
Abstract
Background:
Atherothrombosis is the principal mechanism of type 1 (T1) myocardial infarction (MI), while type 2 (T2) MI is typically diagnosed in the presence of triggers (anemia, arrhythmia, etc.). We aimed to evaluate the proportions of T1 vs. T2 MI based on angiographic and clinical definitions, their concordance and prognosis.
Methods:
Consecutive MI patients [n = 712, 61% male; age 64.6 ± 12.3 years] undergoing coronary angiography were classified according to the presence of atherothrombosis and identifiable triggers. Association of angiographic and clinical MI type criteria with adverse outcomes (Time follow-up was 1.5 years) was evaluated. Predictive ability of GRACE risk score for all-cause mortality was then assessed.
Results:
Atherothrombosis and clinical triggers were identified in 397 (55.6%) and 324 (45.5%) subjects, respectively. Only 247 (34.7%) patients had “true” T1MI (atherothrombosis+ / triggers−); 174 (24.4%) were diagnosed with “true” T2MI (atherothrombosis− / triggers+), while 291 (40.9%) had discordant clinical and angiographic characteristics. All-cause mortality in T2MI (20.1%) patients was higher than in T1MI (9.3%), P = 0.002. Presence of triggers [odds ratio (OR) 2.4, 95% CI 1.5-3.6, P < 0.0001] but not atherothrombosis [OR 0.8, 95% confidence interval (CI) 0.5-1.3, P = 0.26] was associated with worse prognosis. GRACE score is a better predictor of death in T1MI vs. T2MI: area under curve 0.893 (95% CI 0.830-0.956) vs 0.748 (95% CI 0.652-0.843), P = 0.013
Conclusion:
Angiographic and clinical definitions of MI type are discordant in a substantial proportion of patients. Clinical triggers are associated with all-cause mortality. Predictive performance of GRACE score is worse in T2MI patients.
Keywords
Introduction
Significant efforts have been devoted to differentiate between myocardial infarction (MI) types, especially regarding type 1 and type 2 MI. However, this issue remains a challenge to physicians in clinical practice. 1 The recent introduction of the fourth Universal Definition of MI (2018) emphasizes the causal relationship of atherosclerotic plaque disruption with coronary atherothrombosis as the principal mechanism for type 1 MI (T1MI), whereas type 2 MI (T2MI) is defined by clinical conditions that cause myocardial oxygen supply and demand imbalance unrelated to coronary atherothrombosis. 2 Coronary angiography (CAG) is the essential tool used to reveal the presence of atherothrombosis, and guide revascularization, but it is less frequently performed in the presence of clinical signs of T2MI being employed only in about a third of such patients. 3 Clinical conditions or triggers leading to myocardial oxygen supply and demand mismatch, like anemia, severe hypertension, arrhythmia, etc. have been used for making the diagnosis of T2MI in multiple studies. 1 However, atherothrombosis and provoking factors may coexist in some patients undergoing CAG. 4,5 T2MI is associated with worse short- and long-term outcomes, compared with T1MI 3,6 -12 and a nearly 1.5-fold increased risk of 2-year mortality according to a recent meta-analysis. 3 However, to date, there are no formal guidelines regarding risk stratification and management of this condition despite its association with poor prognosis. The purpose of this study was to assess the proportions of type 1 vs. type 2 MI in acutely admitted patients based on angiographic and clinical definitions, their concordance and associated prognosis.
Materials and Methods
Our single-center prospective observational cohort study performed at the Vinogradov Moscow city clinical hospital (Moscow, Russia) included consecutive patients aged >18 years admitted with acute MI who underwent CAG <24 hours after symptom onset from January 1, 2017 to December 31, 2018. MI was diagnosed according to the Third universal definition. 13 We analyzed clinical and demographic characteristics, physical examination findings on admission, laboratory and instrumental (ECG, echocardiography, CAG) test results, and medications given during hospitalization and prescribed at discharge. Access 2 Immunoassay System (Beckman Coulter. USA) was used for the measurement of cardiac Troponin I (cTnI) with 99th percentile being 0.02 ng/L. MI was diagnosed if ≥20% increase (with at least 1 value >99th percentile) in troponin was registered between earlier and later samples taken 6 hours apart. Charlson comorbidity index (CCI) 14 with total scores ranging from 0-37 points (higher scores associated with increasing comorbidity burden), was calculated using data available on admission. The TARRACO (Troponin Assessment for Risk stRatification of patients without Acute COronary athero-thrombosis) risk score 15 including such variables as cardiac troponin, age, hypertension, absence of chest pain, dyspnea and anemia, and ranging from 0 to 13 points was also used. GRACE 2.0 (The Global Registry of Acute Coronary Events) risk score were calculated for each admitted patient. 16 In addition, we excluded patients with type 4 and type 5 MI as well as those who developed MI during hospitalization.
