
Abstract
Introduction
Adolescents and young adults (AYAs) with cancer experience substantial psychosocial distress, yet participation in supportive oncology services remains low. Community-based and nonprofit programs outside hospital systems provide essential developmentally appropriate supportive care, particularly during transitions to surveillance and longer-term follow-up, yet determinants of uptake in these settings are understudied. We examined program leaders’ perspectives on participation gaps and strategies to strengthen equitable engagement beyond the hospital.
Methods
We conducted a qualitative interview study using semi-structured interviews with leaders of community-based and nonprofit AYA psychosocial support programs in the United States and Canada (N = 21). A structured environmental scan and expert verification yielded a 132-program sampling frame; 33 organizations expressed interest. Interviews were analyzed using the Framework Method, organized deductively with the Social Ecological Model and the Theoretical Domains Framework and refined inductively. Transcripts were double-coded, and themes were developed through team consensus.
Results
Leaders described multilevel determinants of uptake, including fragmented referral pathways, limited organizational capacity and program visibility, stigma and safety concerns, and misalignment between program structures and early adulthood realities. Timing was a cross-cutting determinant: engagement was described as least feasible during intensive treatment and especially vulnerable at transitions such as treatment completion and early survivorship, when routines shift and clinical contact decreases. A central finding was wide variability in sociodemographic data collection. Many programs did not routinely collect participant sociodemographic information, limiting their ability to identify representation gaps and tailor outreach. Leaders prioritized strategies including ethical sociodemographic data collection, trust-based community partnerships, clinician-facing referral workflow supports, and shared infrastructure for repeated needs assessment and resource matching.
Conclusion
Low participation was shaped by implementation conditions, not individual disinterest. Improving equitable uptake may require investments in referral and re-referral workflows across care transitions, equity-monitoring infrastructure, and community-embedded approaches that build trust and improve discoverability beyond the hospital.
Plain Language Summary
Background: Young people with cancer often face serious emotional, social, and practical challenges. Many supportive programs exist to help them cope, but these services are often underused. This study explored why that gap exists by listening directly to the leaders of community-based cancer support programs. What We Did: We interviewed leaders from nonprofit and community-based programs in the United States and Canada that provide psychosocial support to adolescents and young adults with cancer. We asked about who their programs reach, who they struggle to reach, and what makes it difficult for young people to enroll or stay involved. What We Found: Program leaders described many barriers that limit participation. Young adults may feel overwhelmed by treatment, lack time or energy, or feel uncomfortable seeking support. Programs also face system-level challenges, such as unclear referral processes, limited visibility, staffing shortages, and heavy reliance on philanthropic funding. Most programs do not routinely collect demographic information, making it difficult to know which groups are being left out. Leaders consistently reported that young people from racially and ethnically minoritized communities, rural areas, lower-income backgrounds, or who speak languages other than English were least likely to participate. Why It Matters: Low participation in cancer support programs is not because young people do not want help. Instead, it reflects gaps in how support is organized, funded, promoted, and connected to health care systems. Improving referral pathways, collecting better demographic data, and building stronger community partnerships could help ensure that supportive care reaches young people who need it most.
Keywords
Adolescents and young adults (AYAs, ages 15 to 39) experience substantial psychosocial distress during and after cancer treatment, including elevated anxiety and depression and disruptions to education, work, relationships, and identity development.1-3 National cancer surveillance data also show a growing population of AYAs living with and beyond cancer, many of whom require supportive care beyond biomedical treatment. 4
In response, a wide ecosystem of psychosocial resources has emerged across the United States and Canada, including hospital-based supportive care programs, community organizations, digital platforms, peer support networks, and national nonprofits offering education, connection, financial support, and survivorship resources.5-7 Given that many AYAs receive cancer care in community settings, often outside pediatric and academic centers,8,9 and community-based treatment is common for many AYA diagnoses, 10 psychosocial support beyond hospital systems is an essential part of the AYA care ecosystem.
AYA cancer also occurs during a highly vulnerable developmental period, and supportive care needs often recur well beyond diagnosis, particularly during transitions from active treatment to surveillance and longer-term follow-up. Recent evidence indicates that developmentally appropriate information and support are frequently inadequate not only at diagnosis, but also during treatment and survivorship, and that survivors face persistent access barriers to follow-up care that can complicate transitions and continuity. 11 Because community-based and nonprofit programs operate outside oncology clinics yet often serve as primary access points for AYA support, this study focuses on organizationally independent programs while acknowledging that hospital-based psychosocial support and institutional survivorship supports warrant dedicated study. Community-based and nonprofit psychosocial support programs are not peripheral to AYA oncology; they are a core part of the supportive care landscape. While hospital-based psychosocial resources vary widely in availability, scope, and visibility, community-based programs often provide the age-responsive support AYAs actually encounter, especially across care transitions and beyond the clinic.
