
Abstract
Background
Liver cancer (LivCa) is one of the most prevalent malignancies globally, and can result from viral hepatitis, non-alcoholic steatohepatitis (NASH), and alcohol use. LivCa is of increasing concern in Asia, but the burden of etiology-specific LivCa and future projections remain to be elucidated.
Methods
We extracted the incidence, mortality, and disability-adjusted life years (DALYs) of LivCa across Asia and in 34 Asian countries in 1990-2021 from the Global Burden of Disease Study 2021 (GBD 2021). We then calculated their estimated annual percentage change (EAPC) and percentage variation to quantify the changes in the burden of LivCa. The association of the level of social development with LivCa burden was explored using the sociodemographic index (SDI). Moreover, the trend of the epidemiology of LivCa burden in Asia from 2022 to 2040 was predicted using the Bayesian age-period-cohort (BAPC) model.
Results
Overall, the age-standardized incidence, mortality, and DALYs rates of LivCa in Asia showed a general declining trend, with EAPCs of -0.47, -0.73, and -1.14, respectively. Notably, hepatitis B virus remained the predominant cause. However, the burdens attributed to non-alcoholic steatohepatitis and alcohol use increased significantly, while that of hepatoblastoma decreased. Regarding demographic distribution, the highest disease burden was observed among males and the elderly population aged 85–94 years. Geographically, Nepal, Taiwan (Province of China), India, and Malaysia contributed most substantially to the increasing burden. In terms of risk factors, high BMI and alcohol use were prominent in Central Asia, whereas smoking was a key factor in East and Southeast Asia. Additionally, a positive correlation was observed between the SDI and the burden of LivCa. Finally, projections from the BAPC model indicated a persistent decline in the burden of LivCa from 2022 to 2040.
Conclusions
Despite the overall decreasing trend, targeted strategies addressing etiology-specific risks and regional disparities are urgently needed to further reduce the future burden of LivCa in Asia.
1. Introduction
Liver cancer (LivCa), including primary LivCa and hepatoblastoma (a distinct and rare type), is the first cause of death in patients with cirrhosis and chronic liver disease, and one of the most prevalent malignancies globally, which puts a heavy public health, clinical resource, and economic burden on the entire society and the healthcare system worldwide due to high incidence and mortality. Hepatoblastoma is the most common type of LivCa in children, with an extremely low incidence and accounting for 1% of all childhood cancers.1-3
As revealed by the Global Cancer Observatory, primary LivCa was the sixth major cancer globally in 2020, with 905,677 new cases, which rose by 21.1% as compared to the figure (748,000 cases) in 2008. It was also the third leading cause of cancer-related deaths, resulting in 83,180 deaths, with a 19.5% increase from 69,500 deaths in 2008, and it ranked fifth in global incidence.4,5 In addition, both incidence and mortality of LivCa are far higher in males than in females in the vast majority of regions, especially in countries of economic transition, where the incidence of LivCa in males is 2.4 times higher than in females. 4
This substantial global burden is driven by the complex etiology and heterogeneous pathological subtypes of LivCa. For primary LivCa, the main subtypes include hepatocellular carcinoma (HCC, 75-85%), intrahepatic cholangiocarcinoma (CCA, 10-15%), combined HCC-CCA (<5%), and other rare types such as fibrolamellar hepatocellular carcinoma.4-7 The major risk factors include chronic hepatitis B virus (HBV) and hepatitis C virus (HCV) infections, alcoholic fatty liver and alcoholic liver disease (ALD) due to excessive alcohol consumption, exposure to aflatoxin B1, non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) due to type 2 diabetes or obesity, and genetic factors.4,8-12 A study on the burden of LivCa in adolescents showed significant decreases in the incidence and mortality of LivCa in 5-24-year-old adolescents in 2000-2021 globally, but HCV, NASH, and alcohol use, except HBV, all became more important contributors to LivCa incidence. 13 These findings reveal the complex etiology behind different types of LivCa. Therefore, we should further explore the impact of different causative factors on LivCa so that more precise strategies for prevention and treatment can be adopted.
