
Abstract
Objectives
Adolescents and young adults (AYAs) with cancer often experience educational and vocational challenges that hinder long-term developmental goals and milestones. While more attention has been paid to addressing employment-related needs, little research has focused on identifying and addressing educational needs during or after treatment for AYAs with cancer, particularly younger AYAs, who rely on caregivers for educational support and guidance. We report our process for developing and refining an educational guidance session for caregivers of AYAs with cancer.
Methods
Guided by an extended Social Determinants of Health framework, we developed a standardized process to identify and address educational needs reported by caregivers of AYAs with cancer. Key stakeholders were consulted at multiple stages of development, and the process included a prescreening tool, guidance session, and curated resource list. During beta testing, formative guidance sessions were conducted with caregivers, followed by one- and three-month follow-up check-ins to collect feedback and refine the intervention.
Results
During beta testing, we pre-screened caregivers of 16 AYAs (ages 12–20 years; M = 16.31; SD = 2.18). Thirteen caregivers screened positive and were eligible for the guided session; 11 reported their AYA had unmet educational needs. Reported concerns were clustered into three domains: school enrollment, learning support, and school-related financial barriers. Most participants reported sessions were helpful and appreciated personalized resources. Preferences varied by depth and frequency of support, underscoring the need for flexibility in delivery and resulted in a standard, yet tailorable slide for future guidance sessions.
Conclusion
This caregiver- and patient-informed intervention addresses a critical gap in AYA cancer care by identifying and responding to educational needs. The structured guidance model is more inclusive of educational needs specific to younger AYAs and caregiver support and thus integrated as a component of an AYA needs navigation program (AYA-NAV).
Plain Language Summary
Adolescents and young adults with cancer often experience major disruptions to their education and work during and after treatment. These challenges can affect their emotional well-being, independence, and quality of life, yet support for navigating school and job-related needs is often limited. This study describes the development of educational guidance sessions designed to help young people with cancer and their caregivers identify and address education- and work-related challenges. The program includes a brief screening to identify needs, structured guidance sessions with a trained navigator, and tailored resources to support school and employment goals. Feedback from young people with cancer, caregivers, and other stakeholders was used to refine the program so that it is practical, relevant, and responsive to their needs. Although a pilot study is currently underway to examine how feasible and acceptable the program is in a clinical setting, this paper focuses on how the program was developed and refined. This work aims to improve access to educational and vocational support for young people with cancer and their families.
Keywords
Introduction
Adolescents and young adults (AYAs) with cancer often experience disruptions in educational and vocational trajectories during and after treatment. Hospitalizations, treatment schedules, treatment-related toxicities, and prolonged absences from school can interfere with academic engagement and continuity.1,2 Emotional distress, including depression and anxiety, may further affect school attendance and engagement. 3 In addition, cancer- or treatment-related physical and cognitive effects can shape a young person’s ability to participate in educational activities and influence long-term educational and vocational goals.4,5 These challenges are particularly consequential during adolescence and emerging adulthood, a developmental period characterized by increasing autonomy and key educational transitions that influence long-term vocational opportunities.6-8
Education and employment are important social determinants of health, shaping long-term socioeconomic stability, access to healthcare resources, and quality of life. These factors are recognized within the World Health Organizations (WHO’s) Social Determinants of Health (SDOH) framework, 9 which highlights how nonmedical related factors such as social and economic factors influence health outcomes. 9 Within this framework, disruptions to educational and vocational attainment function as intermediary determinants of health and may have implications beyond academic achievement, contributing to longer-term financial and health inequities. Prior work has documented substantial educational and vocational needs among pediatric and AYA oncology populations. Studies involving AYAs with cancer have reported difficulties maintaining employment or school engagement during or after treatment,10-12 while pediatric oncology research has identified unmet educational needs reported by caregivers of children with cancer, including challenges navigating educational accommodations and academic supports.1,13,14 Together, these findings highlight the importance of addressing educational needs as part of comprehensive AYA cancer care in pediatric oncology.
Several tools exist to identify school-related concerns among pediatric and AYA populations, including school needs inventories and broader quality-of-life assessments that include school functioning domains.10,15-17 One such tool, the Brief School Needs Inventory (BSNI), assesses school-related needs among medically complex pediatric populations, including academic performance, attendance, educational accommodations, and communication between families and schools.18,19 However, standardized approaches for identifying then addressing educational needs among AYAs with cancer remain limited. Burns et al. conducted a systematic review that found limited adherence to Psychosocial Standards of Care criteria among existing educational support interventions in pediatric oncology and emphasized the need for more comprehensive programs, including greater caregiver involvement. 20 Existing interventions have largely focused on supporting employment among adult cancer survivors or on AYA-directed programs addressing vocational planning or school re-entry.7,21-23 One such example from Australia has used intervention mapping to develop programs addressing educational and vocational needs among AYAs with cancer (i.e., the Educational and Vocational Support Program (EVSP) and Education and Career Support (ECS) programs).24,25 These interventions, however, primarily target AYAs themselves, and few incorporate caregivers as active partners in addressing educational challenges.