Despite the growth of psychosocial resources, a persistent gap remains between what AYAs need and what they use.12-14 Psychosocial interventions can improve quality of life and reduce anxiety and depression among AYAs,15-17 but participation in available psychosocial programs remains strikingly low.18-20 This pattern suggests that implementation conditions, including discoverability, referral pathways, and fit with AYA realities, may be as consequential as intervention availability. Many AYAs do not initiate services or disengage early.21-24 Digital models have expanded rapidly and show early feasibility for reducing geographic and logistical barriers. 25 However, digital delivery alone does not ensure engagement when clinician-facing supports for routine integration are limited. 26
To clarify why and how psychosocial support services are or are not taken up beyond the hospital, we conducted an implementation science-informed qualitative interview study with leaders of community-based and nonprofit AYA psychosocial support organizations. Using the Social Ecological Model and the Theoretical Domains Framework to organize determinants and strategies, we conducted semi-structured, in-depth interviews with community-based and nonprofit AYA psychosocial program leaders (N=21) to (1) characterize perceived participation patterns and equity-relevant representation gaps and (2) elucidate multilevel influences shaping nonparticipation and strategies to strengthen equitable engagement.
This study examines implementation realities in beyond-hospital supportive care to identify barriers, facilitators, and actionable strategies for oncology teams, psychosocial practitioners, and policy stakeholders seeking to improve equitable AYA psychosocial support uptake as expectations for age-appropriate care expand. 27
Terminology
We use psychosocial care and psychosocial support to refer broadly to services that address emotional, relational, and practical challenges across cancer treatment and survivorship. In the context of this study, however, these terms refer specifically to community-based and nonprofit oncology support programs (e.g., peer support, social connection, navigation, wellness, and expressive or supportive programming) rather than formal psychotherapy, psychiatry, or other licensed mental health care. We use program leaders to refer to individuals who deliver, oversee, or coordinate psychosocial support services outside hospital-based clinical care. Finally, patient and survivor are used interchangeably to denote a person living with a cancer diagnosis, regardless of treatment status.
Methods
Study Design and Analytic Frameworks
We conducted an implementation science-informed qualitative interview study to examine why and how psychosocial support services are or are not taken up in routine practice by identifying contextual determinants (barriers and facilitators) and stakeholder-identified implementation strategies. Semi-structured interviews were conducted with leaders of community-based and nonprofit AYA psychosocial support programs and analyzed using the Framework Method. 28 Analyses were organized using two complementary frameworks. The Social Ecological Model (SEM) was used to situate determinants within multilevel contexts (individual, interpersonal, organizational, community, structural),29,30 and The Theoretical Domains Framework (TDF) was used to organize determinants across cognitive, affective, and social domains.31,32 These frameworks informed the interview guide and were applied as prefigured domains to structure coding and theme development (Supplementary Appendix A, Table A1). The reporting of this qualitative study conforms to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 33 The study protocol was approved by the University of Maryland, Baltimore Institutional Review Board (IRB# HP-00110798), and oral informed consent was obtained. No monetary incentives were provided for study participation.
Sampling Frame, Eligibility, and Recruitment
To approximate how an AYA newly diagnosed with cancer might seek psychosocial support, research assistants within the AYA age range (H.L. and B.N.T.) conducted a structured environmental scan including online searches and phone/email inquiries to identify community-based and nonprofit AYA psychosocial support programs in the United States and Canada. The preliminary list was reviewed and expanded by the full research team based on disciplinary expertise and professional networks. W.E.G., director of the AYA program at The University of Texas MD Anderson Cancer Center, conducted an additional verification step by cross-referencing the compiled list with an existing database of psychosocial support and recommending programs for inclusion. This multi-step scan yielded 132 programs and served as the sampling frame (Supplementary Appendix A, Table A2). Because discoverability changes over time, we treated the sampling frame as a best-available representation of the beyond-hospital psychosocial support landscape during the recruitment window.
Participants were eligible if they held leadership roles (e.g., executive directors and program directors) within independent community-based or nonprofit AYA cancer support organizations and if the program was not housed in or formally affiliated with a hospital-based cancer center or clinical care setting. Participants were purposively selected to capture variation in program model, service modality, and geographic reach among community-based and nonprofit AYA cancer support organizations, and characteristics are reported in aggregate to protect identities. Some participants may have been aware of the study team through professional networks, but no formal pre-existing interviewer-participant relationship was established for study purposes.
Program leaders were contacted via email and invited to participate in a one-on-one interview. We used publicly available contact information and, when needed, contacted general organizational inboxes to identify an appropriate program leader contact. A recruitment log documented invitations, responses, eligibility screening, and dispositions (eligible, ineligible, declined, no response). Of the 132 organizations contacted, 0 explicitly declined participation and 1 was determined to be ineligible due to limited AYA-specific recruitment experience; 98 did not respond, and 33 expressed interest. Nonresponding programs were sent three follow-up emails over the recruitment window. Of those expressing interest, 21 completed interviews and 12 did not ultimately complete an interview due to scheduling constraints or nonresponse to follow-up. The analytic sample for this manuscript comprises 21 completed interviews. Because the sampling frame was derived from publicly identifiable organizations, information available for nonparticipating programs was limited and inconsistent. We were therefore unable to conduct a formal comparison of participating and nonparticipating organizations beyond recruitment disposition, but we considered the implications of nonresponse during interpretation of the findings.
