
Abstract
Background
Breast cancer patients and their informal caregivers often report unmet psychosocial, relational, and physical health needs. Dyadic interventions may improve patient and caregiver outcomes, but few have been integrated into clinical care or designed for Black breast cancer patients and their female caregivers. We used the Health Equity Implementation Framework to design for dissemination by identifying facilitators and barriers to implementing a dyadic survivorship intervention delivered via video teleconferencing (e.g., Zoom).
Methods
We conducted semi-structured interviews with a purposive sample of 18 collaborators with roles at a comprehensive cancer center and community organizations to understand facilitators and barriers to implementing a dyadic intervention for Black breast cancer patients and their caregivers. We used rapid qualitative analysis (templated summaries synthesized in matrices) to conduct a directed content analysis. We identified patterns in responses to interview guide questions and developed cross-cutting themes.
Results
Collaborators’ roles fell into four domains: patient-facing mental health (33%), patient-facing physical health (28%), research/administration (28%), and cancer-focused community groups (11%). Participants were supportive of a dyadic intervention for Black women with breast cancer and female caregivers. Collaborators noted that psychosocial care at the cancer center was already being delivered via Zoom and saw benefits to including caregivers. Overarching themes include the need to address gaps in care (for caregivers, Black women, and long-term breast cancer survivors); the importance of representation in building trust and mitigating stigma; and the challenges within the healthcare system around providing care services to dyads.
Conclusion
Application of these findings can help address the challenges of implementing a dyadic survivorship intervention for Black women with breast cancer and their caregivers in clinical settings. Expanding models such as the Health Equity Implementation Framework to include caregivers may help focus dissemination and implementation efforts on both members of a dyad and improve outcomes for both.
Plain Language Summary
Breast cancer patients and their caregivers both often report unmet needs involving mental and physical health once patients move into long-term survivorship. Programs or services for patient-caregiver pairs may improve outcomes, but these programs or services have not been included in clinical care very often, and few are designed for Black breast cancer patients and their female caregivers. We used the Health Equity Implementation Framework to help us understand what would make it easier and more effective to deliver a program or service for patient-caregiver pairs. We interviewed 18 colleagues from a comprehensive cancer center and community organizations to understand how to deliver a program or service for Black breast cancer patients and their caregivers. We used rapid qualitative analysis techniques to identify patterns in people’s responses to interview guide questions, and we developed over-arching themes that cut across questions. Participants were supportive of the idea of helping Black women with breast cancer and their female caregivers. Overarching themes include the need to address gaps in care (for caregivers, Black women, and long-term breast cancer survivors); the importance of representation in building trust and lessening stigma; and the challenges within the healthcare system around providing care services to patient-caregiver pairs. Our findings highlight the potential benefits and challenges of providing a program or service for Black women with breast cancer and their caregivers. Expanding models such as the Health Equity Implementation Framework to include caregivers may help us figure out how to deliver services to both members of patient-caregiver pairs, which may ultimately improve outcomes for patients and their loved ones.
Background
Breast cancer is the most commonly diagnosed cancer in Black women in the U.S. 1 Black women with breast cancer are less likely to receive guideline-concordant treatment and follow up care compared to white women,2-4 often report lower quality of life,5,6 and are 41% more likely to die from the disease. 1 Addressing these disparities requires innovative, effective interventions to support Black patients throughout treatment and survivorship.2,7,8
One way to support patients is to support their informal caregivers—the family members, partners, and friends who provide important emotional, tangible, and decision-making support to women with breast cancer.9-11 Although many caregivers find their role rewarding, 12 they may also face physical and emotional burdens due to caregiving.13-16 Outcomes such as depressive symptoms are often interdependent in patient-caregiver dyads,17,18 which means it may be effective to intervene with patients and caregivers together. 19
Much dyadic cancer caregiving research to date in the U.S. has involved primarily white, spousal couples,19,20 which is problematic given the well-documented disparities in treatment and outcomes for Black breast cancer patients.1,4,8 Health disparities with historical roots continue to be perpetuated through structural racism,21,22 and Black women with breast cancer may face interpersonal discrimination and feel they need to protect themselves from an untrustworthy medical system. 23 Spouses and other intimate partners often provide support to Black women with breast cancer who are partnered or married.24,25 The majority of older Black women in the U.S. are not married, 26 however, and Black women with breast cancer often rely on social support from an extended network of family and friends,27,28 particularly female caregivers. 29 In our team’s recent study of caregivers for Black breast cancer patients, for example, we found that the most commonly referred caregiver was a female family member of the patient. 30 A recent review found that equity-focused caregiving research is still in the very early stages. 31 Caregivers for Black breast cancer patients may have unmet psychosocial and health needs while having access to few tailored or culturally appropriate resources.30,32,33 It is crucial to better understand the experiences of breast cancer patients and caregivers of diverse racial and ethnic backgrounds and those who have a range of roles in relationship to the patient.
Dyadic interventions for cancer patients and caregivers, often delivered by nurses, counselors, or social workers, are a promising strategy for addressing individual and relationship-level psychosocial outcomes for both members of a patient-caregiver pair, but such interventions are rarely implemented in clinical practice. 19 There has been a lack of research examining several key factors, including (1) interventions for non-spousal dyads, (2) interventions delivered at timepoints other than cancer diagnosis, (3) dyads from minoritized racial/ethnic backgrounds, (4) flexible/remote modes of intervention delivery, and (5) facilitators and barriers to implementing dyadic interventions in clinical practice. 19 This work seeks to address those research gaps by developing a psychosocial intervention to be delivered to Black women with breast cancer and female (non-spousal) caregivers via video teleconferencing (i.e., Zoom) to facilitate successful transition to long-term survivorship.