Caregivers often play a central role in supporting AYAs with cancer, providing emotional, informational, and practical support throughout treatment and survivorship.16,26,27 Caregivers may also act as advocates when navigating healthcare, school systems, and employment-related issues.27-29 Research in pediatric oncology demonstrates that caregivers are critical to coordinating school reintegration and educational accommodations12,30; however, relatively little work has focused on caregiver-informed strategies to support educational and vocational navigation for younger AYAs with cancer.
Guided by the Social Determinants of Health (SDOH) framework and its application to AYA cancer care,9,31,32 this manuscript describes the stakeholder-informed development and beta testing of a structured educational guidance session designed for caregivers of younger AYAs with cancer. The goal of this work was to develop a feasible and relevant intervention component to identify and address educational needs during treatment. We describe the iterative development process, including stakeholder engagement and refinements made during early implementation within a caregiver needs navigation study. Because most participating AYAs were in middle or high school, the current paper focuses primarily on educational guidance for caregivers of younger AYAs.
Methods
Study Context and Design
This study describes the development and early refinement following beta testing of the educational and vocational component of a broader needs navigation intervention for AYAs with cancer, AYA-NAV.33,34 We report on the structured process designed to identify educational and vocational needs and deliver tailored guidance sessions for AYA patients and caregivers. As this intervention is currently being piloted, formal outcome measures are not reported here; instead, this manuscript focuses on describing the intervention development process and early refinements informed by initial beta testing.
This study was approved by the Institutional Review Board at a large academic medical center in the Northeastern United States (IRB; #AAAU9477; initial approval granted 2/9/24; ClinicalTrials.gov #: NCT06296641). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional review board and the Declaration of Helsinki (1975), as revised in 2024. Informed consent was obtained from all participants that enrolled in the beta testing phase prior to participation. The data underlying this article will be shared upon reasonable request to the corresponding author. This study was reported in accordance with the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidelines, where applicable. Findings from this study will be disseminated through peer-reviewed publications and presentations at scientific conferences.
Setting