The incidence of LivCa greatly varies across the world. Previous research has suggested that East Asia, occupying 21.5% of the world’s population, is responsible for more than half of the estimated global cases (54.3%) and deaths (54.1%) of LivCa, with China as the main contributor. 14 In 2020, the age-standardized incidence rates (ASIRs) per 100,000 population for LivCa were the highest in East Asia and North Africa, especially Mongolia (85.6) and Egypt (34.1). In Southeast Asia, Cambodia (24.3), Vietnam (23.0), and Thailand (22.6) had far higher ASIRs. In contrast, ASIRs were far lower in Central and South America, the U.S., and Central and Eastern Europe. 5
In Asia, the incidence and mortality of LivCa remain regionally high due to high prevalence of HBV, aflatoxin contamination resulting from climate and diet, endemic schistosomiasis, smoking, alcohol use, and lack of screening due to economic backwardness or excessive health burden.15-20 For example, the major risk factors for LivCa are liver fluke infections in Southeast Asia, chronic HBV infection in China, and chronic HCV infection in Japan.21,22 In Western countries (e.g., the United States) where the risk of LivCa is also high, however, HCV, smoking, alcohol use, obesity, and diabetes are the primary contributors to LivCa. 21 As neonatal HBV vaccination and horizontal prevention are implemented, and clinical management of chronic hepatitis advances, the incidence of LivCa and the associated health burden have declined in parts of Asia. 23
Great efforts have been made in LivCa prevention and treatment in most Asian countries, but the incidence of LivCa caused by metabolic syndrome, obesity, and NAFLD due to alcohol use and smoking is rapidly rising in Asia. Therefore, the overall trend of LivCa and the impact of specific etiology on the LivCa burden remain to be deeply explored. 23 Overall trends of LivCa have been examined, but more comprehensive, etiology-specific analyses and future projections of the LivCa burden across Asian countries and regions are still lacking. Using the data from the Global Burden of Disease Study 2021 (GBD 2021), this study intends to assess the changes in the burden of etiology-specific LivCa across Asia and in different Asian countries in 1990-2021, as well as the projections to 2040. The findings are expected to offer theoretical guidance and practical reference for cancer prevention and control in Asia.
2. Methods
2.1. Data Source and Disease Definition
Data on LivCa were acquired from the GBD 2021, a database that presents up-to-date estimates for the burden of 371 diseases and injuries and the epidemiology data of 288 etiologies in 21 regions, 204 countries and territories, and 811 local administrative (subnational) regions in 1990-2021. The major indicators incidence, mortality, disability-adjusted life years (DALYs), and age-standardized rates (ASRs) were sourced from censuses, vital registration systems, disease registries, investigations, and scientific literature. To guarantee data availability, sophisticated scientific statistical models were utilized for standardized processing.24,25 The GBD is designed to quantify the burden of health due to diseases, injuries, and risk factors across regions, populations, and time, making it an important tool for prioritization of global public health policy, resource allocation, and monitoring of the sustainable development goals.24,25
The criteria for attributable risk factors are directly from the GBD, which perform the following steps within a comparative risk assessment framework: incorporating risk-outcome pairs into analysis; estimating relative risks as exposure functions; estimating exposure levels and distributions; determining the exposure level with the lowest theoretical risk; calculating population attributable fractions and burdens; estimating the mediating effects of different risk factors on others to calculate the burden of various risk factor combinations. 26
In the GBD 2021, primary LivCa is defined by the International Classification of Diseases (ICD) codes C22.0-C22.8 and portions of C22.9 in the ICD-10, including all types (e.g., hepatocellular carcinoma, hepatoblastoma). Hepatoblastoma is defined by C22.2 in the ICD-10. Other types of LivCa are classified based on the etiology; for example, LivCa caused by NASH, alcohol use, HBV, and HCV is defined by C22.0-C22.8 and portions of C22.9 in the ICD-10, but distinguished by their etiologies.5,13 Additionally, “Liver cancer due to other causes” is a residual category classified by the GBD classification system. It primarily covers other known or potential etiological factors of LivCa besides the above four major etiologies, including liver fluke infection, aflatoxin exposure, and obesity.
Directly using the GBD result tool GHDx (https://ghdx.healthdata.org/), the estimates of incidence, mortality, DALYs, and ASRs for LivCa across Asia and in 34 Asian countries in 1990-2021 were extracted, including their 95% confidence intervals (CIs). The reporting of this study conforms to the GATHER guidelines.
The sociodemographic index (SDI), a composite indicator commonly used in GBD published by the IHME in 2015, is calculated by the total fertility rate for people aged below 25 years, the mean educational level for people aged ≥15 years, and lag-distributed income per capita. SDI ranges from 0 (the highest fertility, lowest educational level, and lowest income per capita) to 100 (the lowest fertility, highest educational level, and highest income per capita). 204 countries and territories were categorized into low, middle-low, middle, middle-high, and high SDI.24,27
DALYs (total healthy life years lost from disease onset to death, Years of Life Lost + Years Lived with Disability) are a core measure for quantifying the burden of diseases, injuries, and risk factors24,27:

All data passed the ethical review by the University of Washington Institutional Review Board.
2.2. Statistical Analysis
The changing trends in ASRs over specific time periods were analyzed by the estimated annual percentage change (EAPC). It is calculated by fitting the natural logarithm of the regression model, with time as the variable, fitting the natural logarithm of each observation to a straight line, and plotting the slope of this line.28,29



In response to different study preferences, the GBD 2021 has a hierarchy of risk factors, with behavioral, environmental, occupational, and metabolic factors as the primary risk factors. 26 This study focused on behavioral (smoking, alcohol use, and drug use) and metabolic factors (excessively high BMI and high fasting glucose).
The burden of LivCa across Asia and in 34 Asian countries from 2022 to 2040 was predicted using the Bayesian age-period-cohort (BAPC) model:

2.3. Ethical Statement
This study is a secondary analysis of exclusively aggregated, anonymized data from the GBD database, which contains no individual identifiers. No human subjects were directly involved, and no primary data collection was conducted. Similarly, no animal experiments or animal-derived data were used in this research. All original datasets were generated in compliance with the ethical standards of the institutions involved and adhered to the principles outlined in the Declaration of Helsinki. Therefore, Institutional Review Board (IRB) approval and Institutional Animal Care and Use Committee (IACUC) approval were not required for this study.