Angiographic and Trigger Assessment
Coronary angiography was performed in accordance with conventional protocol and international guidelines. 17 Epicardial coronary artery stenosis ≥50% as assessed by quantitative coronary analysis was considered significant. 18,19 Coronary atherothrombosis was diagnosed as previously described 20,21 in the presence of impaired flow (TIMI grade <3). Cases of complete obstruction of coronary artery with multiple fine collaterals were classified as chronic total occlusions.
Criteria for T2MI triggers were was based on definitions used in previous studies
4,22
-24
: Anemia defined as hemoglobin ≤88.6 g/L for male or ≤80.6 g/L for female patients, or acute gastrointestinal bleeding, or red blood cell transfusion prior to or within 24 hours following the peak serum troponin. Severe hypertension defined as systolic blood pressure (SBP) >180 mmHg or SBP >160 mmHg with concomitant progressive retinopathy and/or encephalopathy and/or pulmonary edema requiring treatment with nitrates or diuretics. Tachyarrhythmia defined as any rhythm disturbance with ventricular rate >150/min excluding sinus tachycardia. Bradyarrhythmia requiring medical treatment or cardiac pacing. Respiratory infection determined by clinical signs (flu-like illness with fever, cough and sore throat) and laboratory tests (increased markers of inflammation) with abnormalities in physical examination of the respiratory system.
We excluded such triggers as hypotension, respiratory failure, and shock because in those cases it was difficult to determine the sequence of clinical events, i.e. whether they occurred before or after MI.
The angiographic evidence of atherothrombosis was considered diagnostic for T1MI. Absence of atherothrombosis and documentation of at least 1 trigger were recognized as signs of T2MI. We classified the patients into 4 groups based on angiographic findings (presence or absence of atherothrombosis) and medical history (presence or absence of identifiable triggers).
Outcomes
Patients were followed up for 1.5 years, and events were recorded at the time of the last patient contact or at the time of a major adverse cardiovascular event.
Outcomes assessed in the study included all-cause in-hospital and long-term mortality, non-fatal recurrent MI, and unplanned cardiac rehospitalization. Of the 712 included patients, 89 (12.5%) were lost to follow-up. Occurrence of cardiovascular events was verified during initial hospital stay (36 patients), by telephone interviews (485 patients) and in-person visits (102 patients).
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 21.0 and MedCalc 14.0 software. Comparisons of categorical variables were performed by Chi-Square and Fisher’s exact test, and between-group differences in continuous variables were assessed using the unpaired Student t-test for normally distributed variables and Mann–Whitney U test for non-normal data. Outcomes were compared between groups using Chi-Square and Fisher’s exact test. Univariate logistic regression was performed to establish the association of angiographic and clinical definitions and individual triggers of MI type with all-cause long-term mortality. We compared the predictive ability of GRACE risk score for long-term mortality by comparing AUCs in ROC curve analysis using the Hanley-McNeil test, with T1MI patients as the reference group. To establish clinical predictors for all-cause long-term mortality in T2MI patients, uni- and multivariate logistic regression then was performed. TARRACO score and Charlson index were also evaluated in T2MI patients for prediction of all-cause mortality and compared to GRACE score by evaluation of AUCs and Hanley-McNeil test. For continuous variables, receiver operating characteristic (ROC) curve analysis was performed to find the optimal cut-off value for regression model. Odds ratio (OR), 95% confidence interval (CI), and P values are presented for each independent predictor of the negative outcome. P-values <0.05 were considered significant.
Results
In total, 712 consecutive patients [median age 65 (IQR, 56-74) years, 39% male] with acute MI were included in the study. Baseline patient characteristics are shown in Table 1.
Baseline Demographic and Clinical Characteristics of Study Population.

Abbreviations: MI, myocardial infarction; CAD, coronary artery disease; TIA, transient ischemic attack; COPD, chronic obstructive pulmonary disease; BP, blood pressure; EF, ejection fraction; PCI, percutaneous coronary intervention.
For continuous variables median (interquartile range) is given. For binary ones absolute and relative frequencies are shown. * P < 0.05 for comparisons with Type 1 MI; ≠ P < 0.05 for comparisons with Type 2 MI; ┼ P < 0.05 for comparisons between groups Type 1MI with triggers and MI without atherothrombosis and triggers.
