end points were studied: in-hospital mortality, opiate use, percentage of infarcted myocardium by magnetic resonance imaging (MRI), and mass of infarcted myocardium by MRI.
Results:
No significant difference was noted with end points when comparing those randomized to high-concentration oxygen versus those randomized to titrated oxygen or room air in the setting of AMI. No significant publication bias was identified although this could not be assessed for all end points.
Conclusion:
High-concentration oxygen may not offer any benefit when compared to titrated oxygen or room air. A large, randomized trial is warranted to further delineate these differences with respect to multiple end points.
Introduction
Supplemental oxygen has been a part of the routine management for acute myocardial infarction (AMI). The 2004 American College of Cardiology/American Heart Association guidelines for the management of patients with ST-segment elevation myocardial infarction included administration of supplemental oxygen for patients with arterial saturations of less than 90% as a class I recommendation and included administration of supplemental oxygen for all patients with AMI during the first 6 hours as a class IIa recommendation. 1 The 2013 guidelines no longer recommend oxygen therapy and rather simply state that supplemental oxygen be given consideration in light of limited data regarding its use. 2
Data for oxygen therapy come from 2 studies done in dogs and only a handful of human studies, with much of these data being from an era in which thrombolytic therapy was not available. Newer studies have even demonstrated an association of liberal oxygen supplemental use in the setting of AMI with harm. 3 –6 Decrease in coronary blood flow, decrease in myocardial oxygen consumption, decrease in cardiac output, increase in systemic vascular resistance, and increase in reperfusion injury in patients with cardiac disease when exposed to hyperoxia may all be possible mechanisms. 7 –10
We conducted a systematic review of the literature with a meta-analysis of available data to compare the use of high concentration oxygen versus titrated oxygen or room air in the setting of AMI.
Methods
Identified Outcomes
The aim of the study was to determine the effect of high concentration oxygen versus titrated oxygen or room air in the setting of AMI. Preliminary review of studies identified the following end points for comparison: in-hospital mortality, opiate use as a surrogate for pain, infarction percentage by magnetic resonance imaging (MRI), and infarction mass by MRI.
Search Methodology and Study Identification
Electronic databases PubMed, EMBASE, Medline, and the Cochrane central register of clinical trials were searched for pertinent studies. Each database was queried using the following search terms: “acute myocardial infarction,” “coronary thrombosis,” and “heart attack” in isolation or in combination with one of the following search terms: “supplemental oxygen,” “oxygen,” “room air,” “hypoxemia,” “normobaric,” and “hyperbaric.” There were no restrictions placed on date or language of publication.
Resulting manuscripts were reviewed by title and abstract with pertinent manuscripts being selected for full-text review. Full-text review was then conducted with additional studies being excluded if felt to not be pertinent to the study question. References of manuscripts undergoing full-text review were also reviewed to identify additional manuscripts. Cited Web sites were also visited for additional data. This search methodology was carried out by 2 authors (RL and KN) independently with subsequent comparison and reconciliation of any differences.
Bias Assessment
The Cochrane Collaboration’s tool for assessing risk of bias was utilized for the assessment. This tool assesses for adequate sequence generation, allocation concealment, blinding, incomplete reporting of outcome data, selective reporting of outcome data, and other potential areas of bias. Bias assessment of studies identified for inclusion in the study was done by 2 authors independently (KN and SA) with subsequent comparison and reconciliation of any differences.
Publication bias was assessed by both a qualitative and quantitative method. Funnel plots were created for visual assessment of publication bias, and an Egger test was conducted to quantify publication bias.
Data Abstraction
Data abstraction was done for previously identified end points using a data collection tool. Data abstraction was done by 2 authors independently (RL and SA) with subsequent comparison and reconciliation of any differences. Authors of included studies were not contacted for additional data.