3. Results
3.1. Burden of LivCa
3.1.1. Variations Across Asia
The Burden of LivCa Stratified by Different Regions and Countries in 1990 and 2021

UI: uncertainty interval.
The Burden of LivCa Stratified by Different Etiologies in 1990 and 2021
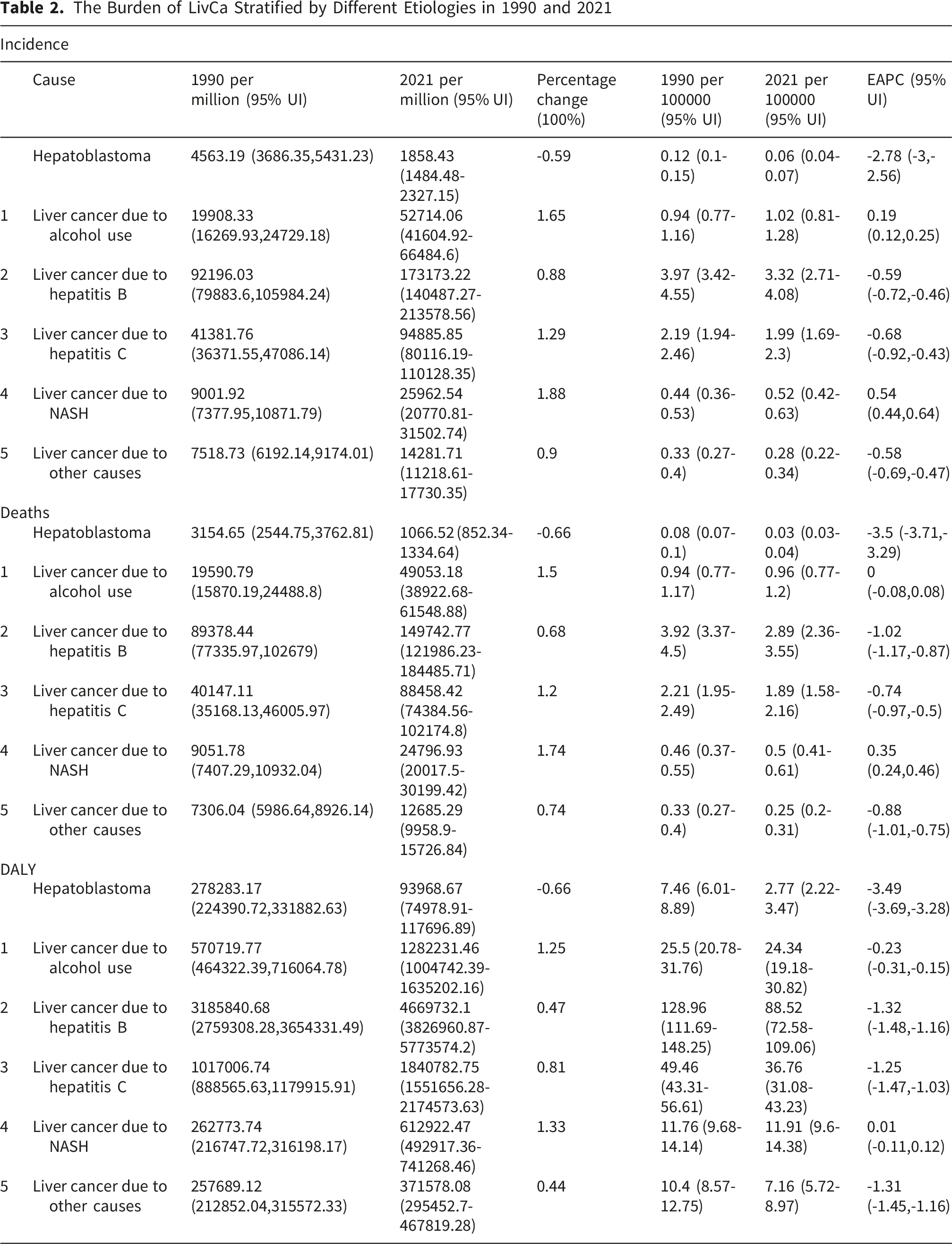
In 2021, the proportion of hepatoblastoma cases was 0.77%, and alcohol use, HBV, HCV, NASH, and other factors were responsible for 14.23%, 46.17%, 27.7%, 7.24%, and 3.89% of the primary LivCa burden in Asia, suggesting that HBV remained the leading cause of LivCa in Asia. In East Asia, represented by China, HBV even accounted for over 60% of LivCa. Hepatoblastoma, Alcohol use, HCV, and NASH were the largest contributors to primary LivCa in Thailand (30.9%), Japan (67.89%), and India (13.82%), respectively, and the proportion of hepatoblastoma cases was the highest in Pakistan (3.13%) (Figure 1). Mortality and DALYs of LivCa caused by other factors in Asian countries are detailed in Figure S1-S2. Percentage of hepatoblastoma and primary LivCa incidence caused by five different etiologies in Asia in 2021
3.1.2. Variations Across Regions
However, ASIRs greatly rose in Taiwan (Province of China) (EAPC=2.24, 95% CI 1.41, 3.07) and Nepal (EAPC=2.27, 95% CI 1.98, 2.56), far higher than in other Asian countries (Figure 2A). From the perspective of percentage variations, the burden of LivCa was high in India (228%), Nepal (299%), and Malaysia (299%) (Figure 2B). Notably, the percentage variation was -37% in Kazakhstan (EAPC=-3.33, 95% CI -3.62, -2.98), and ASIRs also sharply declined. The percentage variations of mortality were also high in Nepal (319%) (EAPC=2.33, 95% CI 2.04, 2.62) and Malaysia (289%) (EAPC=0.86, 95% CI 0.46, 1.26). In contrast, ASMRs greatly declined in Japan (EAPC=-2.31, 95% CI -2.89, -1.73) in 1990-2021 (Figure S3-S4). Worryingly, Nepal still had the highest percentage variation of DALYs across Asia (228%) (EAPC=2.04, 95% CI 1.74, 2.34) (Figure S5-S6). (A) EAPC analysis of the LivCa ASIRs from 1990-2021. EAPC: Estimated annual percentage change; (B) changes in incidence cases of LivCa from 1990-2021; (C) the ASIR trends in males and females of LivCa from 1990-2021; (D) the ASIR trends in males and females of hepatoblastoma and primary LivCa caused by five etiologies from 1990-2021
3.1.3. Variations by Age and Sex
ASIRs, ASMRs, and ASDRs were higher in males than in females for overall LivCa and for LivCa of five etiologies and hepatoblastoma (Figure 2C and S7-S8). In both males and females, ASIRs, ASMRs, and ASDRs of LivCa, except LivCa caused by NASH and alcohol use, all decreased over time. Interestingly, females had lower ASIRs, ASMRs, and ASDRs of LivCa caused by HBV and alcohol use than males, and HBV and alcohol use were also responsible for the highest ASIRs of LivCa in males. However, the proportion of the two etiologies displayed slight decreases with fluctuation in males in 1995-2005. For females, HCV accounted for the higher incidence, mortality, and DALYs, and its proportion rose sharply in 1990-1995 and then gradually declined. In addition, the burden of LivCa caused by NASH was comparable in terms of trends and counts between males and females, showing a significant upward trend (Figure 2D and S9-S10).