Atherothrombosis was present in 397 (55.6%) of the study patients, and clinical triggers of MI were identified in 324 (45.5%) subjects, of which the most common were severe hypertension—177 (54.6%) patients, paroxysmal tachyarrhythmia—97 (29.9%) patients, and anemia—60 (20.4%) patients. Based on the MI definition by clinical features (triggers) and the presence of atherothrombosis, there were 4 phenotypes of MI were classified: T1MI, which had atherothrombosis and triggers were absent, accounted for 247 (34.7%) patients. T2MI, which had at least 1 trigger and atherothrombosis was absent, accounted for 174 (24.4%) patients. And another 2 MI phenotypes: T1MI with triggers, accounted for 150 (21.1%) patients and MI without triggers and atherothrombosis, accounted for 141 (19.8%) patients (Table 2). This means that angiographic data contradicted the clinical definition of MI type in 291 (40.9%) patients. These groups are compared in Table 1.
Angiographic and Clinical Correlates of MI Type.

Abbreviation: MI, myocardial infarction.
For binary ones absolute and/or relative frequencies are shown.
Patients with T2MI presented less often with chest pain [154 (88.5%) vs. 240 (97.2%), P < 0.001], and more frequently had dyspnea [48 (27.6%) vs. 22 (8.9%), P < 0.001]. T2MI was characterized by lower troponin values [0.25 (IQR 0.09-1.24) vs. 0.73 ng/mL (IQR, 0.08-7.75), P = 0.002], lower hemoglobin [131 (IQR 111-142) vs. 142 g/L (IQR, 132-150), P < 0.001] and higher creatinine level [97.5 (IQR 83-115) vs. 90 (IQR, 78-104) µmol/L, P = 0.001]. Significant coronary stenosis [136 (78.1%) vs. 247 (100%), P < 0.001], and three-vessel disease [92 (52.9%) vs. 139 (56.3%), P < 0.001] were less prevalent in T2MI subjects, of which fewer underwent percutaneous coronary intervention (PCI) [104 (59.4%) vs. 237 (96%), P < 0.001] compared with T1MI. There was not statistically difference of PCI rates among T1MI and T1MI with triggers patients) [145 (96.7%) vs. 237 (96%), P = 0.793, respectively]. MI with non-obstructive coronary arteries was diagnosed in 38 (21.8%) patients with T2MI.
In hospital, T2MI patients were more often managed with nitrates [31 (17.8%) vs. 20 (8.1%), P = 0.004], diuretics [89 (51.1%) vs. 75 (30.4%), P = 0.004], and inotropes [7 (4%) vs. 4 (1.6%), P = 0.004] compared with T1MI. At discharge, however, they were less frequently prescribed antiplatelet therapy (i.e. aspirin [140 (86.2%) vs. 241 (97.6%), P < 0.001], P2Y12 inhibitors [159 (91.4%) vs. 240 (97.2%), P = 0.013]) and statins [159 (91.4%) vs. 238 (96.4%), P = 0.034], although treatment with diuretics [78 (44.8%) vs. 71 (28.7%), P = 0.001] and anticoagulants [24 (13.8%) vs. 9 (3.6%), P < 0.001] was more common (Supplemental Table 1).
During hospitalization 36 (5.1%) patients died; moreover, in-hospital mortality in T2MI [12 (6.9%)] and TIMI with triggers [16 (10.7%)] patients was higher than in those with T1MI [6 (2.4%)], P = 0.03 and 0.001, respectively. After long-term follow-up, all-cause death was twice as frequent in T2MI than in T1MI patients [35 (20.1%) vs. 23 (9.3%), P = 0.002, respectively] and was also higher in the group of TIMI with triggers [20 (13.3%), P = 0.03]. Recurrent MI rate was similar [8 (4.6%) for T2MI, 6 (4.0%) in TIMI with triggers, and 10 (7.1%) in MI without triggers and atherothrombosis vs. 11 (4.5%) for T1MI] between groups and cardiac re-hospitalization occurred more often in T2MI patients compared with T1MI [41 (23.6%) vs. 37 (15%), P = 0.03]. Cardiac re-hospitalization was similar between T1MI patients with triggers and T2MI patients [34 (22.7%) vs. 41 (23.6%) P = 0.89]. There were no statistically significant differences between group of MI without triggers and atherothrombosis and T1MI with respect to all studied end points (Figure 1).