Data Analysis
Continuous data are presented as means. Categorical data are presented as frequencies with absolute numbers as well as percentages. P values of ≤.05 were considered statistically significant. Pooled analysis was conducted using a Haenszel-Mantel fixed-effects model when significant heterogeneity was not present and using DerSimonian and Laird random-effects model when significant heterogeneity was present. Heterogeneity was assessed using both chi-square and I2 tests. The odds ratio was calculated for categorical variables while mean difference was calculated for continuous variables. The 95% confidence intervals were also calculated for each. Forest plots were generated for each end point. This analysis was done using Comprehensive Meta-Analysis version 3.0 (Englewood, New Jersey). Meta-regression was conducted for in-hospital mortality using year of publication, age, and gender as variables in the regression model.
Results
Study Identification
A total of 4371 studies were identified with 2508 remaining after duplicates were removed (Figure 1). Of these studies, 162 were identified for review of the full text. Ultimately, 5 studies were included in the final analysis. 11 –15 One of these studies was not published in a journal but had data available online with its methods previously published. 11,16 There were a total of 446 patients in the high concentration oxygen and 467 patients in the titrated oxygen or room air group. Patient characteristics for included studies are provided in Table 1.

Study methodology.
Patient Characteristics in Included Studies.

In-Hospital Mortality