Some previous research has examined facilitators and barriers to providing caregiver and family support in clinical contexts.34-36 In one mixed methods study of clinicians and administrators about implementing cancer caregiver support services, participants underlined the importance of obtaining buy-in from leadership, staff, and clinicians and identified cost and clinician burden as major barriers. 35 One qualitative study with family caregivers, cancer center leaders, and providers found barriers at multiple levels to providing caregiver services, including caregivers’ feelings of being overwhelmed, caregivers’ desire to focus on the patient, and structural constraints within the healthcare system. 34 Another qualitative study found that primary care and palliative care physicians often see caregivers as resources for the patient, but when caregivers themselves need support or training then providers may view them as a burden. 36 Although this work has provided important information about addressing caregivers’ needs, very little previous work has investigated implementation factors that may lead to successful clinical uptake of dyadic interventions that are designed for both members of a patient-caregiver pair.
Following the principle to “design for dissemination” we engaged collaborators from cancer care practice settings and intended users of the intervention early in the process of intervention development to better understand and nimbly adapt to variations within the anticipated intervention delivery context.37-40 This process is thought to maximize the chances that innovations are adopted and suitably address health equity. 40 We used the Health Equity Implementation Framework 41 to examine facilitators and barriers to implementation at multiple levels. Because the Health Equity Implementation Framework centers the clinical encounter, it is ideal for equity-focused health services research that examines the effects of both the immediate clinical context as well as the broader social context on adoption or uptake. 41 Using this framework and rapid qualitative analysis techniques, 42 we conducted this study to understand the perspectives of people who might be involved in the implementation of a dyadic survivorship intervention that would be integrated into clinical care for Black women with breast cancer and their female informal caregivers. Our goal was to generate actionable insights that would increase the likelihood of creating an intervention that would be successfully delivered in a clinical context.
Methods
Initial plans for the proposed psychosocial intervention were developed for a grant application and based on a review of the caregiving literature, as well as our team’s previous research with Black women with breast cancer and their caregivers. The proposed intervention was designed to be compatible with the current psychosocial care model at the cancer center where recruitment was conducted (i.e., outpatient therapy delivered by psychologists via telehealth) and was planned to be delivered to patients and their female informal caregivers around the transition to long-term survivorship. The team planned from the early stages of the project, however, that the final intervention would be shaped by findings from the team’s formative work (the interviews described here, plus separate interviews conducted with caregiver-patient dyads).
The COnsolidated criteria for REporting Qualitative research (COREQ) checklist was used as a starting point for reporting study procedures and findings. 43 However, in agreement with Braun and Clarke, we note that individual COREQ items are not always appropriate for reporting results of diverse qualitative methods, 44 including rapid qualitative analysis. We therefore followed reporting described by Keniston et al. adapting COREQ for rapid qualitative analysis. 45
Study Participants
We interviewed key collaborators from a comprehensive cancer center and community organizations in one Midwestern metropolitan area. Critical to “designing for dissemination” is engaging early in the design process with those individuals who might deliver, support, or champion the intervention. 40 Although the term “stakeholder” is commonly used in this context, 41 we use the term “collaborator” to emphasize the fact that we were soliciting interdisciplinary perspectives from colleagues and community members who might work together with our team to deliver the intervention. 46
Qualitative methods for implementation often use a targeted approach to participant selection and data analysis. 42 We used purposive sampling, which was appropriate because our aim was to ensure that we spoke with key individuals and thus maximized the “information power” of the data collected. 42 The interview list for people to approach for our purposive sample was developed in consultation with the director of survivorship services at the region’s comprehensive cancer, who suggested people at the cancer center and in the community who could provide rich data about the topics of interest. 42 Although a sample of 6-10 well-chosen participants can be adequate when conducting implementation research within a single health system, 42 due to the complex, multidisciplinary nature of breast cancer care, we aimed for a sample of 15 participants, which included doctors, nurses, researchers, administrators, mental health providers, and members of community organizations. Because our initial plans involved an intervention delivered by psychologists at the cancer center, we oversampled psychologists. These interviews were designed to complement our previous work with caregivers for Black patients,10,30 as well as ongoing dyadic qualitative interviews with Black patients and female informal caregivers.
Collaborators were eligible if they were 18 years of age or older; able to answer questions in English; involved in the delivery, referral, or planning of psychosocial or survivorship care for breast cancer patients; and a member of a local cancer-focused community group or employed by the cancer center, school of medicine, or hospitals affiliated with this project.
Procedure
This work was conducted by a team with a range of backgrounds and perspectives. Team members’ disciplinary backgrounds included social work, psychology, public health, implementation science, health disparities and health equity, marriage and family therapy, and sociology. Team members’ intersectional identities included both Black and white racial identities, and almost all were women (there was one man). One team member reported a history of cancer, and another reported experience as a caregiver for a Black female family member.
The interview guide developed by the study team was loosely based on the Health Equity Implementation Framework 41 and included questions about provider factors, patient factors, healthcare system factors, and societal influence, as well as characteristics of the proposed intervention (see Appendix for the complete interview guide). These questions drew on participants’ expertise and their roles in the cancer center or the community. 41 We asked about current referral patterns for mental health and survivorship services; the benefits and drawbacks of proposed intervention characteristics (i.e., a culturally tailored, dyadic intervention for Black women and female caregivers people delivered over Zoom around the transition to survivorship); and how the racial history of the region might affect intervention delivery. Based on previous focus groups 30 and ongoing dyadic interviews conducted by the study team, we also asked about taking a tiered approach to intervention in which a one-time celebratory event could be used to draw people in, inform them about services, and connect them to resources. Members of the study team pilot tested the interview guide by role playing with one another.
The first author emailed potential participants information about the goals of this research and invited them to complete a one-time, semi-structured interview of 30-45 minutes at a time that was convenient for them. She had a previous professional relationship with some but not all of the potential participants who were approached.