Adverse cardiovascular outcomes in study groups. P value were obtained from groupwise comparisons using χ2 test with type 1 myocardial infarction as the reference group. MI: myocardial infarction. MI: myocardial infarction. Group type 1 MI with triggers: patients with diagnosed atherothrombosis and at least 1 trigger. Group MI without atherothrombosis and triggers: patients without neither atherothrombosis nor clinical triggers.
In logistic regression analysis, three-vessel coronary artery disease (OR 1.6, 95% CI 1.1-2.2, P = 0.011), but not atherothrombosis (OR 0.8, 95% CI 0.5-1.3, P = 0.26) was associated with all-cause death. However, the presence of any trigger (OR 2.4, 95% CI 1.5-3.6, P < 0.0001), including anemia (OR 4.5, 95% CI 2.6-8.0, P < 0.001), paroxysmal tachyarrhythmia (OR 1.8, 95% CI 1.0-3.2, P = 0.037), bradyarrhythmia (OR 3.2, 95% CI 1.3-7.9, P = 0.013), respiratory infection (OR 3.2, 95% CI 1.5-6.8, P = 0.002) predicted long-term mortality (Table 3).
Angiographic and Clinical Predictors of All-Cause Long-Term Mortality.
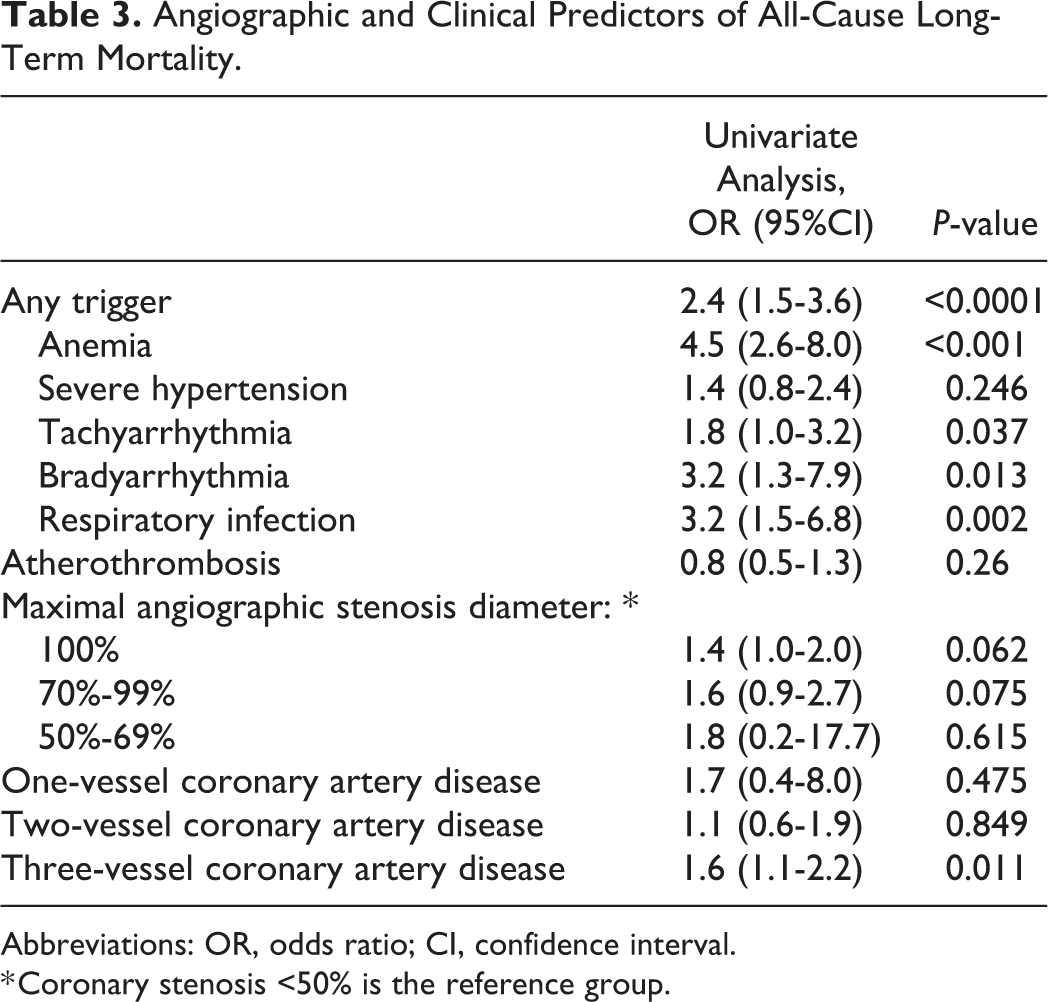
Abbreviations: OR, odds ratio; CI, confidence interval.