A total of 4 studies with 425 patients in the high-concentration oxygen and 447 patients in the titrated oxygen or room air group (Figure 2). A fixed-effects model was used as significant heterogeneity was not present (Q = 6.123, P = .106, I2 = 51%). The in-hospital mortality rate was 4% among those receiving high-concentration oxygen and 3% among those receiving room air. No significant difference was noted between the 2 groups (odds ratio 0.981, 95% confidence interval 0.439-2.195).

Forest plot comparing in-hospital mortality.
Opiate Use
Data for opiate use were extracted from 2 studies with 102 patients in the high concentration oxygen group and 97 in the titrated oxygen or room air group (Figure 3). A fixed-effects model was used as significant heterogeneity was not present (Q = 2.140, P = .144, I2 = 53%). Opiate use was needed in 72% of those receiving high-concentration oxygen and 72% of those receiving room air. No significant difference was noted between the 2 groups (odds ratio 0.990, 95% confidence interval 0.526-1.865).
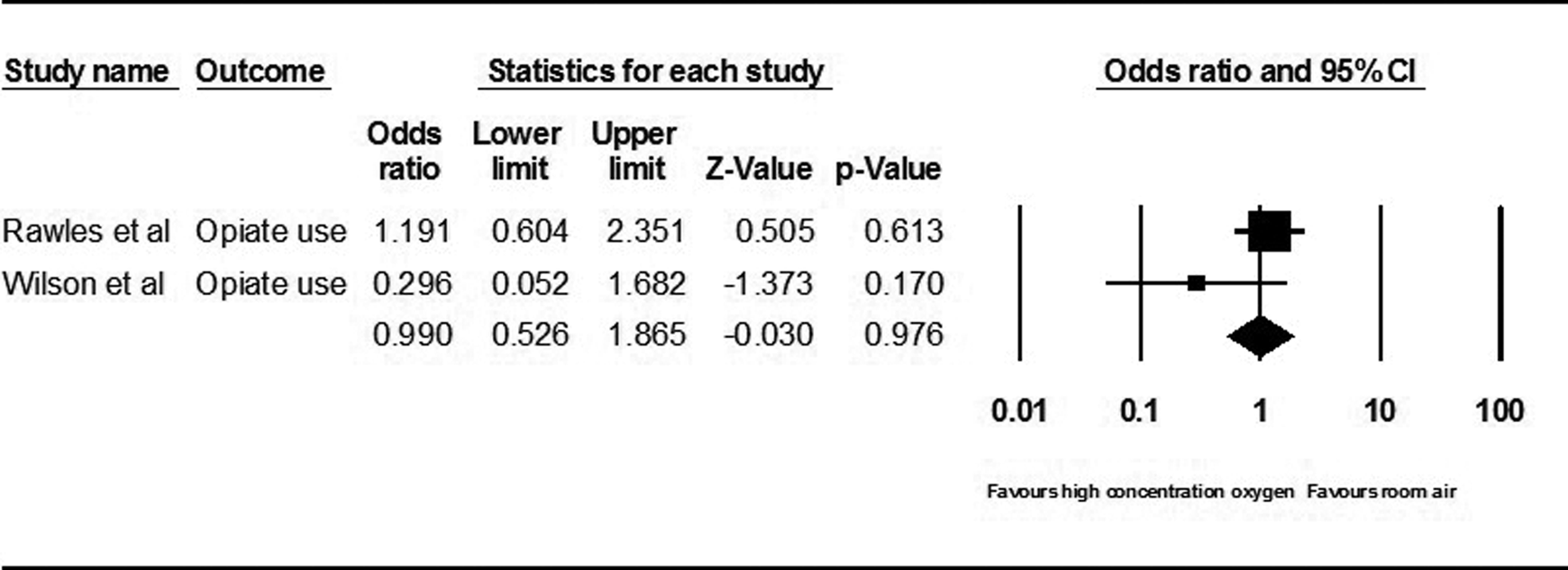
Forest plot comparing opiate use.
Infarction Percentage by MRI
Two studies were pooled with 286 patients in the high-concentration oxygen group and 291 patients in the titrated oxygen or room air group (Figure 4). A fixed-effects model and random-effects model were used due to ambiguity in the heterogeneity analysis (Q = 2.976, P = .085, I2 = 66%). Chi-square analysis did not demonstrate significant heterogeneity although the I2 test did. A significant difference was noted between the 2 groups (mean difference 2.224%, 95% confidence interval 0.906-3.541). When the analysis was repeated with a random-effects model this became insignificant.
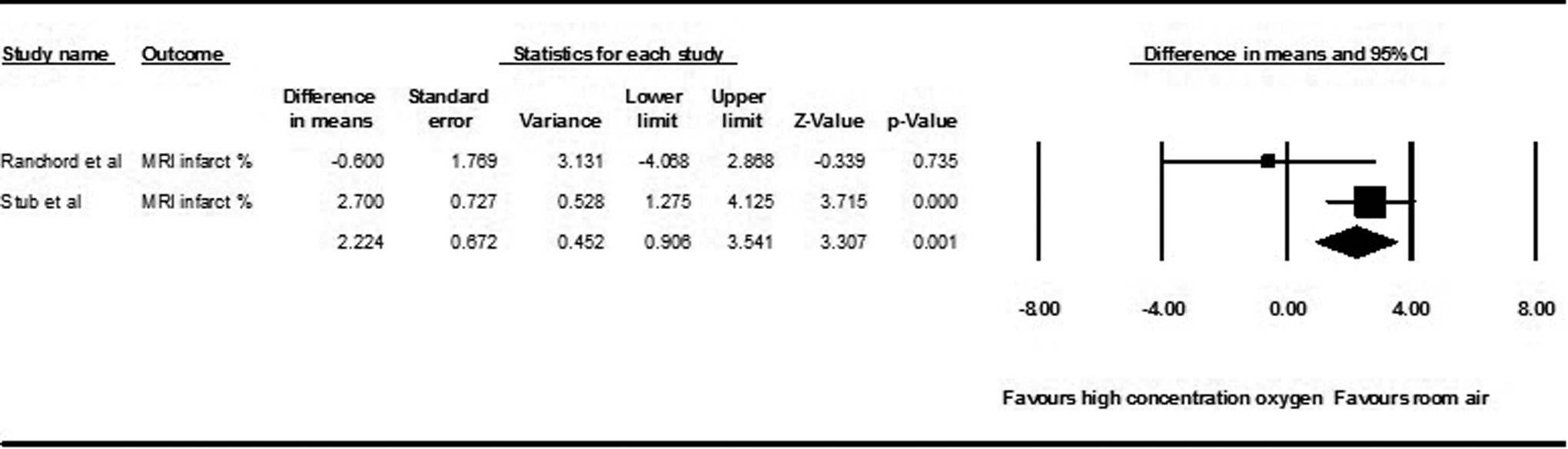
Forest plot comparing percentage of infarcted myocardium by magnetic resonance imaging.