One-on-one study interviews were conducted and recorded using the university’s secure, HIPAA-compliant Zoom platform. Interviews were conducted by the first, second, or third author (a PhD-level faculty member and two doctoral students, respectively), all of whom had received training in qualitative research and all of whom identify as white and female. Questions were based on the interview guide (see Appendix), but interviewers could vary the ordering or wording of questions as needed based on the flow of conversation. At the end of the interview, participants reported their age in three broad categories (18-44 years, 45-64, 65 or older), race and ethnicity, gender, and highest level of education completed. After each interview, the video recording was deleted, and the audio recording was retained for reference during analysis as needed. Zoom auto-generated interview transcripts were also available for reference.
This study was approved by the Institutional Review Boards (IRBs) at the institution where recruitment was conducted, as well as at the institution from which the first author led the analysis [Washington University in St. Louis (#202302078, 2/24/23); University of North Carolina at Chapel Hill (#401090, 9/15/23)]. The research was considered exempt at both institutions because it involved low-risk procedures with adequate provisions to protect privacy and maintain confidentiality. The IRBs did not require the team to obtain written or verbal informed consent from participants; instead, participants were provided with study information via email and given the opportunity to ask questions before the interview. Participants received a $20 gift card to thank them for their time.
Analysis
We used rapid qualitative techniques to conduct a directed content analysis. 42 Rapid qualitative analysis is a useful strategy for implementation projects because it allows researchers to obtain actionable information quickly,42,45 and it can be used in conjunction with implementation frameworks. 47 Our analysis, which was iterative and involved high levels of coordination between team members, used templated summary forms and matrices to analyze participant responses.42,45,47-49 The goal of rapid qualitative analysis is to provide an overview of interview content and themes rather than an in-depth analysis of individual quotations. 47
The team created a template summary form that summarized responses to each question and contained additional notes about the interview. The form was piloted by the first, second, and third authors on an initial interview and refined after further discussion. 45 For each interview, one of the first three authors who had not conducted the interview used the template to summarize the participant’s responses. Summaries were entered into a matrix in Excel to examine responses within participants and across participant roles. 49 The first, second, and third authors used an iterative process to synthesize responses for each question/domain and identify over-arching themes that cut across questions. The first author checked all summaries and returned frequently to the original data to verify the findings. 45 Preliminary findings and themes were refined by the entire study team through discussion and review of the matrix and written drafts. The team discussed data saturation during the analysis process and agreed that it was reached. Although we did not solicit feedback on the findings directly from study participants, the first author discussed the findings with an umbrella organization of local breast cancer community groups during the group’s monthly meeting.
To protect participant privacy, to prevent identification, and to facilitate comparisons, we grouped collaborators into four general categories: patient-facing mental health (MH), patient-facing physical health (PH), research/administration (RA), and community groups (CM). In Results, we have been cautious when noting the intersection of demographic details and roles so that individual participants would not be identifiable.
Results
Twenty people were invited to participate; one did not respond, one declined (no reason for refusal given), and one declined but nominated another person from the same organization to participate (who she thought would be a good fit for the research). A total of 18 collaborators completed a Zoom interview from March to June 2023. Interviews lasted between 18 and 57 minutes. Collaborators’ roles fell broadly into four domains: patient-facing mental health (MH; e.g., psychologist, social worker) (33%), patient-facing physical health (PH; e.g., physician, nurse) (28%), research/administration (RA; 28%), and cancer-focused community groups (CM; 11%). Fifty percent self-identified as white and female, 33% as Black/African American and female, 11% as white and male, and 5% as another race and female. All described themselves as non-Hispanic. Ninety-four percent of participants reported having a graduate or professional degree, and 5% reported having some college.
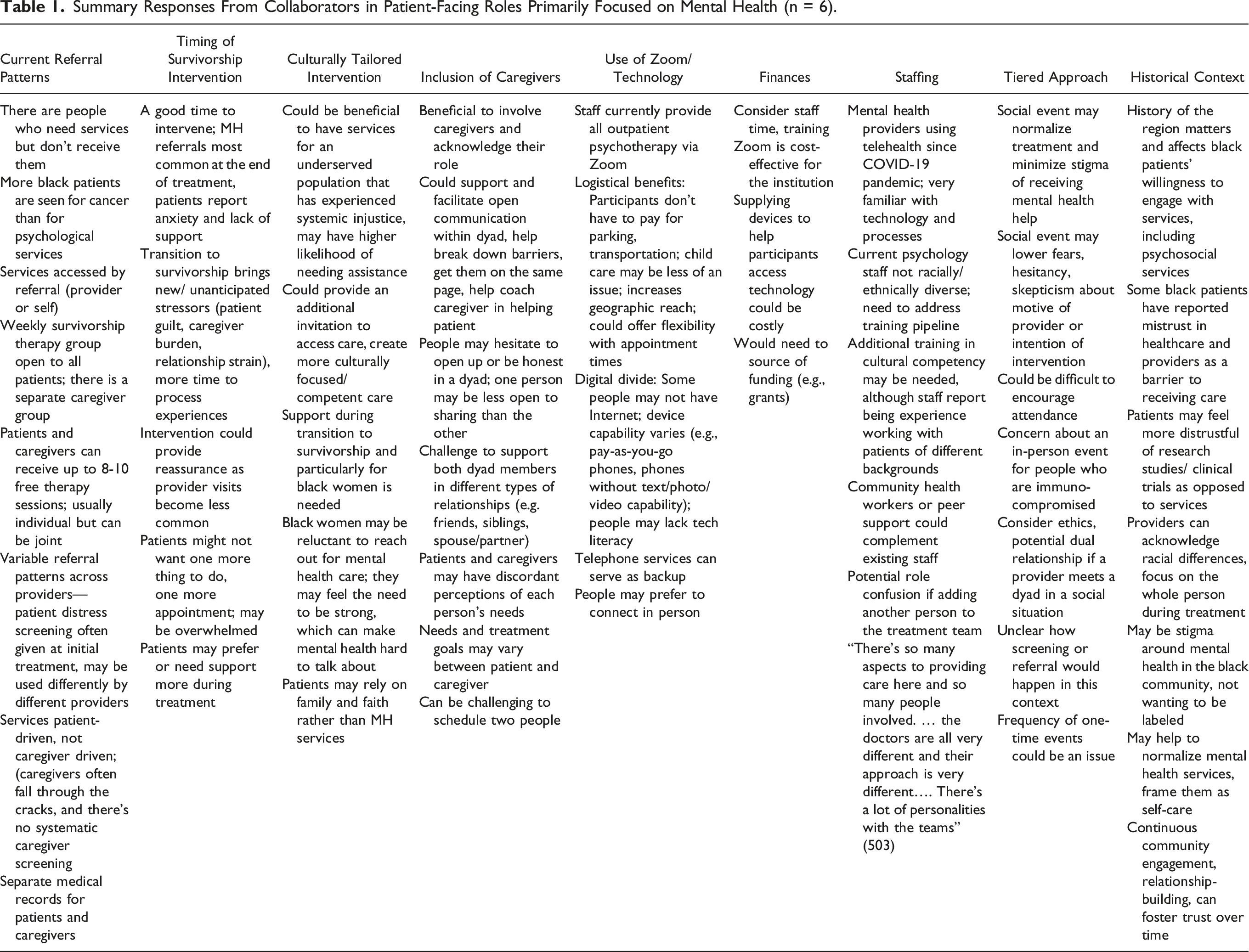
Summary Responses From Collaborators in Patient-Facing Roles Primarily Focused on Mental Health (n = 6).