* Coronary stenosis <50% is the reference group.
The ROC curves of the GRACE score for all-cause long-term mortality prediction in all groups are shown in Figure 2. GRACE score is a better predictor of all-cause death in T1MI patients compared to those with T2MI: AUC 0.893 (95% CI 0.830-0.956) vs 0.748 (95% CI 0.652-0.843), P = 0.013.
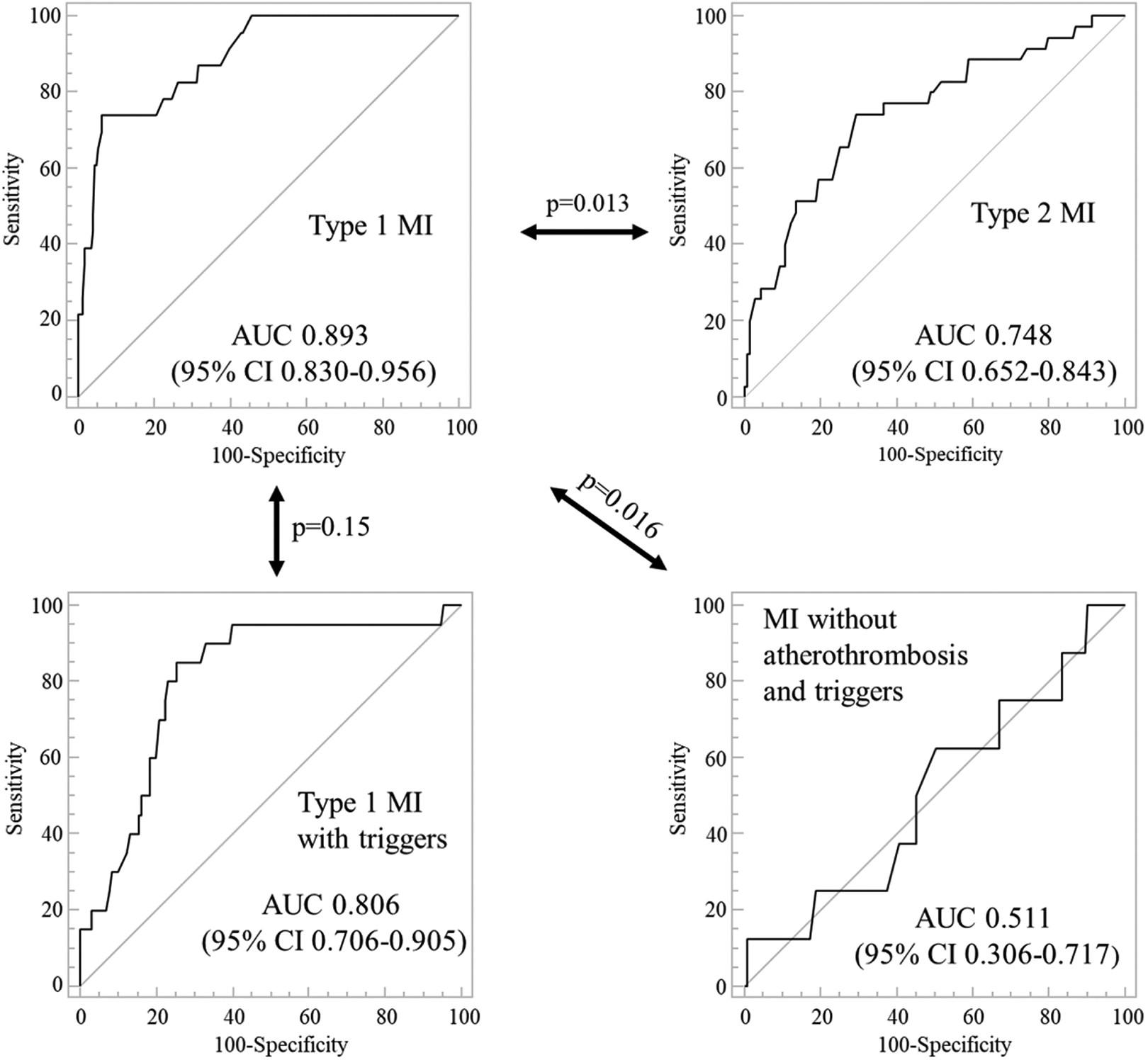
GRACE score performance for long-term all-cause mortality prediction. Comparisons of areas under the curve (AUCs) was performed using Hanley-McNeil test with T1MI patients serving as the reference group. MI: myocardial infarction. CI: confidence interval.