Data Collection
Semi-structured in-depth interviews were conducted via Zoom by C.K.C., PhD, MSW, the study principal investigator between July and December 2024 and lasted approximately 60–90 minutes. At the time of the study, C.K.C. was a tenured faculty member. The interview guide addressed AYA engagement, barriers to participation, and strategies to improve inclusivity and equitable reach (Supplementary Appendix A, Table A3). The semi-structured interview guide was developed by the research team based on study aims and informed by the Social Ecological Model and Theoretical Domains Framework; as a researcher-developed qualitative instrument, it was not a standardized or previously validated scale. Interviews were audio-recorded, deidentified, transcribed verbatim, and imported into Dedoose (SocioCultural Research Consultants, LLC).
All interviews were conducted by C.K.C., whose lived experience as an AYA cancer survivor and cisgender woman researcher informs her approach to this work. C.K.C. holds extensive prior training and experience in qualitative interviewing and psychosocial oncology research. Participants were informed that C.K.C. was the principal investigator and that her lived experience as an AYA cancer survivor informed her interest in the topic. In alignment with Cheung’s Embodied Research Method, 34 members of the analytic team (A.N., C.K.C., N.G., M.G., S.C.L., and B.N.T.) completed intersectional reflexivity statements and discussed them prior to coding to enhance transparency and relational accountability.
Data Analysis and Trustworthiness
Qualitative analysis followed the Framework Method, 28 using deductive domains from SEM and TDF alongside inductive coding to capture concepts not well represented by prefigured frameworks. Transcripts were reviewed for familiarization, and an initial codebook was developed from the interview guide and early transcript review. Five trained researchers (A.N., C.K.C., N.G., M.G., B.N.T.) coded transcripts in iterative cycles. All transcripts were double-coded, and coder alignment was assessed through structured comparison of applied codes and discussion of discrepancies, which informed refinement of code definitions. Coded data were charted into a framework matrix, with rows representing interviews and columns representing domains and emergent themes to support within- and across-interview comparisons, and themes were refined through analytic memoing and team consensus. When interpretive differences arose, coders revisited the transcript segments and resolved discrepancies through consensus in team meetings, with C.K.C. facilitating discussion and documenting decisions in the codebook and audit trail.
Credibility and dependability were strengthened through double-coding, reflexive memoing, codebook documentation, and consensus-oriented interpretation. Transferability was enhanced by description of the beyond-hospital community-based and nonprofit program context. Confirmability was maintained through an audit trail linking theme development to illustrative quotations.
Sample Size Rationale
The interview sample size (N=21) was shaped by both recruitment feasibility and an information power approach, which determines sample size based on whether interviews provide sufficiently detailed and relevant information to address the research objectives. Within the completed interviews, information power was strengthened by the specificity of the study’s participant group, focused aims, and depth of interviews.
We also assessed thematic saturation, defined as the point at which additional interviews did not generate substantively new themes, domains, or implementation strategies relevant to the study aims. Saturation was evaluated iteratively through team debriefs and review of the evolving framework matrix as coding progressed. In later interviews, participants continued to provide richer examples, variation in emphasis, and nuance within already identified domains, but did not introduce substantively new thematic categories or implementation strategy types. Team review of the matrix indicated that the core multilevel determinants of uptake and the major strategy directions had stabilized, supporting N=21 as an adequate analytic sample for the study aims.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki (1975, as revised in 2024). Ethical approval was obtained from the Institutional Review Board at the University of Maryland, Baltimore (IRB# HP-00110798; approval date: June 20, 2024. The study was determined to meet criteria for exempt review. Verbal informed consent was obtained from all participants prior to participation, and the requirement for written consent was waived by the IRB. All participant details were de-identified in transcripts, quotations, and analytic materials so that individual identities and organizations could not be ascertained. Participants were purposively selected from a sampling frame of community-based and nonprofit adolescent and young adult (AYA) cancer support programs identified through an environmental scan and expert verification.
Results
Characteristics of Interview Respondents
Characteristics of Interviewed AYA Psychosocial Support Leaders and Their Programs (N = 21)

Note.
1 Categories for provider-level variables are mutually exclusive and sum to 100%.
2 For organization-level variables, respondents could select more than one category; therefore, totals do not sum up to 100%, except for ‘years of serving AYAs’ variable.
Organizational Practices for Data Collection and Equity Monitoring
Leaders described substantial variation in whether and how their organizations collect sociodemographic data about AYA participants. Figure 1 displays the proportion of programs that reported collecting specific sociodemographic elements. Programs commonly recorded age and gender, while fewer collected data on race, ethnicity, language, income, geography, or insurance status, limiting equity monitoring and the ability to tailor outreach (Figure 1). Sociodemographic participant data collected by AYA psychosocial programs in the study sample (N=21)). This figure displays the proportion of community-based AYA psychosocial programs, outside of hospital-based oncology care, that reported collecting specific sociodemographic data elements for their participants. Programs most frequently recorded age at diagnosis, age at participation, and gender, while fewer collected race, ethnicity, preferred language, income level, geography, or health insurance status. These patterns illustrate substantial variation in data collection practices across organizations and highlight gaps that may limit programs’ ability to assess representation, monitor equity, and tailor outreach to underserved AYA populations
Leaders often framed limited data collection as a deliberate effort to avoid discouraging participation, especially when questions were perceived as sensitive or burdensome. One leader described how their organization prioritized minimal data collection while attending to program balance and inclusion goals: “We don’t ask demographics. Like I know a lot of [programs] do… sexual orientation… we don’t ask. Race, we don’t ask… male or female, we do. That’s for housing, mainly, and making sure we have balance. We don’t want just women [programs]. We want male and female. We want co-gender [programs]. So that way we can learn from the other perspectives, and that’s what we’re all about.” — NPP15 (Participant ID)
Program Models and Delivery Modalities
Programs described offerings spanning informational and educational resources, navigation and practical supports, wellness programming, and peer connection, with the strongest concentration in opportunities for social connection (Table 1). Leaders noted that vocational, fertility or sexual health, and formal survivorship services were less commonly incorporated or were treated as peripheral (Table 1).