Summary Responses From Collaborators in Patient-Facing Roles Focused on Physical Health (n = 5).

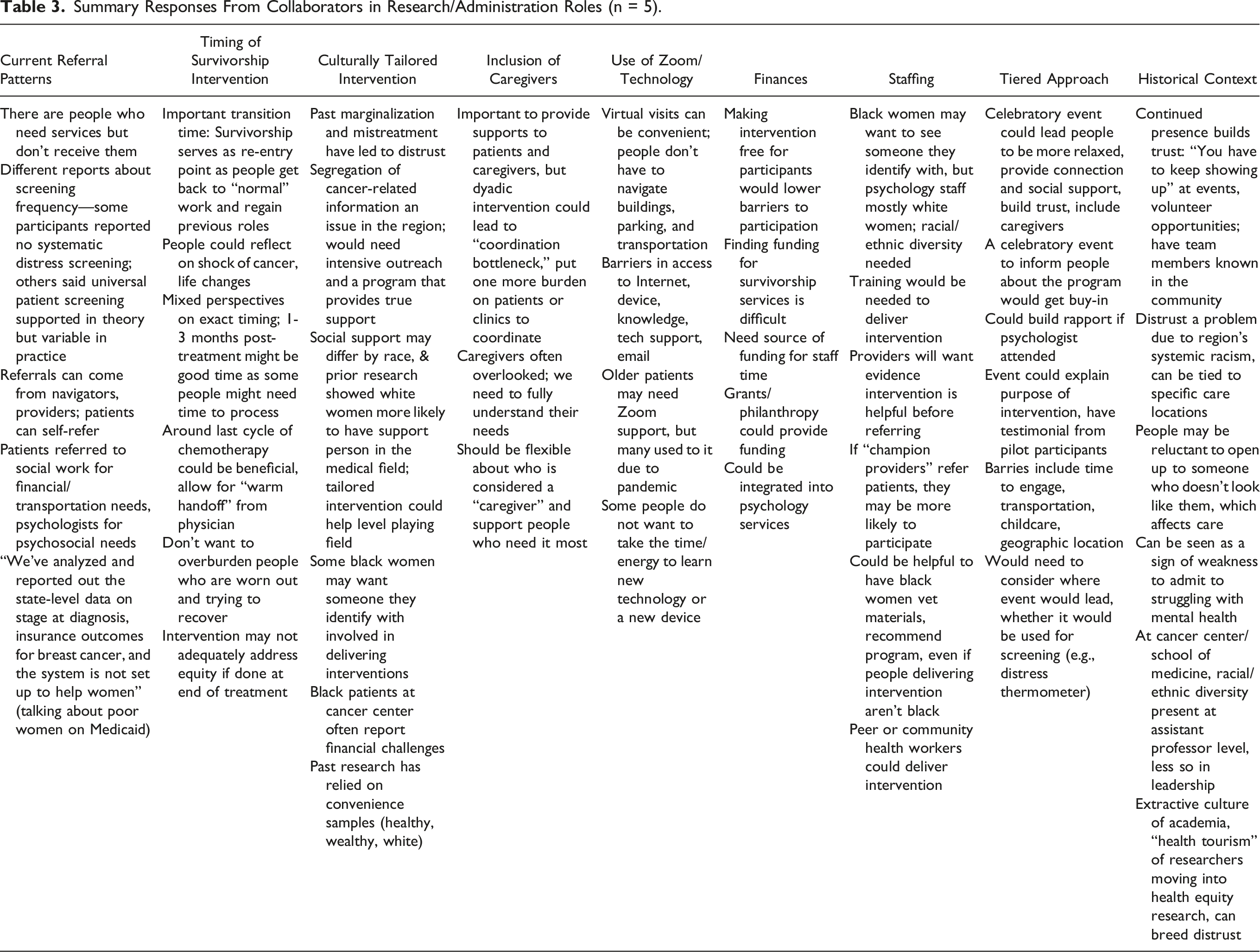
Summary Responses From Collaborators in Research/Administration Roles (n = 5).
Summary Responses From Collaborators From Community Groups (n = 2).

