
Abstract
The conditions in which people are born, live, learn, work, play, worship, and age affect a range of health, functioning, and quality-of-life outcomes, and contribute to social needs across the cancer control continuum. To address these needs, advance the quality of cancer care, and achieve health equity, cancer care clinicians must possess comprehensive knowledge and skills to mitigate the effects of social determinants of health on patient outcomes. This knowledge should also encompass an understanding of how racism, sexism, and discrimination – along with exposures to trauma – also influence patient behaviors and outcomes, given evidence of their effects on population health. For over 100 years, social workers have comprised an essential workforce that is duly educated and trained to identify social needs and improve patient outcomes within the context of health care service delivery, and cancer care in particular. Oriented to an ecological framework, social workers are adept at identifying and mitigating the negative effects of the social determinants of health on individual knowledge, attitudes, beliefs, and behaviors, with the intent of improving results for people at risk for or diagnosed with cancer. Social workers are professionally trained for organizing communities, understanding and intervening upon social systems (including families, organizations, and institutions), providing emotional support and mental health counseling, and advocating for programs and policies that best serve patients, families, and communities. Thus, social workers play a critical role in service delivery across the cancer control continuum.
Plain Language Summary
Social workers play an underappreciated yet essential role in health care and in cancer care, specifically. Given growing interest in social factors that influence disease and the need to address social conditions as they influence cancer care and outcomes for cancer patients, we argue that social workers are critical, and that they have been attending to the social needs of individuals and families in the context of medical care for over 100 years.
Introduction
The literature on Social Determinants of Health (SDoH) and their link to human behavior, health outcomes and disparities has gained renewed attention since the turn of the 21st century.1,2 The conditions in which people are born, live, learn, work, play, worship and age affect a wide range of health, functioning, and quality-of-life outcomes and risks and contribute to social needs across a cancer control continuum that initiates with screening and early detection, and continues through phases of disease onset, diagnosis, treatment, and subsequent transitions to post-treatment survivorship or for some the end of life. For example, the American Cancer Society has reported “substantial variations in risk factors, stage at diagnosis, receipt of care, survival, and mortality for many cancers by race/ethnicity, educational attainment, and metropolitan status (pp. 136).” 3 Similarly, known health-determining factors such as food insecurity, 4 socioeconomic status, 5 insurance status, 6 social isolation, 7 and geographic distance to comprehensive cancer centers 8 have been repeatedly associated with timely cancer screening, access to novel therapeutics, quality of cancer care, and distal health outcomes including morbidity and mortality.
In 1905, physicians at Massachusetts General Hospital recognized the manifestations of social stressors in their patients and their implications for service delivery and patient outcomes. They also recognized that they, as physicians, lacked a comprehensive set of clinical skills and knowledge base to fully address these social effects in the context of medical care. As a result, they hired Garnet Pelton and Ida Cannon as the first social workers to be employed by a U.S. hospital. Their charge: to assess and address the deleterious effects of social factors -- the social determinants (or drivers) of health -- on patient behavior and outcomes. 9 For over 100 years, social workers have comprised an essential workforce that is duly educated and trained to identify social needs and improve patient outcomes within the context of health care service delivery, and cancer care in particular.
Leading organizations such as the National Cancer Institute, the National Cancer Policy Forum, the American Society of Clinical Oncology, and the National Academies of Sciences, Engineering, and Medicine (NASEM) have emphasized the importance of identifying effects of SDoH and addressing patients’ health-related social needs in the clinical care setting.10-12 While physicians are calling upon themselves to spend more time with patients and get to know them as a “whole person” as a way to respond to their social needs, 13 we argue that social workers are trained to lead as a member of an oncology care team and bear clinical responsibility for assessing and addressing patients’ social and mental health needs.