Digital delivery was widely used to expand geographic reach and reduce cost and logistical burden, typically through synchronous video groups and asynchronous resource sharing. Several leaders described that investment in virtual infrastructure before the pandemic enabled continuity and reduced administrative burden when in-person programming became infeasible: “…our digital meetups… originally obviously started as an in-person program, you know, way back in the day before we knew we could do this. And then, even Pre-COVID… we launched our digital meetups over Zoom… So, you know that transition during COVID was pretty easy for us, I guess, compared to some other organizations, because we were [already] doing it, which was helpful.” — NPP13
Across interviews, leaders also described using social media, websites, or custom platforms to improve discoverability and streamline intake for AYAs and clinicians.
Program Origins, Adaptation, and Persistent Inclusion Gaps
Many organizations described origins grounded in personal experiences with cancer and in perceived gaps in age-appropriate psychosocial support. Leaders emphasized that programs often evolved iteratively in response to organizational learning and shifting community priorities, rather than through standardized design. Even among programs describing themselves as AYA-focused, leaders reported variation in how age eligibility was defined, reflecting broader ambiguity in how AYA is operationalized across community-based settings.
Leaders also described internal efforts to address inclusion gaps within organizational leadership and governance, often prompted by recognition that the cancer support space tends to be demographically narrow: “So my team is primarily White women... Our board is fairly White… we’ve really taken it upon ourselves to… make sure that there are people of other lived experiences and demographics within other pieces of our leadership… because… most of the participants in the cancer space in general are White women.” — NPP016
Perceived Representation Gaps in AYA Program Uptake
Leaders frequently described their service populations as predominantly White, cisgender women, often in their 30s and living in urban areas. Underrepresented groups commonly named across interviews included men, younger AYAs, racially minoritized AYAs, LGBTQ+ AYAs, rural residents, immigrants, non-English-speaking AYAs, and those with greater financial needs or rare cancers. As one leader summarized: “Our biggest, biggest gaps in [participation] are always the younger [AYAs] 18 to 25, male-identifying individuals, and BIPOC individuals.” — NPP05
Multilevel Barriers to Participation and Retention
Leaders characterized barriers to AYA engagement as layered and interacting across program design, referral pathways, and AYA psychosocial and structural realities (Table 2). At the organizational level, leaders described limited staffing and funding for outreach and follow-up, constraints in providing access-related supports, and challenges aligning service schedules with AYA work and caregiving demands. One leader described how employment conditions can make even free programming inaccessible: “If someone is working an hourly position, and they're working in the evenings, they're not going to be able to come to our programs… there’s nothing then for them.” — NPP16 Themes and Program Leaders’ Quotations Characterizing AYA Participation in Psychosocial Oncology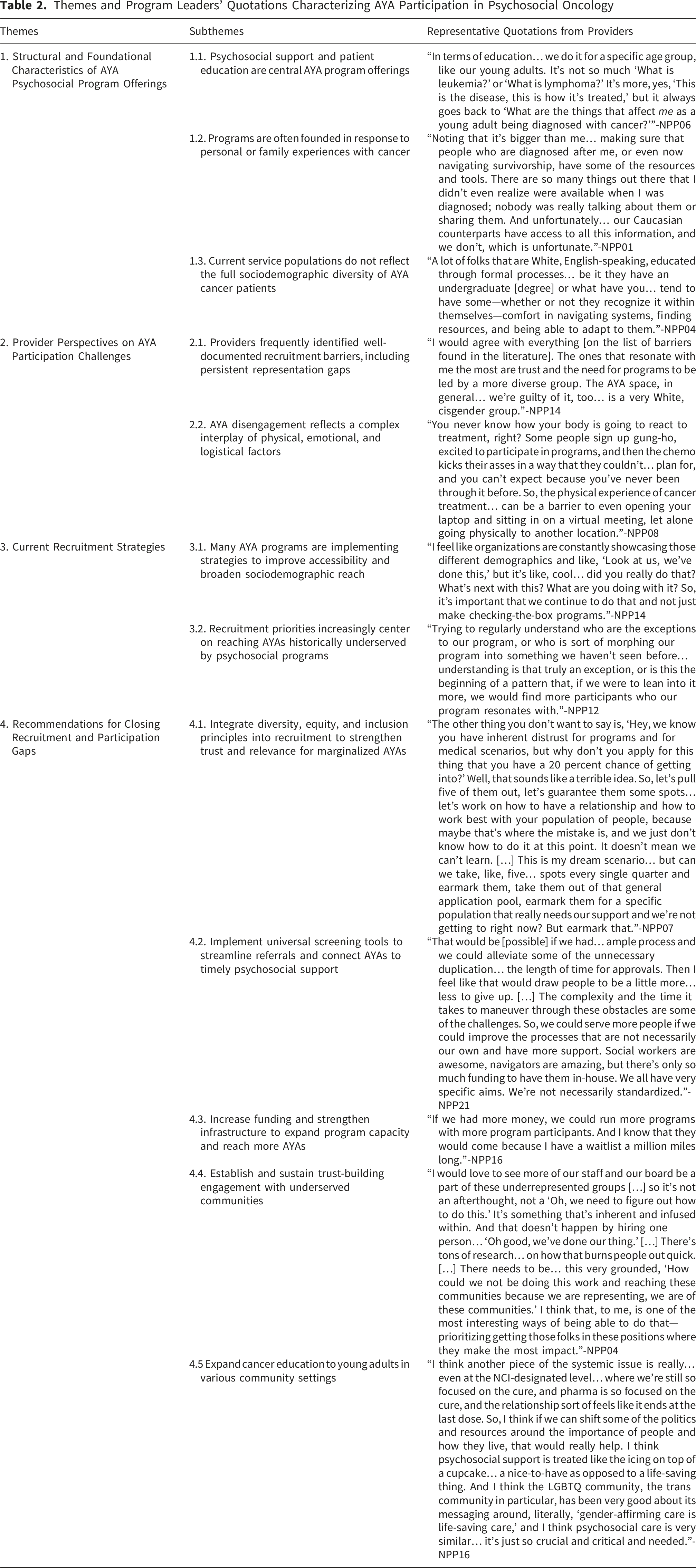