Current Referral Patterns
As recommended by others, 42 we used a broad opening question (about current screening and referral patterns at the cancer center) in order to put participants at ease and help our team understand current practices. Participants described a range of pathways for referring patients to psychosocial services; they said providers screen patients with the National Comprehensive Cancer Network (NCCN) distress thermometer, although they noted variability across providers in terms of the frequency of screening and the referral patterns afterwards. Most commonly, patients were referred to psychologists for psychosocial distress and social workers for unmet social needs (e.g., financial assistance, transportation help). Participants reported there is no systematic screening of caregivers; caregivers can be referred to services by providers (physicians, nurses, or navigators), self-refer, or be referred by patients. Across all four role groups, there was widespread agreement that there are “absolutely” people who need psychosocial services but do not receive them, especially Black women.
One person pointed out the complexity of the care delivery context: “There’s so many aspects to providing care here and so many people involved. The doctors are all very different and their approach is very different…. There’s a lot of personalities [involved] with the teams.”
Intervention Delivered Around Transition to Survivorship
Participants noted that the transition to long-term survivorship (i.e., end of active treatment) could be a good time to intervene because patients face new or unanticipated stressors. Participants said that, once initial treatment is complete, patients want to “get back to normal” and resume previous roles, but they noted a lack of current services to help with the transition. One noted that the completion of initial treatment could provide patients a chance to reflect on their journey, but others thought a potential barrier for a survivorship intervention could be that patients and caregivers might be eager to be done with treatment and reluctant to make additional appointments. They pointed out that a survivorship intervention would not address needs arising during treatment; one participant indicated that intervening once treatment was complete was not ideal for addressing health equity because such an intervention would exclude people who had not initiated or completed treatment.
Developing a Culturally Appropriate Intervention for Black Women and Their Caregivers
Participants saw benefits in developing an intervention specifically for Black women and their caregivers. They noted that Black patients tend to use psychosocial services less than other patients at the cancer center and often have higher unmet needs for financial assistance or transportation services. One MH participant noted that a culturally appropriate survivorship intervention could provide an additional invitation to access care. Several participants thought such an intervention could help address both mistrust of the medical system and stigma in accessing mental health care, particularly if the people delivering the intervention were also Black women.
Some participants pointed out that Black women in particular may be reluctant to ask for help in the context of cancer treatment because they may feel social expectations to project strength and care for their families rather than seek additional care for themselves. Participants shared their perception that Black women may rely on faith and family over formal mental health services and said some may prefer to keep their cancer journey private. Additionally, a CM participant noted that their organization’s listening sessions had shown that different communication strategies were needed to reach younger vs older Black women.
Historical Context
Participants presented a nuanced picture of the ways they believed the historical context of the region affects Black patients’ interaction with the healthcare system. Participants noted a long history of racial discrimination in the region that they believed might lead patients to mistrust the healthcare system, although one PH participant stated her Black patients had not reported a lack of trust and told her they were satisfied with the psychosocial care they had received at the cancer center. A few participants described how mistrust may be linked to historical experiences at specific care sites in the region. For example, one PH participant said that some of her patients preferred to see her at the main cancer center location (which historically served primarily white patients) as opposed to the satellite location in a predominantly Black area due to the perception that the main location provided better care. Some participants in RA and MH roles reported that patients’ mistrust may be directed at more at research conducted by the cancer center rather than health services. One RA participant pointed out that the school of medicine has a lack of diversity at the leadership level and said that the extractive culture of academia could result in patients not trusting researchers.
Participants generally agreed that building trust with Black patients and caregivers requires investments of time and sustained engagement. Some suggested that racial concordance between providers and patients could help build trust, and some noted that providers from all backgrounds should view the patient as “a whole person” and acknowledge the impact of the region’s systemic racism on their clients’ experiences as patients and in other areas of life. A CM participant suggested that partnering with community organizations that serve Black women could help foster trust among Black patients.
Inclusion of Caregivers
Participants across roles saw benefits to including caregivers in an intervention, and they agreed that caregivers are often overlooked. They said an intervention had the potential to address caregivers’ needs, facilitate communication and relationship outcomes within a dyad, coach the caregiver in helping the patient, and get both people on the same page. One PH participant noted that including caregivers could potentially increase patient attendance at appointments.
Challenges to including caregivers included finding ways to meet the diverse needs of support pairs with different types of relationships (e.g., friends, mother-daughter). MH participants pointed out that needs and treatment goals may vary for patients vs caregivers. Participants across roles noted that, depending on the dynamics of dyadic relationships, dyad members may be reluctant to open up emotionally in front of each other. From a logistical perspective, participants suggested it can be challenging to schedule two people; one RA participant mentioned concerns about a “coordination bottleneck” that could burden patients or clinics. Finally, participants across roles encouraged flexibility in defining who is a “caregiver,” as well as consideration about whether that terminology would resonate for potential intervention participants.
Use of Zoom/Technology
MH participants noted that psychologists at the cancer center were currently providing all outpatient services over Zoom, with telephone counseling used as a backup. Many participants described logistical benefits of telehealth for patients, including serving people from a broader geographic area and the fact that participants would not have to find transportation or pay for parking. One participant said that Zoom might mitigate challenges finding childcare but also noted that it could lead to issues around privacy within the home. Some participants said that older patients may need additional Zoom support but also noted that the pandemic had made many people more accustomed to telehealth. They pointed out that some people may not have consistent internet access, technology assistance, or an appropriate device (e.g., people may have pay-as-you-go phones that are not smartphones). An additional drawback noted is that people may see Zoom as impersonal or prefer to connect in person.