Median GRACE, TARRACO scores and Charlson comorbidity index values in T2MI patients were 126 (IQR, 100-149), 4 (IQR, 3-6), and 5 (IQR, 3-6) points, respectively. In ROC curve analysis, TARRACO score (AUC 0.741, 95% CI 0.669-0.805) and the Charlson comorbidity index (AUC 0.786, 95% CI 0.717-0.844) demonstrated good predictive ability for all-cause mortality, although it was similar to that of GRACE risk score (P = 0.89 and 0.34, respectively) (Figure 3).

Receiver-operating-characteristic (ROC) curves of the GRACE, TARRACO scores and Charlson comorbidity index to predict all-cause long-term mortality in T2MI patients. TARRACO risk score: Troponin Assessment for Risk stRatification of patients without Acute COronary athero-thrombosis risk score. Charlson: Charlson comorbidity index. GRACE risk score: Global Registry of Acute Coronary Events (GRACE) risk score.
Uni- and multivariate analysis of factors associated with all-cause mortality in T2MI are shown in (Supplemental Table 2). Presence of anemia (OR 5.7, 95% CI 1.5-21.9, P = 0.012), higher Charlson Index (OR 6.3, 95% CI 1.1-35.4, P = 0.035), presence of ST-elevation (OR 6.7, 95% CI 1.7-26.4, P = 0.007), and history of previous MI (OR 8.0, 95% CI 1.3-48.5, P = 0.024) were associated with an increased risk of death in such patients.
Univariate logistic regression analysis of clinical impact of early myocardial revascularization on outcomes of different MI phenotypes revealed that PCI within 24 h after symptom onset was associated with lower cardiovascular rehospitalization in patients with T2MI (OR 0.4, 95% CI 0.2-0.9, P = 0.019), and MI without triggers and atherothrombosis (OR 0.4, 95% CI 0.1-0.8, P = 0.014). However, similar results and for in-hospital and mortalities within 1.5 years were not observed in all MI phenotype patients (Table 4).
The Clinical Impact of Percutaneous Coronary Intervention on Outcomes of Different MI Phenotypes in Univariate Analysis.

Abbreviations: OR, Odds ratio; 95% CI, confidence interval; MI, myocardial infarction.
Assessment of the effect of percutaneous coronary intervention on outcomes of different MI phenotypes by using univariate analysis with OR and 95% CI.
Discussion
The primary finding of our study is that 40.9% of MI patients had discrepant angiographic and clinical definitions of MI type, which means that 21.1% of MI patients with clinical signs characteristic of T2MI also demonstrated acute atherosclerotic plaque rupture by CAG and 19.8% of MI patients without any apparent triggers had no atherothrombosis on CAG, which makes the determination of MI type quite complicated. Similar to our result, in the study by Landes et al, 4 which included 107 patients with T2MI diagnosis, acute plaque rupture which is the hallmark of T1MI was detected in 29% of patients who underwent CAG, although this procedure was performed only in 29 (27.1%) of study participants. That means that angiographic and clinical definitions of T2MI may coexist in some cases. In the CASABLANCA study (Catheter Sampled Blood Archive in Cardiovascular Diseases) 5 that enrolled 1251 patients undergoing coronary or peripheral angiography, who were prospectively followed for 40 months, 152 patients had at least 1 incident T2MI, of which 21 (13,8%) patients subsequently developed T1MI. Therefore, signs of unstable plaque during CAG in addition to clinical definitions of MI type could play an important additional role in differentiation between T2MI and T1MI. Since the diagnosis of T2MI is often based on physician judgment, it is possible that some patients classified as having T2MI actually have T1MI. Therefore, demonstration of unstable plaque signs during CAG could play an important additional role in differentiation between T2MI and T1MI leading to correct diagnosis in this population.