This study was conducted in a large, academic medical center in Northern New York City that serves a socioeconomically and ethnically diverse patient population. 35 This intervention development grew from formative research conducted by a nurse researcher (MPB) that aims to address unmet health-related social needs for AYAs with cancer (NCT06072833). As described below, a critical unmet need – educational needs – were observed among caregiver participants of eligible AYAs; thus, this study centers on the outpatient pediatric oncology clinic at the medical center.
Intervention Development Overview
Stages of AYA-NAV Guidance Session Development, Beta Testing, and Refinement
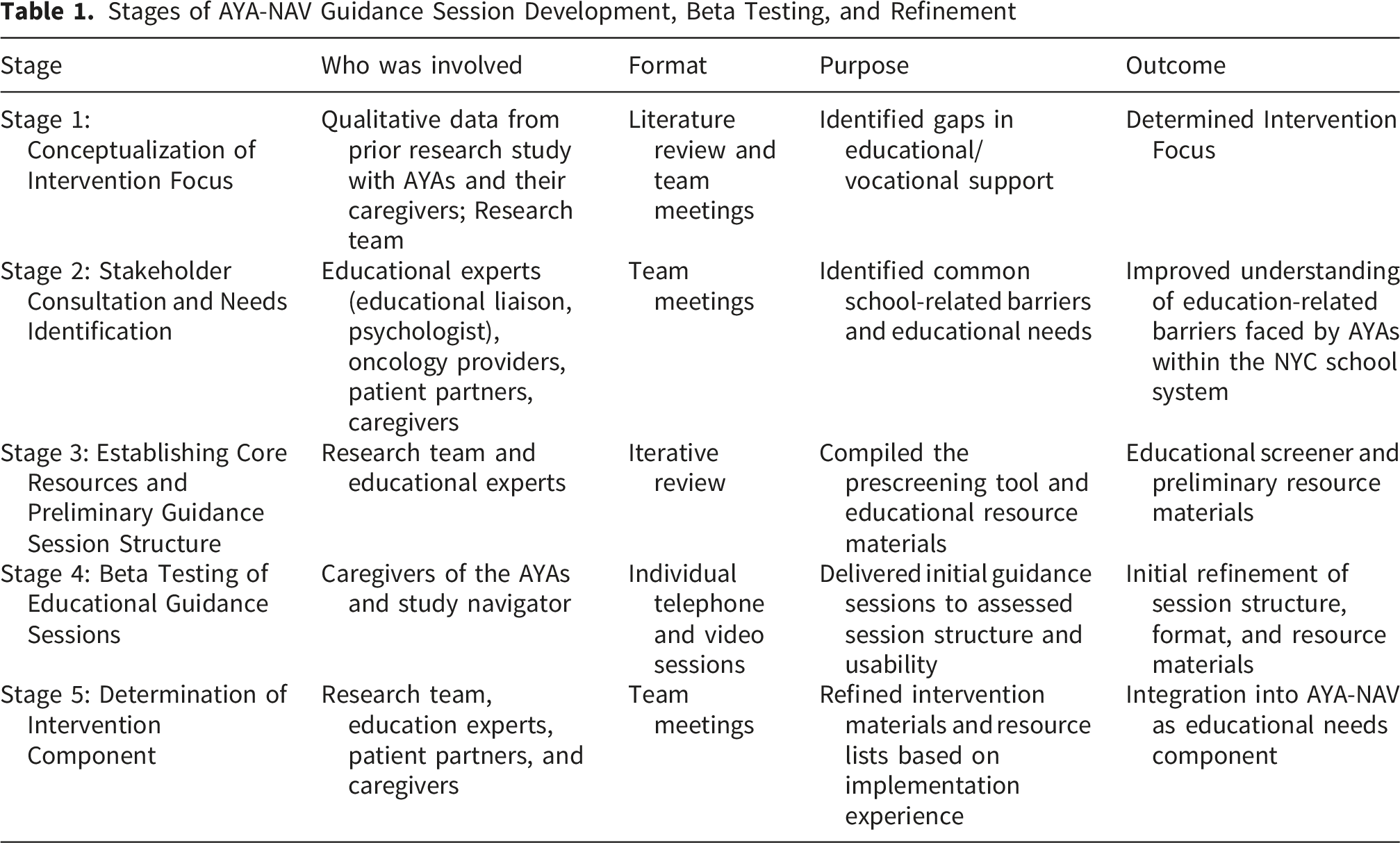
Conceptualization of Intervention Focus
The initial stage focused on conceptualizing the educational guidance component within the broader AYA-NAV needs-navigation intervention, which was developed and piloted by the research team. 33 The need for targeted educational guidance as a core component of an intervention addressing unmet health-related needs emerged during formative development of AYA-NAV.29,34 The predecessor study included AYAs who spoke English or Spanish and were aged 15–39. In these earlier studies, younger participants and their caregivers more frequently reported unmet educational needs during qualitative interviews or navigation sessions, and these needs were not explicitly addressed in the AYA-NAV intervention model. 34 These observations, together with prior literature documenting educational disruptions among pediatric and AYA oncology populations, highlighted the importance of developing a structured approach to identify and address educational needs among AYAs with cancer.
Because of the focus on educational needs specifically, this study focused on the pediatric oncology setting and included adolescents and emerging adults aged 12–26. Given the known educational needs both in pediatric and AYA populations, including younger adolescents was justified to facilitate earlier identification of these needs in the cancer trajectory, when school reintegration and developmental transitions are actively occurring. Because of the role caregivers play in navigating educational systems and coordinating school accommodations and from our prior qualitative study supporting the involvement of caregivers for younger AYAs, the intervention was designed for caregivers to serve as the primary participants in the guidance process.
Members of the research team, including the principal investigator, pediatric psychologist, educational liaison, research coordinator, and bilingual study navigator, met through a series of planning meetings. The study team reviewed the literature and data from our prior AYA-NAV research studies to review educational support needs and to determine how these needs could be addressed through a structured educational guidance intervention. As the AYA-NAV intervention development was guided by our adapted WHO Social Determinants of Health framework, this framework was applied as it conceptualizes education and vocational attainment as intermediary determinants that may influence long-term health and socioeconomic outcomes.