Leaders also described limited integration with oncology workflows during active treatment and early survivorship, noting that referrals often depend on overextended health care providers who have inconsistent awareness of community resources: “It's difficult to get oncologists and to get social workers to immediately direct people to us… the last thing they’re… thinking about is getting them psychosocial support.” — NPP08 At the individual and interpersonal levels, leaders emphasized stigma, emotional burden, limited perceived need, and low awareness of psychosocial support. One leader described a broader pattern of reluctance to seek psychosocial help, including perceived gendered differences in uptake: “This is a group that… doesn't lend itself to finding help… they don't seek out opportunities for therapeutic help… and again, you see a massive… male-female divide.” — NPP02
Intersectional vulnerabilities were also described as shaping uptake and safety, including concerns about information disclosure, precarious insurance coverage, and limited caregiver availability. One leader highlighted fears related to immigration enforcement as a deterrent to engagement for some Latine AYAs:
“When we look at specifically the Latine community… just fear of ICE [U.S. Immigration and Customs Enforcement]… sharing information about their address… that’s come up as a concern… navigating safety planning.” — NPP17
Leaders further emphasized that financial barriers persist even when programs are free, given lost wages and the costs of participation:
“Class and financial status is always one [barrier]… our programs are free… but still lost wages, time off work, childcare…” — NPP05
Dropout and Disengagement as Multifactorial Process
Leaders described dropout as difficult to interpret in the absence of systematic evaluation capacity, and as shaped by timing, competing demands, psychological depletion, and mismatch between program structure and AYA realities. Leaders also described uptake as time-sensitive, with participation often least feasible during intensive treatment and difficult to sustain during transition points such as end of treatment or early survivorship when routines shift and clinical contact decreases. Several noted that programs rarely have systematic ways to document where participants are in the treatment or recovery trajectory, limiting their ability to anticipate vulnerability windows or tailor re-engagement. One leader associated limited resources with their inability to improve programmatic fit: “If we had more money, we could run more programs with more program participants. And I know that they would come because I have a waitlist a million miles long.”—NPP16.