Program Finances
Relatively few participants reported having control over a budget that would fund interventions for patients or caregivers. Financial constraints tended to be addressed more indirectly through concerns about the staff time needed to deliver an intervention, institutional capacity, and sustainability. Participants suggested that grants or philanthropy had the potential to provide funding for an intervention, or an intervention could be integrated into current psychology services offered at the cancer center (and presumably be covered by that budget). Participants in mental health roles noted that Zoom is cost-effective for the institution because it is already in use; however, supplying devices to people who don’t have them so they could participate in an intervention could prove costly.
Staffing
MH participants said that the COVID-19 pandemic had helped them become very familiar with the technology and processes used for telehealth. They said that current staff have experience working with people from different backgrounds but are not racially and ethnically diverse as a group; collaborators said there is a need to address the mental health training pipeline and said there could be a need for additional training in cultural competency for current providers. Participants in PH and RA roles stated that it would be important to have buy-in from providers about the intervention so they would refer people for participation or serve as “champions” for the intervention.
Most participants across roles agreed that it would be desirable to have a more racially diverse staff at the psychology center, and that it could be helpful to have racial concordance between intervention staff and patients/caregivers. One participant who was a Black woman and a cancer survivor said, however, that she would feel just as comfortable with white staff members as Black staff members. Participants suggested that community health workers or peer support could complement the existing staff at the cancer center, and that at the very least it would be helpful to have Black women vet materials and recruit people for the intervention even if the interventionists themselves were not Black.
Tiered Approach
Overall, participants were supportive of the idea of a tiered approach in which a celebratory event could be used to draw people in and inform them about or connect them to services. People thought that starting with a free, celebratory event—preferably one that involved food—could help build connections and trust, include caregivers, minimize stigma, provide general information about survivorship, and inform people about the intervention, potentially through testimonials of participants in a pilot study.
Participants had questions, however, about how such a strategy would work in practice. Some expressed uncertainty about how mental health screening or referral would happen in a social context. There were concerns about how to promote attendance, as well as whether an in-person event would be appropriate for people who are immunocompromised. One MH participant expressed concerns about potential dual relationships (i.e., meeting people in a social setting and then seeing them as clients). MH participants pointed out that the frequency of one-time events could be a challenge, since they would have to be held fairly frequently to make them effective as a source of referrals. CM participants said it would be important to be thoughtful about the location of such an event and perhaps choose a venue other than a medical setting. One CM participant pointed out that skilled facilitation would be needed to validate people’s experiences but not allow only the “airing of grievances” or the sharing of medically inaccurate information.
Over-arching Themes
In addition to more straightforward responses to individual interview guide domains, our team identified three themes that cut across questions: gaps in care; the importance of representation in helping to build trust and reduce stigma; and systemic barriers to working with dyads.
Gaps in care
Participants noted several gaps in the care currently provided at the cancer center. They reported that support for patients “dissipates” around the transition to long-term survivorship, and there was widespread agreement that additional services around this transition could be beneficial. Likewise, there was widespread agreement that Black patients were not receiving mental health services at the cancer center in proportion to the number of Black patients treated for breast cancer. Finally, participants described how caregivers often “fall through the cracks” due to a lack of systematic screening, ad hoc referral patterns, and caregivers’ limited time and energy, as well as caregivers’ desire to focus on the patient.
The Importance of Representation in Helping to Build Trust and Reduce Stigma
Representation—the idea that people would receive a referral or services from “someone who looks like them”— emerged in response to several interview questions as an important strategy to combat mistrust and stigma around accessing mental health services. One Black PH participant, for example, described how her Black patients “brighten” when they discover they are receiving medical care from a Black woman. One white MH participant said she thought some Black patients would prefer disclosing information in the context of racially concordant psychosocial care, but she also pointed out that racial concordance is not necessarily taken into consideration in other contexts at the cancer center (e.g., physician care). Participants talked about the idea and benefits of representation in different ways; some used the term representation directly or talked explicitly about racial concordance as a means of building trust, while others seemed to assume that an intervention designed for Black women would be delivered by Black staff. There was widespread acknowledgement that the mental health providers at the cancer center are not currently racially and ethnically diverse, and that increasing diversity of the staff would be desirable. Several participants recommended ways to compensate for lack of staff diversity, such as incorporating community health workers into intervention delivery or employing Black women to help with recruitment, which suggests they may be accustomed to employing a range of strategies to provide culturally appropriate care in predominantly white spaces.
Systemic Barriers to Working With Dyads
Participants discussed health-system-level barriers to working with caregivers and patient-caregiver dyads. They described how the health system is set up to serve patients as individuals in terms of screening, referrals, scheduling, and treatment, which can make it difficult to integrate caregivers into services. This bias towards focusing on the patient emerged in the process of conducting the interviews as well; although many of the questions in the interview guide asked about both patients and caregivers, participants primarily discussed cancer care from the perspective of the patient only. The study team also discussed how the conceptual model guiding this study (the Health Equity Implementation Framework) is patient-focused as well and does not explicitly incorporate caregivers.
Discussion
To our knowledge, this is the first study to solicit insights from collaborators from a comprehensive cancer center and community organizations about facilitators and barriers to implementing a dyadic intervention for Black breast cancer survivors and caregivers. These findings have implications the development and implementation of dyadic and culturally appropriate interventions in healthcare contexts. Our analysis using the Health Equity Implementation Framework 41 points to factors at multiple levels that may affect intervention delivery. Collaborators were generally supportive of the idea of an intervention for Black women and their female caregivers delivered remotely around the time of transition to long-term survivorship; they believed it was important to provide high-quality care to patients and caregivers, and they described a setting in which mental health providers are already well-equipped to provide care via telehealth. At the same time, they described significant barriers to intervention delivery. We identified three over-arching themes related to intervention design and implementation of dyadic interventions for this population: the need to address gaps in care; the importance of representation in building trust and mitigating stigma; and the challenges within the healthcare system around providing care services to dyads.