Stakeholder Consultation and Needs Identification
Given the lack of evidence-based interventions addressing educational and vocational needs among AYAs with cancer, 8 this formative consultation process was used to guide the development of a feasible standardized screening and intervention framework for integrating educational guidance into clinical care. The next step in developing our educational guidance intervention was through iterative, stakeholder discussions within and outside the institution. Stakeholders were defined as individuals with clinical or educational experience relevant to AYAs with cancer, AYA cancer survivors, or caregivers of AYAs. These individuals were identified through our multidisciplinary team’s networks, and included patients, caregivers, and representatives from community organizations to provide feedback and inform refinements to the AYA-NAV intervention, including specific input on developing this component. All stakeholders were informed that participation was voluntary and that they were not required to respond to any questions they did not feel comfortable answering. Stakeholder input was gathered through structured discussions both individually and with a group on a virtual meeting to identify common educational challenges faced by AYAs with cancer and barriers to accessing school-based supports. We assessed current practices in identifying and addressing educational needs among AYAs, including considerations related to navigating the New York City Department of Education system, where the broader navigation intervention had been developed and planned for further testing. These discussions facilitated a deeper understanding of the complexity of educational support needs for this population from diverse perspectives, identify gaps in the preliminary conceptualization of the educational guidance sessions, and informed the development of the intervention framework.
Establishing Core Resources and Preliminary Guidance Session Structure
Following stakeholder discussions to inform the framework for development of the educational component, the study team (principal investigator, navigator, research coordinator, educational liaison, clinical psychologist, and patient advocate partners) met sequentially to adapt the pre-screening questionnaire and collate resources and information to facilitate the development of initial guidance session materials and structure. The prescreening questionnaire was developed collaboratively with experts in pediatric and adolescent educational and vocational support and adapted from a pre-existing educational liaison questionnaire used clinically. It was refined through clinical experience and stakeholder input to ensure its relevance and actionability for a navigator focused on providing support to AYAs and their caregivers.
Endorsed Needs of Eligible Families and Follow-Up Questions