We also explored the age distribution of the LivCa burden. As shown in the pyramid diagrams (Figure 3A and B), the burden of hepatoblastoma was mainly borne by children <5 years old due to its nature, and the overall incidence of LivCa and the incidence of primary LivCa of different etiologies were higher in the population aged 85-89 and 90-94 years, respectively. The incidence rose with age in the population aged below 85 years but declined in the population aged above 95 years. Males generally had a higher or the same incidence of LivCa than females of the same age, especially LivCa caused by alcohol use and HBV. Mortality and DALYs are detailed in Figure S11-S14. (A) The number of incidence cases grouped by age and sex of LivCa; (B) the number of incidence cases grouped by age and sex of hepatoblastoma and primary LivCa caused by five different etiologies; (C) Asian distribution of SDI and LivCa ASIRs in different countries. SDI: Sociodemographic index; (D) Asian distribution of SDI and LivCa ASIRs from 1990-2021 in different regions. SDI: Sociodemographic index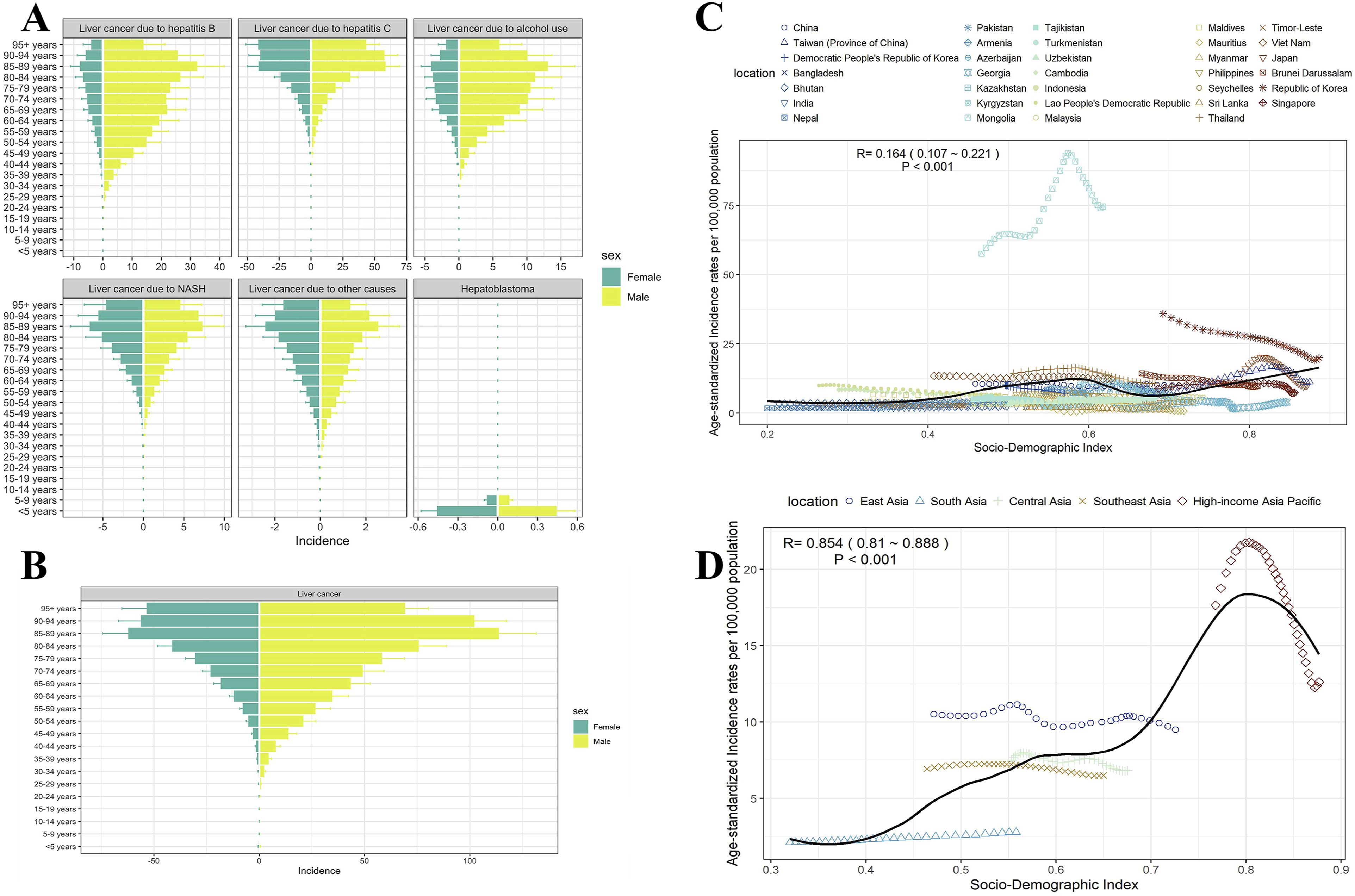
3.1.4. Association of LivCa Burden With SDI
In Asian countries, SDI had significant but weak correlations with ASIRs (r=0.164, 95% CI 0.107-0.221, P<0.001), ASMRs (r=0.114, 95% CI 0.055-0.171, P<0.001), and ASDRs (r=0.095, 95% CI 0.037-0.153, P<0.001) of LivCa. In other words, higher levels of economic development may be associated with higher incidence, mortality, and DALYs of LivCa (Figure 3C and S15-S16). Meanwhile, the low r values indicate that while a positive association exists, the level of socioeconomic development accounts for only a small proportion of the variance in LivCa rates. Korea, Taiwan (Province of China), Japan, and Singapore (all SDI>0.7) had far higher incidence, mortality, and DALYs than low-SDI countries, especially incidence. The higher level of regional medical levels could be a potential explanation for this phenomenon. Notably, Mongolia had far higher ASIRs, ASMRs, and ASDRs of LivCa than expected despite a lower SDI (0.5). In addition, we analyzed the association in different regions of Asia and found that the burden of LivCa was higher than expected in East Asia, slightly lower than expected in South, Southeast, and Central Asia, and increased at first and then decreased in high-income regions (Figure 3D and S17-S18).
3.2. Risk Factors