Infarction Mass by MRI
Two studies were pooled with 286 patients in the high concentration oxygen group and 291 patients in the titrated oxygen or room air group (Figure 5). A random-effects model was used as significant heterogeneity was present (Q = 4.552, P = .033, I2 = 78%). A significant difference was not noted between the 2 groups (mean difference 2.418 g, 95% confidence interval −1.960-6.797).

Forest plot comparing mass of infarcted myocardium by magnetic resonance imaging.
Bias Assessment
No studies were excluded from the analysis due to bias as evaluated using the Cochrane Collaboration’s tool for assessing risk of bias (Table 2). Ranchord et al was found to have a high risk of selective reporting as MRI was only performed in a subgroup of patients. 12 This also added to the risk of other bias. Ukholkina et al was found to have a high risk of incomplete outcome data, as there were some significant differences in baseline characteristics. 14 Wilson and Channer were found to have a high risk of selective reporting, as no mortality data were reported. 13
Bias Assessment.

Publication bias was assessed only for in-hospital mortality as the remainder of end points had too few studies. Visual inspection of the funnel plot did not demonstrate significant publication bias, which was confirmed by an Egger test which demonstrated a 95% confidence interval of −9.124 to 10.979 with a P value of .729 (Figure 6).

Funnel plot for in-hospital mortality.
Meta-Regression
A meta-regression was conducted for in-hospital mortality (Table 3). This could not be done for other end points, as there were not an adequate number of studies included. While there was not significant heterogeneity present, age accounted for a majority of the heterogeneity that was present.
Summary Results of Meta-Analysis.
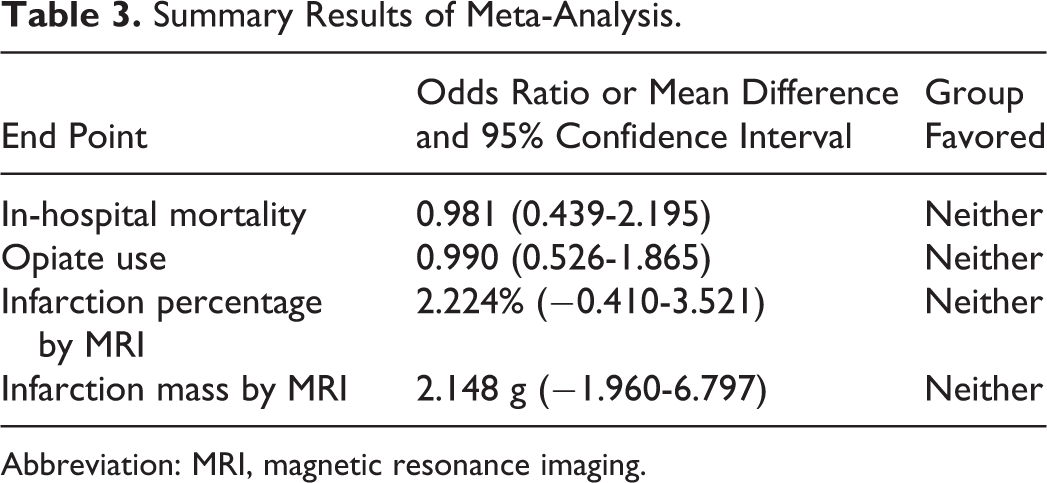
Abbreviation: MRI, magnetic resonance imaging.