Another leader described uncertainty in understanding repeated non-return among AYA men in support groups and the challenge of interpreting attrition without sufficient data: “…of the [support groups] that we have had a male come to, they’ve never come to a second one… we’re backtracking, because there’s… so many X factors… is it the wrong day… the topics… felt uncomfortable… I don’t know… ‘Did you notice? Because this is a red flag’… ‘Okay, sit up and pay attention to this’… I don’t know if this is actually a thing, or… just what I’ve observed.”— NPP007
Leaders also noted that clinical environments themselves can be aversive for some AYAs, especially when supportive services require returning to sites associated with treatment: “…you have to go back into the building where you were treated… and a lot of people don’t want to do that. It’s very triggering...” — NPP16
Others described disengagement when programs do not feel welcoming, immediately relevant, or socially identifiable: “Young people leave programs if they don’t feel that it’s a welcoming place… if they don’t feel that they can identify with the other people in the group… and if they don’t feel that it’s giving them something immediately.” — NPP02
Some leaders also described aging out as a distinct form of disengagement that does not imply diminished need for support: “Sometimes it’s just aging out of the community… doesn’t mean the community support needs go away.” — NPP04
Equity-Focused Recruitment Adaptations and Priority Directions
Some leaders described ongoing efforts to broaden reach through equity-centered practices, including internal justice, equity, diversity, and inclusion (JEDI) structures and community partnerships (Table 2). One leader described how equity commitments were distributed across organizational roles and outreach strategy: “We have an internal justice, equity, diversity, and inclusion committee… it’s woven into everyone’s role at the organization… how can we improve marketing efforts, because our marketing department plays a large role… how can I, in my recruiting efforts, make key partnerships or offer certain services like additional scholarships or additional communication.” — NPP05
Many leaders also described shifts toward community-embedded recruitment and culturally congruent program leadership, including explicit attention to avoiding extractive outreach: “We are… working with community partners… making sure that those programs… are led by people from within those communities, instead of… the White savior coming into those spaces.” — NPP08
Looking ahead, leaders emphasized partnerships, public education about psychosocial support, and stronger integration with healthcare systems to reduce referral friction. Leaders also described interest in shared infrastructure across organizations, including coordinated data collection and standardized needs assessment with resource matching to reduce reliance on clinician memory and time: “There's not an easy way for hospital staff to be able to use [AYA psychosocial] resources… I wish that there was a universal needs assessment… linked to the relevant resources from a purely objective standpoint.” — NPP12NPP17 One leader contrasted the highly visible support culture and advocacy platform in breast cancer with the relative invisibility of psychosocial resources for other AYA diagnoses, arguing that uneven public-facing messaging across cancer types shapes help-seeking norms and makes psychosocial support feel routine in breast cancer but less so for others. “…the breast cancer community… they’re tight. They come together, talk to each other, and that opens up, ‘Have you been on this program? Have you heard of this program?’ They also have programs specifically [for] breast cancer—camps, programs—creating a culture with a lot of commercialized messaging, in my opinion, saying, ‘Hey, ask for support… we’re here for you.’ That makes it feel normal to seek help. I don’t think it’s as normalized [for other cancers] because they don’t see the commercials or marketing that make it feel routine to look for additional care—even though those resources exist.” — NPP015
Discussion
This implementation science-informed qualitative interview study examined barriers, facilitators, and strategies for AYA psychosocial support uptake in community-based and nonprofit programs, an understudied yet consequential segment of the supportive care ecosystem for AYAs with cancer. Program leaders described AYA participation gaps as shaped less by lack of interest in support and more by when support is offered, how referrals occur, what early adulthood permits, and whether program structures fit the realities of treatment, work, caregiving, and recovery. Collectively, the findings position low uptake as an implementation problem rooted in infrastructure, workflow, and fit across the supportive care ecosystem.
Multi-Level Factors Drive Participation
Using the Social Ecological Model and the Theoretical Domains Framework, we interpret AYA psychosocial uptake as produced by interacting determinants across structural, community, organizational, and interpersonal levels rather than by individual preference alone. Leaders emphasized that engagement reflects treatment-related impacts on AYAs’ capacity, competing responsibilities, communication environments, and clinicians’ variable ability to refer efficiently, consistent with prior work highlighting the role of psychosocial bandwidth, practical constraints, and fit between services and daily life demands.35,36
Figure 2 summarizes this multilevel interpretation. The model maps four nested ecological levels (structural, community, organizational, and individual program leader) to the specific challenges leaders identified at each level, showing how challenges at one level can compound challenges at others in shaping AYA psychosocial program participation. The model also illustrates feedback across levels, such as resource constraints shaping organizational capacity, fragmented referral processes increasing staff workload, and program experiences informing adaptation priorities. These constraints contribute to missed referral opportunities when clinical teams lack low-effort tools to match AYAs to psychosocial resources early enough for participation to be realistic. Program-informed contextual factors and challenges to AYA participation in psychosocial oncology care, A conceptual model. This conceptual model illustrates how program-reported barriers to adolescent and young adult (AYA) participation operate across multiple ecological levels. Guided by the Social Ecological Model and the Theoretical Domains Framework, the figure depicts four nested domains—structural, community, organizational, and individual program leader—each associated with specific contextual factors (for example, environmental context, social influences, memory and attention, emotional impacts of work). Arrows extending from each level identify corresponding participation challenges, such as inaccessible program design, logistical constraints, cultural and linguistic mismatch, limited clinician referrals, insufficient organizational data collection, program leaders’ burnout, emotional overload, stigma, and low perceived need for support. Bidirectional arrows reflect that challenges across levels interact dynamically, reinforcing or exacerbating one another. Collectively, these multilevel influences shape the likelihood that AYAs access and remain engaged in psychosocial oncology programs
Leaders’ accounts also highlight timing as a cross-cutting determinant of uptake. Participation was described as most vulnerable during periods of high symptom burden and competing demands and during transition points such as treatment completion, return to work or school, and early survivorship, when clinical follow-up may become less structured. Limited infrastructure to capture participants’ clinical phase may further constrain programs’ ability to align outreach, re-contact, and program offerings with periods of heightened need.
System Design, Literacy, and Referral Fragmentation
Respondents characterized recruitment as being strongly constrained by systemic conditions outside the scope of individual program influence. The most persistent structural barriers included lack of centralized intake or assessment mechanisms that can be repeated over time as needs change, absence of interoperable referral systems, and insurance-linked participation gating. Program leaders also highlighted that geographic feasibility challenges (e.g., time zone differences, travel burden) were especially impactful for AYAs navigating supportive care selection across large catchment regions.