As revealed in Figure 4, the proportion of DALYs attributable to risk factors was the highest in Central Asia (61.39%), which was closely related to behavioral and metabolic factors. Central Asia also held the highest proportion of DALYs attributable to alcohol use (24.42%) and drug use (24.83%), and high BMI (14.65%) was also a major risk factor. Smoking was an important risk factor for the proportion of DALYs, especially in East Asia (12.34%) and Southeast Asia (13.23%). High fasting glucose was a less significant risk factor, and it accounted for the highest proportion of DALYs in South Asia (3.5%). Proportion of LivCa DALYs attributable to risk factors for six regions of Asia. DALY: Disability-adjusted life year
3.3. Projections to 2040
Using the BAPC model, we predicted the future trends of LivCa burden in Asia in 2022-2040. Overall, from the perspectives of incidence, ASIRs, mortality, ASMRs, DALYs, and ASDRs, the LivCa burden was predicted to greatly decrease across Asia and in 34 Asian countries in 2022-2040 (Figure 5A and B and S19-S22). By 2040, incidence, ASIRs, mortality, ASMRs, DALYs, and ASDRs would decrease to 252,723, 5.51%, 223,426, 4.87%, 5,789,622, and 126.28%, respectively (Table 3). (A) The prediction changes trends of LivCa age-standardized incidence cases number from 1990-2040 in Asia; (B) the prediction change trends of LivCa ASIRs from 1990-2040 in Asia Prediction of LivCa Burden in Asia From 2022 to 2024

4. Discussion
4.1. Interpretation of Key Findings
Using the data from the GBD 2021, this study systematically and innovatively assessed the burden of etiology-specific LivCa across Asia and in different Asian countries in 1990-2021, as well as the projections to 2040. LivCa included primary LivCa of five etiologies and hepatoblastoma. The disease burden was quantified using incidence, mortality, DALYs, and ASRs, and EAPC and percentage variation were calculated. Finally, we predicted the future trends of LivCa burden up to 2040 using the BAPC model. The results revealed that: 1) The overall LivCa burden in Asia displayed a significant decreasing trend in 1990-2021, with HBV being the first cause of LivCa, followed by HCV. The burden of primary LivCa caused by HBV and hepatoblastoma declined, while that caused by NASH and alcohol use rose. 2) The proportion of LivCa of different etiologies and attributable to different risk factors greatly varied across Asia. 3) Obvious sex differences were found in the burden of LivCa and major etiologies. Males had a higher overall incidence of LivCa than females, and HBV and alcohol use were the main contributors, while HCV was predominant in females. 4) The overall incidence of LivCa was the highest in the population aged 85-94 years. 5) A significant positive correlation was present between SDI and the burden of LivCa. 6) The burden of LivCa in Asia was predicted to decline in 2022-2040.