Based on expert consultation (e.g., educational liaison, social workers, child psychologists) and participant feedback, the study team categorized educational and vocational needs into three domains: 1) school enrollment, 2) learning needs, and 3) financial needs related to school. Each need was further classified by complexity – low, moderate, or high – based on information collected through the screener and initial recruitment phone call. Caregivers reported all concerns on behalf of their AYA, and the study navigator delivered the guidance session and resources accordingly. AYAs offered the opportunity to co-participate and attend the guidance session with their caregivers. To maintain standardization, feasibility, and confidentiality, the navigator provided standard guidance and resource referrals but did not engage in direct interventions (e.g., submitting paperwork, contacting schools, coordinating care with medical providers). An overview of this process is outlined in Figure 1, with example navigator prompts provided in Table 2. Process map for decision-making in the educational guidance sessions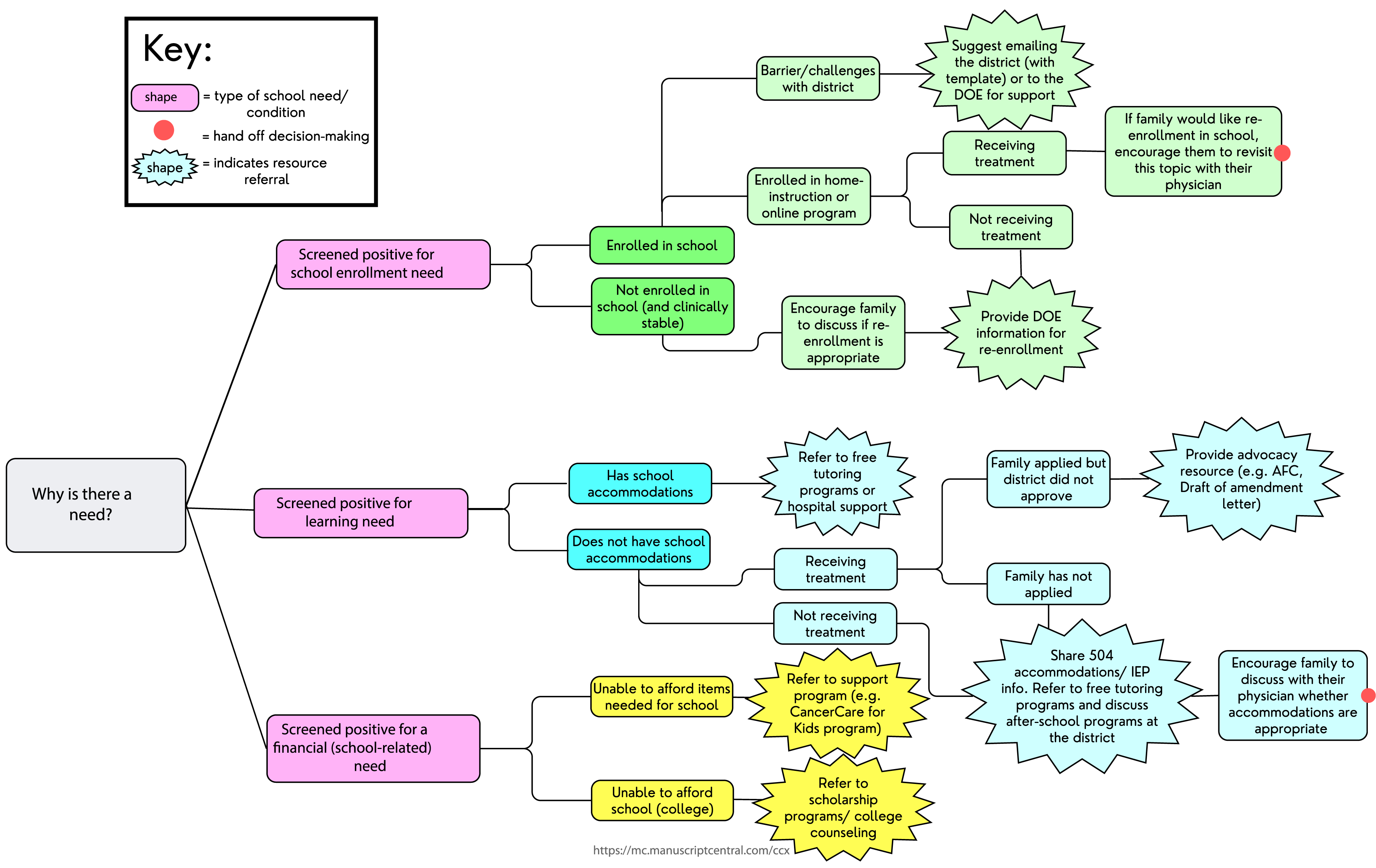
For school enrollment, needs were classified as high if the AYA was not enrolled, and moderate if the caregiver needed support applying for home instruction. Learning needs were considered high if no formal accommodations (e.g., IEP or 504 Plan) were in place, moderate if an accommodation plan existed but was not adequately implemented, and low if accommodations were in place but required maintenance or renewal. Financial needs related to education were addressed through the AYA-NAV intervention.
Beta Testing of Educational Guidance Sessions
Recruitment and Consent
Caregiver participants for beta testing of the educational guidance sessions were recruited from the pediatric oncology clinic if they identified as a self-reported caregiver to a patient between 12–26 years (inclusive) with a cancer diagnosis who was receiving active treatment or within 12 months of treatment completion. The primary participant was the caregiver, defined broadly as a parent or other family member involved in the care of the AYA; AYAs were offered co-enrollment, but this was not required. Participants were required to have English or Spanish as their primary language, reflecting the most common languages spoken by the patient population, our formative needs navigation intervention language availability, and the languages spoken by the study navigator, who is bilingual (English/Spanish).
After obtaining provider approval to approach potential participants, caregivers were sent an opt-out letter that allowed one week to decline further contact regarding the study. Caregivers who did not opt out were subsequently contacted by phone, email, or in clinic to assess interest in participation. Participants were informed that participation was voluntary and that they could withdraw from the study at any time. Informed consent was obtained by trained study staff (e.g., study navigator) either in person or via telephone prior to participation. Participant information was collected and stored securely in accordance with institutional policies, and only authorized study personnel had access to identifiable data.