Discussion
This analysis of 5 studies demonstrated no difference in in-hospital mortality, opiate use, infarction percentage by MRI, and infarction mass by MRI between those receiving high concentration oxygen and those who received titrated oxygen or room air in the setting of AMI. 11 –15 A significant difference was initially noted in infarction percentage by MRI with a fixed-effects model and when repeated with a random-effects model significance was lost. Thus, there was a trend in greater infarct percentage, but this was found to be statistically insignificant. Such statistically insignificant trends were also found in relation to in-hospital mortality and infarction mass by MRI. These findings are similar to that of a meta-analysis published by Cabello et al in 2013 which had similar findings. We now include recent data, including the largest randomized study to date, to the previous study with similar results. 17
The use of oxygen for a cardiac indication was initially described by Steele in 1900 in the setting of severe angina. 18 In 1930, Levy published a 4 patient case series demonstrating relief of clinical symptoms associated with supplemental oxygen in the setting of AMI, thus introducing the routine recommendation of supplemental oxygen in the setting of AMI. 19 Based on data from animal models, it was hypothesized that supplemental oxygen would help reduce the area of infarction and the risk of arrhythmias, further propagating the use of oxygen in AMI. 20 It was as early as 1950 that studies began to demonstrate that supplemental oxygen may not be beneficial and, in fact, may be associated with some harm. Supplemental oxygen was found to be associated with longer duration of electrocardiographic changes consistent with ischemia and did not have any effect on pain, thought to be secondary to hyperoxia interfering with AMI-induced hyperemia. 21 Subsequent studies demonstrated the hemodynamic effects of supplemental oxygen including a decrease in cardiac output, decrease in cerebral perfusion, decrease in renal perfusion, and increase in systemic vascular resistance. 9,22 –26 Despite these findings, high-concentration oxygen supplementation for AMI continued.
Using the in-hospital mortality from this analysis, a total of 3050 patients with 1525 in each group would be necessary to detect a statistically significant difference of 2% in mortality between the 2 groups with 90% power and an alpha of 0.05. The largest study included in this analysis consisted of 218 patients in the high-concentration oxygen group and 223 patients in the titrated or room air group. 11 This highlights the need for a large randomized effort to evaluate supplemental oxygen in patients with AMI. Such an effort would ideally compare serial electrocardiographic, troponin, and brain natriuretic peptide (BNP) data in addition to the prevalence of arrhythmia and mortality between the 2 groups. The percentage and mass of infarcted myocardium by MRI assessment would also be of great value.
There are limitations of this analysis. Limited number of similar end points for abstraction across included studies limited the number of end points. The BNP levels and troponin levels would have been of interest to assess but these were not available in all studies. Additionally, some of these studies included patients who may have received supplemental oxygen upon initial triage by out-of-hospital responders and while in the ambulance en route to the hospital. They were then subsequently randomized to 1 of the 2 oxygen groups upon hospital arrival. More detailed meta-regression and assessment of publication bias could not be conducted due to the small number of studies for most end points. This analysis is also underpowered. In regard to bias, it is also hard to entirely rule out the possibility of publication analysis, despite the statistical analysis run and thus it can only be said that our analysis implies but does not prove the absence of publication bias.
Conclusion
There were no statistically significant differences noted between those with AMI randomized to high-concentration oxygen or titrated oxygen or room air in respect to in-hospital mortality, opiate use, percentage of infarcted myocardium, or mass of infarcted myocardium.
Footnotes
Author Contribution
R. Loomba and S. Aggarwal contributed to conception and design; acquisition, analysis, and interpretation; drafted the article; critically revised the article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. K. Nijhawan contributed to design, acquisition, and analysis; drafted the article; critically revised the article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. R. Arora contributed to design; acquisition, analysis, and interpretation; drafted the article; critically revised the article; gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Authors’ Note
This article has not been submitted elsewhere for simultaneous consideration of publication and has not been previously published. All the authors have been involved in the conception, execution, and preparation of this article and are aware of its submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.