Disparities in population health as well as in clinical outcomes for cancer patients are evident across population sub-groups including but not limited to those defined by race/ethnicity, sexual orientation and gender identity (SO/GI). These disparities have been observed and documented for years. 14 For example, Black Americans continue to have the highest cancer mortality and the second shortest survival time among racial/ethnic groups (with the exception of American-Indian/Alaska-Natives), reflecting a striking survival disparity between Black and White Americans. 15 Similarly, individuals who identify as Lesbian, Gay, Bisexual, Transgender, and/or Queer (also referred to as Sexual and Gender Minority – SGM) have been increasingly recognized as an underrepresented and underserved cancer cohort, as evidenced by cancer care and screening guidelines that do not offer guidance on how to mitigate the effects of social and environmental stressors imposed on individuals from marginalized populations. These shortcomings result in delays in cancer diagnosis and treatment and, in turn, compromise patients’ outcomes. 16 In short, SDoH influence individual health and well-being across cancer control domains.
To achieve health equity and advance the quality of cancer care, a cancer care team must possess comprehensive knowledge about, and skills to mitigate the effects of SDoH. This knowledge should also encompass an understanding of how racism, sexism and discrimination – along with exposures to trauma – influence patient behaviors and outcomes, especially given evidence of their effects on population health.17,18
What do Oncology Social Workers do?
Oncology Social Work Practice Behaviors 21
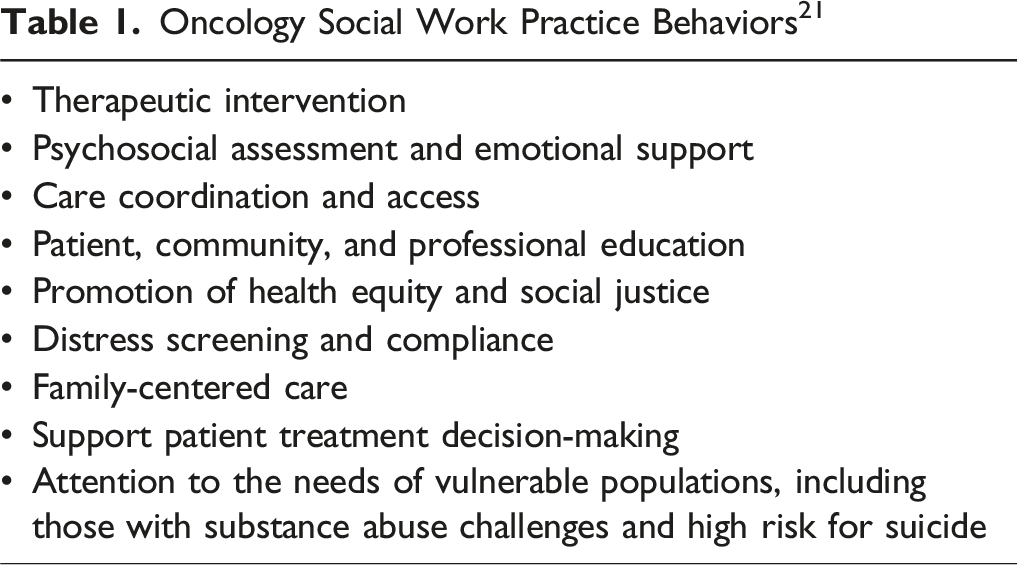
With regard to the cancer control continuum, social workers are employed as community health workers engaged in cancer prevention and screening activities at local community levels, like health fairs or home visits, that are intended to facilitate access to health care services (e.g., mammography, Human Papillomavirus [HPV] vaccination). Proactive programming to educate communities about cancer risks and mitigation strategies is a core element of social work, which in this context involves community-based health awareness and promotion activities addressing risks related to smoking or exposures to environmental carcinogenic exposures (which are concomitant with the climate crisis). Other community-based activities revolve around dissemination of resources for disease prevention education, access to healthy food and health education, access to prevention and early detection services such as mammography or genetic screening.22-24
Throughout phases of diagnosis, treatment, and transition to post-treatment survivorship, and in collaboration with the care team, oncology social workers coordinate structured family meetings to facilitate communication and resolve conflict, assist with patient decision-making related to treatment options, and proffer access to federal, state, and community-based resources. 25 The social workers’ role on the multidisciplinary team is dynamic and includes patient care coordination through letters, phone calls, or electronic health record messages, or referrals to other ancillary care services, including psychiatry or behavioral medicine, mental health counseling, chaplaincy and spiritual support, or financial resources. 26 They apply evidence-based interventions known to facilitate patient adherence to therapy, satisfaction with care, and even survival, including cognitive behavioral therapy (CBT), psychoeducation, and support groups to help patients adjust to illness.27-30 Upon completion of therapy, social workers facilitate patient transitions to post-treatment medical surveillance and survivorship care. 31 They also support patient and family social adjustment after cancer, which may include addressing unique to post-treatment cancer survivors, such as family building.32,33 For patients facing the end of life, social workers support family members to ensure patient comfort and dignity in life’s final stages and address issues related to grief and bereavement. For example, social workers facilitate “legacy work” to help patients and families create memory books or videos for their loved ones. 34