4.2. Shifts in Major Etiologies, Regional Disparities and Risk Factors
The burden of LivCa of different etiologies has been extensively assessed. The Global Burden of LivCa 1990-2015 revealed that the incidence of LivCa due to HBV decreased by 35% over the last 25 years, and it also greatly declined (25%) in cases of other etiologies, with the increase due to population growth excluded; both incidence and mortality of LivCa were higher in middle, middle-high, and high SDI. 32 NASH-associated liver cancer (NALC) showed a significantly increasing burden of mortality globally in 2010-2019, with the highest burden in sub-Saharan Africa and Southeast Asia. Certain sex differences were observed: The incidence of NALC declined in females but remained stable in males. 33 By 2024, the incidence and mortality of LivCa are expected to sharply decline in China but rise in the United States. 34 Another report on LivCa caused by alcohol use in 1990-2021 stated that males and middle-aged and aged people are at high risk for LivCa due to alcohol use, with great increases in mortality and ASRs. 35 As demonstrated by the Global Burden of LivCa 2019, the ASR for DALYs peaked at the age of 75-79, consistent with the trend in Asia. 36
The WHO global health sector strategy on viral hepatitis, endorsed by the 69th World Health Assembly in 2016, aims to reduce new cases of HBV and HCV by 90% and deaths by 65%.5,37 In 2023, the WHO estimated that HBV or HCV infections affected approximately over 350 million people worldwide, and adequate testing and prevention are still lacking among most patients (https://www.who.int/health-topics/hepatitis/elimination-of-hepatitis-by-2030). The policies against HBV and HCV (two major causes of LivCa) have undoubtedly contributed to the prevention and control of LivCa globally. China possesses the highest burden of LivCa, with endemic HBV infections being the major cause. The Chinese government has adopted routine HBV vaccination of infants since 1992, and carried out the comprehensive vaccination policy in backward areas since 2005, dramatically increasing the vaccine coverage. The burden of LivCa further declines with increasing popularization of advanced imaging and molecular diagnostic equipment in large medical centers, and advancements in systemic therapies such as excision and ablation, and immunotherapy. Randomized controlled trials and data indicate that early HBV screening and vaccination have effectively reduced HBV prevalence and spread in China, and prevented primary LivCa and fulminant hepatitis in infants, dramatically easing the public health burden associated with LivCa. 38 HCV infections may be linked to human immunodeficiency virus co-infection and genetic factors. The incidence of HCV was the highest in Taiwan (Province of China); despite high national health insurance coverage, extensive vaccination, and advanced medical levels during the late 20th century, Taiwan (Province of China) had a significantly higher HCV incidence in patients with HIV co-infection due to limitations of economic diversity, resources, regional culture, and behavioral habits. The Chinese mainland harbors a higher incidence of HCV, and even half of the population aged above 40 is infected with HCV in a small-scale survey, which may be attributed to the lack of reasonable methods of medical sterilization due to poor sanitary conditions in some regions of China before 1990, as well as socioeconomic inequality, large regional development gaps, and heterogeneous implementation of prevention programs at that time in China. 39 In recent decades, the incidence of HCV-related LivCa has shown no increase, possibly because of the introduction of highly potent antiviral drugs for HCV in 2014 and the development of medical technology, restricting further HCV progression and prevalence. 40
We observed an overall declining trend in the LivCa burden in Asia, but the increasing impact of NALC cannot be underestimated. East Asia ranked first in the new NALC cases globally in 1990-2021, in contrast to the decline in HBV and HCV. In the high-income Asia-Pacific region, however, negative growth was seen in the burden of NALC incidence and mortality, the latter of which could be mostly attributed to population aging. 