To the best of our knowledge, this study was first to use CAG in all included patients which in combination with clinical definitions of myocardial oxygen supply/demand mismatch allowed to confirm “true” T1MI and T2MI in 21.1% and 24.4% of patients, respectively. The prevalence of T2MI among all patients with MI has been reported to be between 1.6% and 74.2%, 1,25 -28 depending on criteria used. For example, by using cut-off values for conditions leading to oxygen supply/demand imbalance similar to our study, Saaby et al 22 estimated the prevalence of T2MI at 26% (144 out of 553 patients with T2MI and T1MI) of MI cases. Notably, CAG was again performed only in 31 (21.5%) T2MI patients. Some other studies classified T2MI according to clinical judgment, and have not specified thresholds for triggers, like anemia or tachyarrhythmia. 9,24,27,29
Patients with T2MI were less often treated with antiplatelet therapy and statins, but more frequently prescribed with nitrates, diuretics and anticoagulant therapy, which probably reflects the higher prevalence of heart failure and tachyarrhythmia in this group. The lower rate of prescribed antiplatelet and statin therapy is consistent with previous studies, 30 -32 and the higher rate of diuretic and anticoagulant treatment at discharge is partially concordant with the findings of the study by Baron et al. 26 The differences in patient management between studies may be attributed to the lack of evidence-based treatment guidelines for patients with T2MI.
In our study, all-cause in-hospital and long-term mortality rates were higher in T2MI compared to T1MI patients. These findings are in line with published literature. 6 -12,33 -35 For example, a retrospective study by El-Haddad et al 36 included 807 patients with abnormal troponin levels over a 1-year period, of whom 512 (63.4%) had T1MI and 295 (36.6%) had T2MI, and showed higher in-hospital mortality in T2MI patients compared with T1MI cases (28.5% vs 5.5%). This means that patients with T2MI were 6.9 times more likely to die than those with T1MI (P < 0.001). Such difference in mortality rate can be explained by exclusion of patients with T2MI who underwent PCI and a high prevalence of comorbidities in this population. The similar rate of recurrent MI between patients with T1MI and T2MI is consistent with previous studies, 10,11 but contradicts the data from the recent meta-analysis, 3 which showed significantly higher risk of reinfarction with a mean follow-up time of 1.6 years in T2MI patients (risk ratio (RR): 1.68, CI 1.22-2.31, P = 0.001). This may explain by relatively higher rate of PCI use in T2MI patients in our study that may be associated with more favorable prognosis. In our study, cardiovascular rehospitalization rate was higher in T2MI patients compared with T1MI. Neumann et al 37 reported higher rate of cardiac re-hospitalization among patients with T1MI (33.8% vs 19.3%, P = 0.025) within 1 year after admission compared with T2MI, although after adjustment for age, sex and presence of coronary artery disease (CAD) this difference was not significant.
Similarly, the SWEDEHEART registry (Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies) 26 that included 19763 MI patients showed a higher 1-year mortality [hazard ratio (HR) 1.86; 95% CI 1.66-2.08] in T2MI versus T1MI subjects. However, after adjustment for background characteristics and treatment, this risk was no longer significant [hazard ratio (HR) 1.03, 95% CI 0.86-1.23]. In the study by Chapman et al, 10 which enrolled 2165 consecutive patients with troponin elevation, increase in 5-year mortality was attenuated, but remained significant (RR 1.51, 95% CI 1.21-1.87) after adjustment for age, sex, hypertension, diabetes, smoking, CAD, stroke, PAD, renal function, and hemoglobin values.
PCI was performed in 60% patients with T2MI in our study, compared to those with TIMI (96%), and higher than the result from recent meta-analysis, 3 showing a PCI use rate of 40% (range 0% to 87.5%). PCI was not reduced in-hospital and long-term mortalities in patients with T1MI and TIM1 with triggers in this study could be explained by high rates of performed PCI and small sample of these patient groups. For T2MI patients, PCI was not reduced in-hospital mortality that was consistent with the results from the study by Higuchi et al, 32 including 12023 T1MI and 491 T2MI patients (with CAG and PCI rates were 95% and 77% in T1MI, 87% and 53% in T2MI respectively), in which PCI was associated with lower in-hospital mortality in T1MI (OR 0.47; 95% CI 0.40-0.55; P < 0.001), but not in those with T2MI (OR 1.09; 95% CI 0.62-1.94; P = 0.763). The benefits of PCI reduced cardiovascular rehospitalization in T2MI can be explained by predominance of CAD in this study. However, the purposes of this study were not to assess the efficacy of PCI strategy in T2MI patients, that is going on the ACT-2 trial 38 to investigate the prevalence of CAD and the effect of intervention on clinical outcomes. The benefits of PCI in ACS patients have been demonstrated in most studies, that were included in the guidelines from European Society of Cardiology 39,40 and the American College of Cardiology/American Heart Association, 41 however, its’ short- and long-term impacts on clinical outcomes in T1MI and especially in T1MI with triggers patients, compared to those with evidence-based medical therapy have been absent and require further studies to clarify it. 42,43 Additionally, with the effects of triggers and comorbidity for long-term mortality in T2MI patients, discrepancy in medication systems at discharge between T1MI and T2MI with different clinical outcomes, appropriate approaches in the future in these directions should be considered to study T2MI patients. 42