Structural-level findings underscored patterns of missed enrollment opportunities when clinical teams lacked automated or low-effort mechanisms for matching AYAs to psychosocial resources. These determinants were understood as limiting initial program uptake even when supportive care services were theoretically available. These findings are consistent with prior work discussing how the Australian Youth Cancer Service employs a nationally coordinated approach to monitor service delivery for AYAs with goals to improve coordination among different care providers, address specific needs that arise due to fragmented referral systems and meet the challenges posed by geographical disparities. 37 Prior evidence shows that location of cancer treatment influences AYA enrollment onto clinical trials 38 ; likewise, location of psychosocial care matters. These findings also point to the importance of cross-sector coordination between oncology teams and community-based programs so that supportive care options remain visible across care transitions and referrals do not depend on clinician memory.
Community-Level Influences: Literacy, Culture, and Informal Support Patterns
Leaders described structural barriers that limit uptake regardless of program quality, including lack of centralized intake or needs assessment, absence of interoperable referral mechanisms, and participation barriers linked to geography and feasibility. At the community level, leaders highlighted uneven awareness of psychosocial care and inconsistent literacy regarding what AYA support entails, as well as trust and safety concerns that can deter contact with organizations, particularly for AYAs navigating marginalization and surveillance risks. These insights echo prior studies of recruitment and retention of AYAs onto cancer studies, emphasizing the significance of community-driven issues and influence of healthcare professionals and family members on participation in research. 39
Organizational Capacity and Equity Monitoring Gaps
Organizational constraints were described as especially consequential. Because many programs rely on philanthropic funding, leaders noted limited staffing for outreach and follow-up, limited resources for access supports, and inconsistent clinical referral pathways. Leaders also described a widespread lack of clinician-facing tools to support triage and referral fit, leaving referrals dependent on individual awareness and time.
A central equity-relevant finding is that many programs do not routinely collect sociodemographic information on AYA participants. Leaders often framed this as a deliberate choice intended to avoid discouraging participation, particularly among minoritized groups. At the same time, the absence of routine sociodemographic documentation constrains programs’ ability to determine which AYAs are being reached, to identify gaps with confidence, and to tailor outreach, partnerships, and program design accordingly. Without consistent intake data, programs may be left to infer representation patterns from informal impressions, which can obscure participation gaps and limit data-informed planning.
Ethical sociodemographic assessment requires attention to how questions are introduced and implemented. Prior evidence indicates that sensitive items posed without clear purpose or relational context can reduce participation, particularly among marginalized groups.40,41 Accordingly, guidance should emphasize purpose statements, options to skip items, thoughtful timing, trauma-informed communication, and operational supports that prevent staff overload during intake and referral.
Program Leader Capacity and Recruitment Fatigue
At the individual level, leaders described the emotional labor of recruitment, limited bandwidth for repeated outreach, and uncertainty in how to message psychosocial support in ways that feel relevant and nonstigmatizing for AYAs. These experiences influence the sustainability of recruitment work in resource-limited settings and may widen inequities when engagement depends on discretionary, uncompensated labor rather than routinized processes. This account is consistent with AYA survivorship frameworks that call for sustained supports embedded in care systems rather than episodic offerings 42 and with evidence documenting ongoing psychosocial needs throughout AYA survivorship.43,44
Implications for Practice: Sociodemographic Data Collection as a Priority
Routine sociodemographic data collection is a foundational step for community-based and nonprofit psychosocial programs to identify which AYAs they are reaching, where representation gaps persist, and how outreach and program design can be adapted for equitable access. A core finding of this study is that many programs lack systematic sociodemographic intake practices, leaving leaders to infer participation patterns without consistent records. Addressing low uptake therefore requires parallel investments in program delivery, referral workflows, and data capacity so that equity monitoring and targeted engagement are feasible. In parallel, routinized referral and re-referral at key transition points (diagnosis, active treatment, end of treatment, and early survivorship) may help reduce drop-off that occurs when supportive care is offered too late or not revisited.
Leaders described sociodemographic assessment not as peripheral paperwork, but as operational infrastructure for coordinated outreach with clinical teams. Implementation research suggests that clinician behavior is most sustainable when referral tasks are routinized through prompts, automation, and shared systems that reduce time and cognitive load.45,46 Transparent, routine sociodemographic documentation can: (1) clarify which AYAs programs are not reaching, (2) align AYA priorities with clinician expectations, and (3) flag mismatches between program design and real-world participation constraints. This foundation also informs other equity-focused strategies described by leaders, including trust-based community partnerships and clinician-facing referral supports, by grounding those efforts in clear visibility into who is being reached and who is not.
Strengths & Limitations
To our knowledge, this study offers one of the most detailed examinations to date of how psychosocial support organizations identify and interpret barriers that impede equitable AYA access to supportive care. A primary strength is the depth of insight from leaders actively responsible for developing and implementing psychosocial supports beyond hospital settings. Use of the Social Ecological Model and the Theoretical Domains Framework, in combination with the Framework Method, supported systematic analysis while remaining responsive to emergent themes in an implementation science-informed qualitative interview study.