Beta Testing Participants
Figure 2 illustrates the recruitment and participation for prescreening and guidance sessions. Briefly, of 35 caregivers approached, 17 agreed to complete the prescreening participation (AYAs aged 12–20; M = 16.31; SD = 2.18) to determine whether they screened positive for educational or vocational needs. Of 17 caregivers who completed the pre-screener, 13 screened positive at least one unmet need (for either financial toxicity, unmet health-related social needs, or educational needs) and enrolled in the broader needs navigation study. Of 13, 11 screened positive for educational needs. Among the caregivers who screened positive for educational needs, diagnoses of their children included leukemia/lymphoma (n=4), solid tumors (n=5), and neurological cancers (n=2). Of these participants, 8 of 11 caregivers completed the guidance sessions (five mothers, two fathers, and one aunt). Among these caregivers, 4 were Spanish-speaking and 7 were English-speaking. Reasons for non-participation included: being overwhelmed by other medical or personal items (n=2); and being removed from the study due to deteriorating clinical status of the AYA (n=1). Recruitment of participants through prescreening and guidance session participation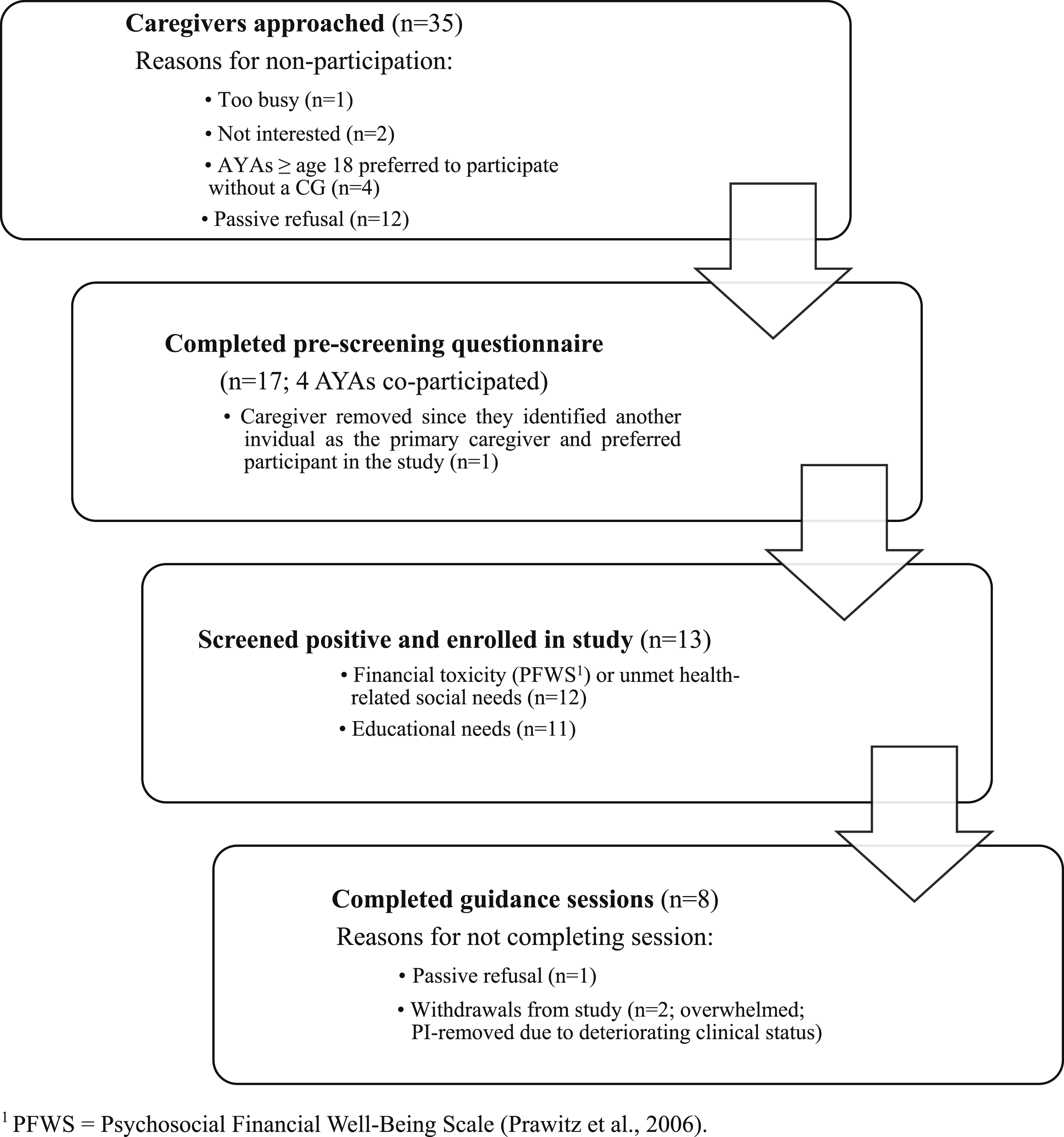
Beta Testing Intervention Delivery
In the beta testing phase, we conducted 8 one-hour individualized formative guidance sessions with caregivers of AYAs, gathering qualitative data on educational challenges. Insights from these sessions were used to inform the refinement of resources and guidance provided during subsequent sessions. Debriefing sessions were held with the educational liaison, the study navigator, the principal investigator, and the coordinator on a biweekly basis to review, analyze, and refine the intervention model. Data were triangulated from participant and stakeholder input to inform resource provision (e.g., referrals to educational advocates, Department of Education [DOE] resources). The preliminary list of resources was collated based on prior stakeholder input. However, the resources that were ultimately shared with patient and caregiver participants during and after a guidance session required tailoring to meet the unique needs of each AYA and caregiver. This tailoring was done by the study navigator after reviewing their baseline surveys prior to the educational guidance session. The navigator collected detailed notes and, with participant consent, recorded three sessions via Zoom 36 for later transcription and analysis. Follow-up telephone check-ins occurred one month and three months after completion of the guidance session, using a semi-structured script to assess the usefulness of the guidance and identify remaining educational needs. The guidance sessions that were recorded were subsequently re-analyzed by another member of the study team who was uninvolved in the guidance session development or delivery; another set of field notes were generated. All documentation, field notes, and audio files were analyzed using a directed content analysis 37 to identify key session elements and necessary refinements for future feasibility testing. Findings from these analyses informed iterative revisions to the guidance session protocol. The structured guidance session protocol was iteratively refined, integrating prescreening results, navigator notes, and a curated resource list. To streamline delivery, we actively created a customizable slide deck via Canva, 38 allowing real-time tailoring by hiding irrelevant slides and focusing on patient-specific resources. By the end of the study, a comprehensive slide deck that addressed various educational needs was developed and could be shared with caregivers post-session, ensuring families received actionable, individualized educational support.