Consistent with prior research, study participants described gaps in care for caregivers, Black women with breast cancer, and longer-term cancer survivors. Prior work has shown that caregivers are often not incorporated into cancer care in any standardized or systematic manner.30,34,50 Others have also reported a lack of psychosocial interventions designed for Black women with breast cancer 51 and for their caregivers. 31 In addition, the transition to long-term survivorship has been noted as a time at which survivors and caregivers could benefit from additional services.11,19,52 Taken together, participants’ responses underscore the need to continue developing outreach strategies and supportive interventions to address these gaps. Psychosocial interventions that are integrated into clinical care, such as the dyadic Zoom intervention that our team is developing, have the potential to fill these gaps and address survivors’ and caregivers’ needs during the transition to long-term survivorship.
Collaborators described representation as an important strategy for building trust and mitigating stigma around accessing mental health care. This finding is consistent with a prior review showing that racial concordance is associated better patient-physician communication across several domains. 53 Participants believed a history of racism in the region (and nationally in the U.S.) had led to mistrust among Black patients, and many stated that having Black women provide referrals or deliver a psychosocial intervention for Black women with breast cancer could help overcome this lack of trust. Many believed such racially concordant staffing might mitigate perceived stigma around accessing mental health care, but there was also an acknowledgement that current staffing at the cancer center often precluded racially concordant care for Black patients and caregivers, even when patients or caregivers might prefer such care.
The suggestion that some Black patients may avoid care sites in historically Black communities due to perceived low quality of care complicates the idea of representation, especially in the context of disinvestment in predominantly Black communities. 54 Others have suggested a two-pronged strategy to build trust in healthcare settings that involves (1) helping providers from all backgrounds deliver relationship-centered care, while also (2) building “structural competency” to address disparities, including deliberate attempts to diversify the healthcare workforce and leadership. 55 Such strategies are consistent with prior research in which Black breast cancer survivors described desiring culturally competent care from healthcare providers that demonstrates empathy, respect, and acknowledgement of their humanity. 23
Participants described health system barriers to including caregivers in cancer care that could affect the uptake of dyadic interventions intended to be embedded in the healthcare system. They described healthcare systems that focus on individual patients in terms of screening, referrals, and treatment. In addition to these findings, as we analyzed data our team was struck by the fact that our conceptual framework (the Health Equity Implementation Framework 41 ) did not explicitly include caregivers. We chose the Health Equity Implementation Framework because it focuses on the social context and addresses factors at multiple levels that may perpetuate or ameliorate health disparities. At the same time, the framework centers the clinical encounter without explicitly depicting how to incorporate non-clinical caregivers or considering the dyad, rather than the individual, as the unit of analysis. Although prior work has shown that “patients” and “caregivers” in a dyad may move back and forth between both roles, 10 in the context of cancer treatment, “patients” and “caregivers” have very different relationships to and roles within the health care system, including access to services to address their own care and wellbeing. Patients have medical records at the cancer center, but caregivers may not (or, if they do, they are not linked to the patient’s).35,36,50 Patients receive at least occasional routine distress screenings, but caregivers often do not. 50 The mental health providers at the cancer center did offer services to caregivers through one-on-one sessions and support groups, but those services did not address patients and caregivers as a unit. Reblin et al found that caregiver support falls outside of a cancer center’s usual care delivery process 34 ; we extend that finding and note that serving dyads as a unit may fall outside a cancer center’s care delivery process as well. As cancer centers face growing calls to incorporate caregiver services into their care delivery processes,11,35 providers and staff must continue to refine workflows and referral patterns to include caregivers and patient-caregiver dyads. A recent proposal to create a national Caregiver Support Accelerator could support cancer centers across the U.S. as they assess their workflows and day-to-day operations and assist them in implementing interventions for caregivers and patient-caregiver dyads. 35
To guide future work, we suggest that the Health Equity Implementation Framework and similar frameworks could be broadened to depict patients and caregivers or other family/friends. For the Health Equity Implementation Framework, one potential way to include caregivers would be in the “other people” section of the framework; although “other people” are conceptualized by the creators of the framework as “individuals who affect the delivery of an innovation, such as a clinic manager, quality assurance administrator, or clerk” 41 (p. 6), the concept could be extended to include caregivers or others in a patient’s support network. Another potential opportunity for inclusion would be to broaden the “patient” framing and include caregivers as integral recipients of the intervention and key parts of the clinical encounter.
The Health Equity Implementation Framework could also be used to guide the development of future structural interventions that could complement individual-level and dyad-level psychosocial interventions. Our questions about current screening and referral patterns revealed considerable variability from clinic to clinic even within the same cancer center; structural interventions (e.g., universal caregiver screening, targeted navigation for high-risk patients) may also be necessary for reducing and ultimately eliminating health disparities. 54 Using a structural lens may also be useful when considering ways to increase racial and ethnic diversity in staffing. For example, a lack of diversity among staff is perhaps unsurprising when psychosocial care is provided primarily by clinical psychologists, since Black people make up only 4% of psychologists in the workforce 56 ; including additional types of providers (e.g., social workers, peer coaches) is one potential pathway for increasing racial/ethnic diversity. Addressing factors at multiple levels has the potential to promote “structural competency” and reduce health disparities. 55
This work has several strengths. We used an equity-focused framework to interview collaborators and “design for dissemination.” Our team-based analysis was highly coordinated, and we developed themes with implications for culturally appropriate and/or dyadic interventions in health care settings more broadly. During our iterative analysis process, we discussed and revised themes, returning frequently to the data to verify our findings.
This study also has limitations. Although rapid qualitative analysis was appropriate for our research questions, it may miss nuances that could be illuminated by more traditional qualitative methods. 45 Our sampling strategy was based on including professional collaborators from a single metropolitan area, and thus we did not intentionally sample Black patients and caregivers in this collaborator-focused recruitment (although we had Black women in our sample who identified as one or both). We are in the process of conducting separate dyadic interviews to elicit patient and caregiver perspectives and preferences for intervention. For the most part, our participants addressed the needs of female patients, but they did not specifically address the pros and cons of an intervention for female caregivers (vs support people of other genders); the team realized during analysis that it would have been beneficial to probe this topic further and encourage participants to address it more thoroughly.