Although 33 of 132 contacted organizations expressed interest, most did not respond. We were unable to systematically characterize nonresponding organizations because publicly available information was limited and inconsistent across the sampling frame. As a result, the analytic sample may over-represent programs with greater staffing capacity, stronger organizational infrastructure, more stable communication systems, or greater interest in research and external visibility. This pattern may have influenced the inferences drawn from the data by emphasizing barriers, adaptations, and equity efforts described by relatively more organized or research-engaged programs, while undercapturing the experiences of less visible, more resource-constrained, or less formally structured organizations. Findings should therefore be interpreted as reflecting a purposive sample of participating beyond-hospital programs rather than the full landscape of eligible organizations.
Because hospital- and academic center-based psychosocial programs were outside the sampling frame, these findings should not be generalized to institutional supportive care settings, where psychosocial resources vary widely in availability, scope, and visibility. At the same time, this distinction should not be read to position community-based and nonprofit programs as peripheral to AYA psychosocial oncology. Rather, our findings underscore that these programs are a core part of the supportive care landscape and warrant direct study on their own terms, particularly given their importance across care transitions and beyond the clinic encounter. Future research should examine how community and academic oncology teams coordinate referrals, follow-up, and re-engagement across the treatment-to-survivorship transition.
Finally, the absence of direct interviews with AYAs constrains inference about AYA motivations and experiences. Subsequent work should incorporate AYA perspectives to more directly characterize lived experiences of referral processes, perceived relevance of psychosocial support, and context-specific barriers and facilitators shaping uptake.
Conclusion
Leaders of community-based and nonprofit psychosocial support programs described AYA psychosocial support uptake as shaped by interacting determinants across referral systems, organizational capacity, and AYA psychosocial and structural realities. Strategies proposed to strengthen equitable uptake emphasized routine sociodemographic data collection, trust-based community partnerships, clinician-facing workflow supports, and shared infrastructure for needs assessment and resource matching. Advancing AYA psychosocial oncology will require structural investments that make psychosocial support feasible to access, straightforward to refer to, and equitable across the supportive care ecosystem.
Supplemental Material
Supplemental Material - Beyond the Hospital: Understanding Psychosocial Support Uptake for Adolescents and Young Adults With Cancer in Community-Based and Nonprofit Programs
Supplemental Material for Beyond the Hospital: Understanding Psychosocial Support Uptake for Adolescents and Young Adults With Cancer in Community-Based and Nonprofit Programs by Christabel K. Cheung, Nishtha Gupta, Haelim Lee, Susan K. Parsons, Wendy Griffith, Gail Betz, Maria Gianelle, Adishree Nayak, Sophie C. Lu, Bria N. Thomas, Kimberly A. Miller, David R. Freyer, Melissa Beauchemin, Anao Zhang, Alexandra Psihogios and Michael E. Roth in Cancer Control.
Footnotes
Acknowledgments
We extend our deep gratitude to the psychosocial program leaders who generously shared their time, perspectives, and organizational experiences; no monetary incentives were provided for participation. We also thank Merrick R. McKelvie, MSW, LCSW-C, doctoral research assistant, for his thoughtful review and feedback on the manuscript.
Ethical Considerations
This study was approved by the Institutional Review Board at The University of Maryland, Baltimore (IRB# HP-00110798); approval date: June 20, 2024. The study was determined to meet criteria for exempt review.
Consent to Participate
All procedures were conducted in accordance with the Declaration of Helsinki. Verbal informed consent was obtained from all participants, and the requirement for written consent was waived by the IRB.
Author Contributions
C.K.C. and M.E.R. conceptualized the study and designed the research approach. C.K.C. M.E.R., A.Z., A.P., and K.A.M. contributed to development of the semi-structured interview guide and analytic framework. H.L. and B.N.T. conducted the environmental scan and developed the sampling frame, with verification support from W.E.G. C.K.C. conducted all interviews and led data collection. A.N., C.K.C., N.G., M.G., and B.N.T. conducted qualitative data analysis using the Framework Method, including double-coding, codebook development, and thematic synthesis. A.N., C.K.C., N.G., M.G., S.C.L., and B.N.T. contributed to interpretation of findings and analytic refinement through team-based consensus. C.K.C. drafted the original manuscript. N.G., H.L., S.K.P., W.E.G., G.B., M.G., A.N., S.C.L., B.N.T., K.A.M., D.R.F., M.B., A.Z., A.P., and M.E.R. contributed to critical revision of the manuscript for important intellectual content. All authors reviewed, edited, and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C. Cheung’s contribution to this article was supported by funds through the National Cancer Institute - Cancer Center Support Grant (CCSG) – P30 CA134274. M. Roth received research support from the National Cancer Institute P30 CA016672. Additionally, the University of Maryland School of Social Work’s Doctoral Research Assistant program provided research support for H. Lee and its Research Assistant Scholars Program provided research support for N. Gupta and A. Nayak.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to participant confidentiality and the sensitive nature of organizational data but are available from the corresponding author on reasonable request and with approval from the University of Maryland, Baltimore IRB, as applicable.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.