33 This suggests that in developed regions (e.g., Japan and South Korea), NALC prevention and control have achieved the desired effect, and NALC mortality simultaneously decreases with the increase in life expectancy resulting from improvements in healthcare and hygiene levels. China, with a high proportion of the population and not classified as a high-income Asia-Pacific country, may be the primary contributor to the current increase in the NALC burden in East Asia. The possible reason is that in the developed regions of China, the dietary structure gradually shifts from a vegetable diet to an animal-based diet, but the health awareness of controlling fat and carbohydrate intake in the high-income Asia-Pacific region is lacking, thus greatly raising the risk of obesity and metabolic problems.41-43 In China, the number of NALC cases and overweight and obese people is the largest, and the burden of NALC is predicted to constantly rise in East Asia as obesity and insulin resistance become more common. It was predicted that the overall burden of LivCa declined in East Asia, possibly suggesting a continued reduction in the NALC burden in other East Asian countries and regions, or that China can continue to effectively combat viral hepatitis. However, this undoubtedly signifies that China and other NALC-increasing regions in Asia need to raise their vigilance and strengthen their efforts to control NASH.44,45 Previous studies on NASH in Asia also revealed that the ASR for incidence of NALC in Mongolia was higher in 2021, which was possibly attributed to the high-fat diet. Meat and dairy products may have contributed to the development and progression of NALC in Mongolia. In China, India, and the United States, which recorded the largest number of new NALC cases and deaths in 2021, heavy metal pollution from large-scale industrial and agricultural activities is also a significant risk factor, besides large populations and lifestyle. 46 Meanwhile, the peak of increase in ASIRs for alcohol use-related LivCa has been observed in Southeast Asia. Due to an urgent demand for alcohol with social development, rising purchasing power, and lack of governmental control in Southeast Asia, combined with the local dietary habits and lack of early screening, hard-to-detect alcoholic hepatitis has become the culprit in the growing burden of LivCa. 47 Additionally, in low-SDI countries, such as Thailand and Mongolia, alcohol-related LivCa exhibits a high ASR for incidence, and both the total number of cases and mortality increased in younger populations in 2000-2021. This is attributed to a certain delay in the onset and mortality of alcohol-related LivCa, longer time required for diagnosis, or later-stage detection, which is closely linked to the backward medical prevention and control measures. 47 Inspired by NASH- and alcohol use-related cases, policymakers should develop sound public health policies and safety education, achieve early detection of associated LivCa and perform preventive controls and clinical interventions, and guide rational dietary control and alcohol use, thereby reducing the possible burden of NALC and alcohol use-related LivCa. In the high-income Asia-Pacific regions with abundant medical resources, the survival rate of preterm and very-low-birth-weight infants rises, increasing hepatoblastoma-susceptible population and worsening incidence and DALYs, but on the positive side, the burden of hepatoblastoma in children declines, presenting the efforts made by the government to address this health issue. 48
Besides direct etiologies, different risk factors were also important contributors to variations in the burden of LivCa. Drug injection, as an effective route of transmission of HBV or HCV causing cirrhosis and LivCa deaths, was a major risk factor for LivCa in less developed regions of Central Asia (e.g., Mongolia, Kazakhstan, Afghanistan, and Uzbekistan). The possible reason is closely related to drug abuse and illicit trafficking, wars, and low political and economic conditions. 49 Research also suggests that due to the widespread habit of chewing betel nut in some Asian countries, the combination of adverse factors may synergize to significantly increase the incidence and mortality of LivCa and digestive tract cancers, in addition to oral cancer, in specific populations, such as male smokers. 50 In addition, metabolic factors (e.g., obesity and high BMI) also led to an increasing burden of LivCa in Central Asia, possibly related to alcohol use and high-fat diets shaped by climate and customs. 49
Furthermore, the correlation of some risk factors and their combined underlying effects on disease warrant our attention. Liver diseases such as HBV and HCV are major contributors to LivCa. The synergistic relation of drinking and hepatitis development and progression has been demonstrated in numerous studies. For example, the HERO study revealed high HCV infection rates in heroin injectors, and drinking is closely linked to higher infection rates and accelerated HCV progression, whereas less alcohol significantly achieves an antiviral effect. 51 Another study showed that obesity (high BMI) with diabetes increases the risk of cirrhosis and HCC. Immunosenescence and cellular energy depletion exacerbate the inflammatory and carcinogenic effects of obesity with age, and patients with high BMI often consume excessive alcohol. 52 As a result, these factors jointly contribute to the progression of liver disease toward LivCa.