Participant Feedback
The study team conducted brief check-ins at one and three months post-guidance sessions to assess the perceived utility of the session and to offer opportunities for additional support. Feedback was collected through qualitative notetaking during these check-ins and used to inform ongoing refinement of the guidance session structure and materials. Most participants reported the sessions were helpful and valued the school-related support. Some expressed a desire for more comprehensive information, while others preferred brief interactions (e.g., sessions lasting 5-20 minutes). Preferences for session frequency also varied; some requested more frequent sessions, while others favored minimal follow-up.
Determination of Intervention Component
Informed by expert input, navigator research, and participant feedback, the team developed a standardized slide deck to support information delivery during educational guidance sessions. The slides were designed to be easily accessible and shareable via email for future reference, a decision made by the research team based on participants’ feedback that the information shared via email could have been better organized so they could have the referrals for ‘later reference’. The materials were subsequently shared with stakeholders, including patient partners, who supported this approach. The slide deck includes content relevant to educational needs and challenges faced by students ages 12+, including applying for accommodations (e.g., IEP and Section 504), enrolling in school, applying to college and financial aid, academic difficulties such as concerns about grades or passing classes, and high school graduation. A vocational component was added for AYAs aged 18 years and older to provide information and resources on career navigation, job applications, vocational school, inability to attend work, unemployment benefits, disability services, and mental health resources. Each slide includes seamless access to resources via embedded links, and the content was organized for efficient navigation based on specific criteria, such as resources specific to local NYC residents, Spanish-speaking AYAs, specific age groups, and type of resource (e.g., community or school-based). During guidance sessions, content was individualized by selecting resources aligned with each caregiver’s identified educational or vocational concerns. The need for further refinement will be assessed during the planned pilot study of the refined AYA-NAV intervention (NCT06950983).
Discussion
Through a patient- and caregiver-informed process and multidisciplinary collaboration, we developed guidance sessions as a part of the AYA-NAV needs navigation program, a structured model designed to identify and address educational needs among younger AYAs with cancer and their caregivers. In this manuscript, we describe the intervention development process used to create a structured educational guidance framework for AYAs with cancer, an area that has received comparatively little attention within existing care navigation and survivorship support programs. Although the model was developed within a broader needs-navigation study, the educational guidance component represents a targeted approach to addressing the educational disruptions commonly experienced by AYAs during cancer treatment. This work provides the foundation for future pilot testing to evaluate feasibility and explore the intervention’s potential to improve educational and longer-term vocational and other health outcomes for AYA cancer survivors.
Within the WHO Social Determinants of Health framework, educational and vocational attainment are considered intermediary determinants that shape long-term socioeconomic stability and health outcomes. To date, most navigation interventions addressing intermediary social determinants of health have focused primarily on connecting patients to financial resources. Far fewer have systematically addressed educational needs, despite their clear influence on long-term survivorship and quality of life. This work extends the scope of needs navigation by incorporating structured educational guidance. Addressing these needs is particularly important given documented disparities among AYA cancer survivors, who experience more than double the risk of unemployment and lower educational attainment compared to their healthy peers.39,40
Qualitative feedback from AYAs and caregivers reinforced the importance of assessing educational and other health-related social needs early and throughout the cancer trajectory. Caregivers valued consistent check-ins related to school and emphasized the importance of receiving actionable resources. Several caregivers also highlighted the benefit of having a designated individual to guide them through complex processes, such as re-enrolling their child in school following treatment. At the same time, readiness to engage in educational planning varied across families and was influenced by diagnosis, treatment stage, and emotional readiness. These findings suggest that future research should examine the optimal timing and frequency of educational navigation, recognizing that engagement needs may vary across the treatment trajectory and across populations with different diagnoses and treatment intensity.