Conclusion
This study is one of the first to examine facilitators and barriers to implementation of dyadic cancer survivorship interventions for Black women with breast cancer and their caregivers. These findings provide important data highlighting the potential benefits of survivorship interventions for both patients and caregivers, as well as for Black women in particular. Application of these findings can lead to successful implementation of dyadic survivorship interventions for Black women with breast cancer and their caregivers in clinical settings. Participants described systemic barriers to working with dyads that would need to be addressed in order integrate dyadic interventions into clinical care. Participants described how Black women in particular are often underserved in cancer care settings, and they suggested strategies to build trust and extend outreach. Participants’ discussions about the historical context locally and nationally indicate that structural interventions (e.g., implementing universal caregiver screening, working to diversify the cancer care workforce) could complement psychosocial interventions in addressing health disparities. Expanding implementation models such as the Health Equity Implementation Framework to include caregivers could help apply these findings and focus dissemination and implementation efforts on both members of a dyad. The ultimate goal of this intervention development work is to create and disseminate effective interventions that will improve health and psychosocial outcomes for patients and their loved ones as they face cancer together.
Footnotes
Acknowledgements
We thank our colleagues who shared their insights in these interviews, and we are grateful to Drs. Charlene Caburnay and Amy McQueen for their assistance with this project.
Author Contributions
Tess Thompson (conceptualization, methodology, formal analysis, investigation, resources, writing—original draft, writing—review and editing, supervision, project administration, funding acquisition); Christi Lero (methodology, formal analysis, investigation, writing—original draft, writing—review and editing); Julia Levitan (methodology, formal analysis, investigation, writing—review and editing); Cory Bradley (conceptualization, methodology, formal analysis, writing—review and editing); Aimee James (conceptualization, writing—review and editing); Katie Heiden-Roots (conceptualization, writing—review and editing); Emani Sargent (writing—review and editing); LaShaune Johnson (conceptualization, formal analysis, writing—review and editing).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was funded by R03CA273485 (PI: Thompson). Christi Lero’s time was supported in part by T32MH19960-29 (National Institute of Mental Health) (PI: Cabassa), and Aimee James was supported by the Siteman Comprehensive Cancer Center and NCI Cancer Center Support Grant (P30 CA091842). This research was also supported by the Washington University Institute of Clinical and Translational Sciences (grant UL1TR002345 from the National Center for Advancing Translational Sciences of the National Institutes of Health [NIH]).
Ethical Statement
Semi-structured Collaborator Interview Guide
Note: This interview guide was used to conduct one-on-one interviews with participants via the university’s HIPAA-compliant Zoom platform. Participants were informed that the interview was being recorded and were told they were free not to answer any questions that they did not want to answer.
Thanks so much for agreeing to talk with us today. As we mentioned, we are talking with stakeholders at the cancer center and in the community about developing an intervention for Black women with breast cancer and their female support people that would be delivered after patients had finished their initial treatment. We want to know what would make this intervention an exciting and feasible addition to the resources currently available for patients and caregivers. 1. Could you start by telling me a bit about your [professional/community] role? What involvement do you have with planning, delivering, or referring patients or caregivers to resources related to mental health or cancer survivorship? (Probe for details: Amount of time in role, interactions with patients or caregivers, oversight of staff or budgets, reporting structure within the department, etc.) 2. Can you walk me through the process of how breast cancer patients and caregivers currently access psychosocial services? (Probe: Who screens or refers? Are there multiple screening/referral pathways? Do you think some people who need services don’t receive them?) 3. We are developing an intervention to serve Black women and their female support people. What do you anticipate will be the benefits of providing services specific to their needs? What do you anticipate might be the challenges of providing services specific to their needs? What are the benefits and challenges of providing supports to both patients and their support people? (Probe for whether it might be better to help people separately or together, as well as institutional constraints) 4. The intervention we’re envisioning would be delivered by psychologists at the cancer center via Zoom once patients are finished with their initial treatment. What do you think would be the pros and cons of this approach? Probes based on interviewer discretion—will vary depending on participant’s role: • Technology: Limitations/concerns for using the technology in general, and at the cancer center in particular—what in your opinion puts the cancer center at an advantage for this delivery format? What would be limitations or concerns at the cancer center? • Finances: What kind of financial resources would be needed? • Staffing: Some of the Black women we’ve talked to have said they’d be most comfortable if the people delivering the intervention are Black women as well. Is that currently possible at the cancer center? Do you think existing staff would need additional training? Would peer or community health workers be effective? • Timing: What are the pros and cons of delivering an intervention around the transition to long-term survivorship? 5. In addition to a videoconferencing intervention, our team has also talked about a more tiered approach that could draw in a larger number of people and then connect them to resources if needed. For example, some of our study participants have suggested one-time events such as lunches or celebrations that would allow patients and caregivers to relax and have fun together. Could you think of ways that single events like this might be used to inform them about available resources or screen them for unmet needs? What would be the pros and cons to using single events to draw people in rather than immediately starting with a multi-session intervention? 6. We know that interventions are affected by the delivery context. The [metro area] has a long history of racial discrimination that may affect Black residents’ trust in the health care system in general or in the cancer center in particular. Do you think a lack of trust affects whether Black patients and their support people are willing to engage with psychosocial services or survivorship services at the cancer center? If so, what steps do you think people at the cancer center or the health system could to take to build trust? 7. Before we wrap up, is there anything you thought we would be discussing that we haven’t touched on? Is there anything you’d like to add about providing psychosocial support for Black women with breast cancer and their support people?