While risk stratification tools are well established for T1MI 39,40 ; few compelling data exist for T2MI patients. The performance of GRACE risk score in T2MI group was comparable with the TARRACO risk score, developed by Celdiel et al 15 in cohort of patients admitted to the emergency department who underwent cTnI measurement. Notably, T2MI was diagnosed using specific criteria proposed by Saaby et al 22 similar to our study. This score performed well in prediction of death or cardiac re-hospitalization at 180 days in T2MI patients (AUC 0.75, 95% CI 0.67-0.83). Additionally, Charlson comorbidity index and presence of ST elevation were associated with all-cause mortality in our study. Clinical predictors previously associated with poor prognosis in T2MI patients include older age, 36 shock, 31 presence of CAD, 10,33 heart failure. 6
In a recent study by Murphy et al, 44 the authors sought to compare the performance of the GRACE, TIMI, and TARRACO scores in patients with T2MI. The authors revealed that the GRACE score predicted all-cause mortality (AUC was 0.66 for in-hospital mortality and 0.70 for 90-day mortality), while the remaining 2 scores were not useful. The modest predictive performance of GRACE score for all-cause mortality was in line with results of our study and may be due to comorbidity burden and older age of T2MI patients, while T1MI group of our study was similar to MI cohorts from which the GRACE score was derived. 45,46
Demonstration of worse GRACE risk score performance in T2MI patients warrant further studies of risk stratification in this patient population to examine the impact of candidate predictors, for example, Charlson index, or anemia that could be incorporated into GRACE model. Association of the presence of identifiable triggers with worse prognosis suggests that treatment of the primary cause of myocardial oxygen supply and demand imbalance is paramount. It also means that both angiographic and clinical definitions of MI type play an essential role in MI classification and therefore decision-making regarding further management strategy. Comparison between angiographic and clinical signs of MI type may help further development and clinical adaptation of the internationally accepted definition for T2MI.
Limitations
First, the enrolment of patients was limited to the cardiac care unit; therefore, it is difficult to characterize the whole population of T2MI patients, some of whom may be primarily hospitalized for another reason and develop MI during hospital stay. Second, although CAG was performed in all patients, finding coronary plaque rupture or small thrombus depends on experience of interventional cardiologist. Specificity of CAG for atherothombosis is high, but its lacks sensitivity for some morphological characteristics, for example intraluminal staining or coronary filling defects. 47 Therefore, the absence of using intravascular coronary imaging like optical coherence tomography or intravascular ultrasound in this study is a disadvantage and may lead to potential misclassification of MI type in some patients.
Conclusions
Angiographic and clinical definitions of MI type are discordant in a substantial proportion of patients. There was a discrepancy of medical managements in patients with type 2 MI when compared with type 1 MI. Presence of identifiable triggers of type 2 MI predicts all-cause death. The predictive performance of GRACE risk score for long-term mortality is worse in T2MI patients.
Supplemental Material
Supplemental Material, sj-docx-1-cpt-10.1177_10742484211005929 - Concordance and Prognostic Relevance of Angiographic and Clinical Definitions of Myocardial Infarction Type
Supplemental Material, sj-docx-1-cpt-10.1177_10742484211005929 for Concordance and Prognostic Relevance of Angiographic and Clinical Definitions of Myocardial Infarction Type by Truong H. Hoang, Pavel V. Lazarev, Victor V. Maiskov, Imad A. Merai and Zhanna D. Kobalava in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Author Contributions
ZhDK is the principal investigator, performed research, and coordinated the study. THH and PVL drafted the manuscript. THH, PVL, VVM, IAM, and ZhDK coordinated the study. THH collected data. THH, PVL, VVM, IAM, and ZhDK contributed to the analysis and interpretation of the data. PVL and ZhDK edited the manuscript. THH and PVL did the statistical analysis. PVL, VVM, IAM, and ZhDK were involved in organization, coordination, conduct, and technical support of the study. ZhDK was involved in organization of research and the final decision to publish. All authors critically reviewed the manuscript and approved the final version. All authors had full access to all data in the studies and had final responsibility for the decision to submit for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.