The future is ripe for considering innovative approaches to oncology social work in terms of alignment with activities that can lead to the restorative allocation of resources directly to the communities where patients and their families live, work, and receive health care. Realizing the need for guidance on integrating social care into the delivery of health care, NASEM has advanced five categories of health and social care integration activities upon which to focus efforts to enhance health care delivery (Table 2).
12
Social workers are adept and well-trained to engage in activities across each of the 5 As categories: • • • • • 5 As Model for Health and Social Care Integration Activities
12

Opportunities for Interprofessional Collaboration in Research
Oncology social work researchers stand to lead scientific efforts when it comes to SDoH and the redress of health-related social needs. A core construct for social work is the “person-in-environment”
35
in which individual outcomes and behaviors are examined within a broader ecology in which social conditions, networks, systems, rules, laws, policies and even historical eras and time (Figure 1).
36
With the emergence of precision medicine, genetic profiling, and cutting edge immunotherapy, a current NCI-funded research study serves as an example of how social work researchers have applied a social ecological perspective in the conceptualization and conduct of a scientific investigation. In this case, social work researchers are leading and collaborating with clinical oncologists, psychologists, genomic scientists, epidemiologists, biostatisticians, and patient advocates in a transdisciplinary fashion to examine the biological mechanisms by which social and environmental risk and resilience factors, such as social support/isolation, exposures to trauma, or experiences of racism or discrimination may affect treatment outcomes.
37
Social Ecological Context for Understanding Individual Outcomes and Behaviors
36

Oncology social workers also are uniquely poised to lead technology-assisted intervention research supporting cancer survivors and their family members. Again, a social-ecological framework serves as rationale for integrating SDoH into the design, development, evaluation, and implementation of a tech-assisted multilevel intervention to achieve accessible and sustainable behavior change. In this example, social work researchers are evaluating the clinical utility of an artificial intelligence (AI-) enabled distress monitoring tool for adolescents and young adults with cancer. 38 With the advancement of AI algorithms, the technological precision of detecting cancer patients’ psychological distress will continue to improve. However, it is arguably important that the research community attend to the applicability of developed AI algorithms as well as the acceptability of these developed technological platforms among underrepresented populations.
There certainly are challenges to the actualization of transdisciplinary research in cancer care. These include overcoming reliance on jargon to achieve clear communication and information sharing across professional disciplines, hierarchical power dynamics that can repress innovation and initiative, and a lack of clarity around professional role delineation. 39
Conclusion
Social workers are professionally trained for organizing communities, understanding and intervening upon social systems (including families, organizations, and institutions), providing emotional support and mental health counseling, and advocating for programs and policies that best serve patients, families, and communities. Oriented to an ecological framework, social workers are adept at identifying and mitigating the negative effects of these conditions on individual knowledge, attitudes, beliefs and behaviors with the intent of improving outcomes for people at risk for or diagnosed with cancer. Given that cancer is not solely a biological or medical issue but also a condition that involves a complex interplay of biological, social, and psychological factors, we suggest that institutions, funders and policymakers be aware of the vital role that social workers play across the cancer control continuum.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.