Although the study allowed for co-participation of AYAs with their caregivers, depending on family preference, the majority of families did not opt to participate as a dyad. This likely reflects both the age distribution of participants, as most AYAs in this study were younger adolescents, and the central role caregivers play in navigating educational systems during active treatment and early survivorship. While AYAs may assume greater responsibility for educational and vocational planning as they age, caregiver involvement remains essential for younger adolescents and during periods of intensive treatment. Future iterations of this intervention may therefore benefit from exploring dyadic approaches that incorporate both caregiver and AYA participation.
Timing also emerged as an important consideration for intervention delivery. In this study, families were eligible to participate if the AYA was receiving treatment or within six months of treatment completion. However, as with other means-tested benefits or health-related government support, the timing of efforts to address educational needs may influence access to services. For example, patients undergoing active treatment may be more likely to receive expedited approval for school accommodations under Section 504 when treatment-related impairments are clearly documented. 41 Conversely, shorter treatment durations (e.g., < 6 months) may limit the time available for service enrollment or formal educational planning. Future research should also investigate the optimal timing for delivering educational navigation and consider whether educational policies should allow more flexible eligibility periods for young patients with cancer.
In addition to timing, future iterations of this intervention may benefit from greater standardization in identifying educational needs. In the current study, needs assessment relied largely on navigator expertise to evaluate the presence and severity of educational concerns. Future research could explore validation of the educational needs screener to improve consistency, reproducibility, and scalability. One potential approach would be adapting the screener used in this study or integrating existing tools, such as the Brief School Needs Inventory (BSNI), to systematically assess educational risk and guide prioritization of supports. 18 Further adaptation of such tools for AYAs, including further incorporation of vocational domains, may support more comprehensive and standardized identification of needs while maintaining flexibility to address individual circumstances.
Future research will evaluate the effectiveness of the educational guidance sessions within AYA-NAV using both caregiver- and AYA-reported outcomes, including resilience and educational or vocational re-engagement. Because education and employment function as important social drivers of health, these outcomes will also be examined in relation to broader health-related social needs, such as financial strain, housing instability, and transportation barriers. In addition, global health outcomes 42 will be assessed to capture changes in mental, social, and physical well-being following participation in the intervention.
Strengths and Limitations
This study represents, to our knowledge, the first structured approach to developing and delivering navigation support for educational needs among AYAs with cancer through caregiver-directed guidance. We acknowledge that the guidance sessions are tailored to a specific geographic region, however, the development process and outcome are transferable and may be adapted for other community settings.43,44 Additionally, due to the formative design with beta testing, the small sample size and single-site recruitment limit the generalizability of these findings, and further feasibility and pilot testing is warranted. AYAs and caregivers consistently expressed a desire for direct, actionable educational support – highlighting a service gap outside of highly resourced cancer centers, where vocational counselors or educational liaisons are rarely available. Our findings demonstrate a process to address these needs using a centralized delivery model from a trained patient navigator that may be scalable to resource-limited settings. A strength of our process was the patient- and caregiver-informed development from inception. Further, we prioritized up-front integration of bilingual support to include Spanish-speaking families. However, challenges arose due to the lack of public-facing, Spanish-language educational materials and websites and the need for navigators to become familiar with specialized educational terminology in Spanish, which significantly increased preparation time. These findings underscore the importance of exploring and incorporating language accessibility from the outset of intervention design to prevent worsening of access disparities for patients who use languages other than English.
Conclusions
Despite growing recognition of the educational and vocational disruptions faced by AYAs with cancer, few interventions have systematically focused on addressing these needs within AYA oncology care settings. In this study, we developed a structured educational guidance model to help identify and address educational and vocational challenges faced by AYAs with cancer and their caregivers. This work highlights the central role of educational and vocational support within broader needs navigation frameworks and provides a foundation for future pilot testing to evaluate feasibility and preliminary effect on improving educational outcomes. By addressing educational and other health-related social needs, navigation interventions may help reduce barriers to educational attainment and long-term socioeconomic stability among AYA cancer survivors.
Footnotes
Ethical Considerations
This study was approved by Columbia University Irving Medical Center IRB (Protocol AAAU9477, initial approval granted 2/9/24).
Consent to Participate
Informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Pilot Grant, Leveraging COmmunity Partnered nEeds navigation to reduce unmet health-related social needs among Caregivers for Adolescent and Younger Adult Cancer survivors (Cope-CAYAC) (PI: Melissa Beauchemin), supported by the Center for Social Capital (U54CA280808).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.