Overall, the significant increase in the LivCa ASIR in Taiwan, Nepal, and India in the past few decades is undoubtedly worth attention. Taiwan is one of the global models for LivCa prevention and control, and the first region to implement universal HBV vaccination. However, the ASIR of LivCa anomalously rose in Taiwan. We speculated that the coverage of free HBV, HCV, and LivCa screening was significantly expanded in Taiwan in 1990-2021, leading to an increase in detected cases rather than a natural increase. The possible reason was also related to regional heterogeneity due to a small sample size in Taiwan. Besides, the challenges faced by Nepal in LivCa prevention and control are an inadequate cancer registration system and a lack of extensive screening resulting from low economic and medical levels. The elevation of ASIR in LivCa is closely linked to the absence of preventive means and high BMI resulting from unhealthy dietary habits. Additionally, India experienced unsatisfactory policy implementation effects and poor socioeconomic conditions. The viral hepatitis and LivCa prevention and control program was launched in India as early as the late 20th century. However, its coverage was limited, and the screening rate remained low due to inefficient workflows, a fragile cold chain system, and a shortage of healthcare providers. Moreover, India has a large population, severely inadequate health insurance coverage, significant economic disparities across regions and populations, and low health literacy and disease cognition, thus further worsening the LivCa burden.53-57
4.3. The Role of Sex, Age, and SDI
Sex induced variations in the burden of LivCa of different etiologies in Asia, consistent with the global situation. The reasons are as follows: The proportions of smokers and drinkers are higher in males, producing a higher incidence of LivCa; the distribution and accumulation of body fat, as indicated by BMI, are closely associated with the development of LivCa, and middle-aged and aged males are at high risk for obesity, hyperglycemia, and high BMI. 58 In addition, chronic HBV is the first cause of LivCa in males, whereas HCV, as the primary cause in females, can be radically cured by antiviral medications, expanding the sex difference in LivCa. 59
An impressive correlation was present between socioeconomic status (SDI) and LivCa burden. Due to low fertility, high educational levels, and higher per capita income, high-SDI regions differ from middle- and low-SDI regions in economic conditions, medical levels, living environments, consciousness, and living habits. For example, the burden of LivCa caused by viral hepatitis persistently decreases in high-SDI regions with high vaccination coverage and medical levels, and air contamination may be a potential risk factor for LivCa in industrialized areas.60,61 Meanwhile, due to more advanced LivCa detection means and early diagnosis techniques, high-SDI regions may also have higher LivCa incidence than low-SDI regions with insufficient disease screening. 52 Research suggests that HCV is prevalent in some of the high-SDI regions, while the burden of HBV is high mostly in middle-low-SDI regions. Such regional variations reveal the heterogeneity of risk factors worldwide. 62 In addition, risk factors in high-SDI regions also contribute greatly to LivCa, e.g., alcohol use contributed to 35% of LivCa in 2019 in Europe and Australia. 62 Faced with this phenomenon, local government agencies or CDCs should be motivated to develop corresponding policies. In low-SDI regions, the overall survival rate of LivCa patients may be lower due to competitive risks such as infectious diseases and trauma rather than chronic diseases (e.g., HBV, HCV). Moreover, these regions face higher risks of exposure to aflatoxins, potentially attributed to poor grain storage facilities and dietary habits. 63
As mentioned above, a positive correlation was present between SDI and LivCa burden, but no absolute causality was observed; SDI only accounted partially for high LivCa burden. This may be attributed to higher diagnosis and screening rates in high-SDI regions, and the influence of regional factors (e.g., population, race, genetics, and culture), as well as regional disease prevalence and environmental pollution. Given the limitations posed by geographical variations in Asia and the scarcity of cases contradicting this correlation, whether genetic or environmental factors are the most significant contributors cannot be determined. From the perspective of the commonalities in low-SDI regions, however, this should probably be attributed to non-proactive preventive screening and insufficient medical levels and budget.
4.4. Limitations
Some limitations are worth noting. First, the GBD 2021 only contains the data on the global disease burden in 2021 and before, resulting in a certain lag and a lack of real-time data on the current burden. The GBD relies on available diagnostic and reporting data, which may neglect undiagnosed or unscreened LivCa cases and inadequately reflect the influence of early screening on incidence and disease burden.
Second, the reliability of incomplete or missing data in the GBD is based largely on predictive analyses by modeling methods, and the healthcare data in some less developed or developing countries may be affected by misdiagnosis, underreporting, overreporting, or even misreporting, thus restricting data completeness, accuracy, and comparability.
Third, this study was also limited by data and model assumptions. GBD integrates multi-source data by statistical algorithms to fill gaps, but the inherent model assumptions (such as the constant relationship of risk factors with disease burden across regions) may not align with real-world differences in screening strategies, healthcare accessibility, and prevention practices across countries. This may lead to biased estimates of disease burden in some regions. Additionally, the BAPC model has inherent limitations. It extrapolates based on historical trends, and assumes that age, period, and cohort effects remain unchanged in the future. As a result, it cannot incorporate potential major medical breakthroughs, policy interventions, or dramatic environmental changes that may occur during the prediction period. Meanwhile, uncertainties in the input data are amplified during the prediction process. Finally, GBD etiology attribution is uncertain for multi-etiology cases and does not reflect heterogeneity in etiology. Macroscopic results at the national level may obscure significant variations in domestic subpopulations, and the direct applicability of study findings to policy-making is restricted due to delays in data release and analysis.
5. Conclusion
The burden of etiology-specific LivCa and hepatoblastoma declined greatly in Asia in 1990-2021. The burden of different types of LivCa varies in trends, with downward trends in the burden of LivCa caused by HBV and HCV, and hepatoblastoma, increases in incidence and mortality, and a less significant increase in DALYs in the burden caused by NASH, and stable changes in the burden caused by alcohol use. The proportion of LivCa of different etiologies and attributable to different risk factors shows regional disparities across Asia. Obvious sex differences are also present in the burden of LivCa (higher in males), and SDI has a significant positive correlation with the LivCa burden. The highest incidence is found in the population aged 85-94 years. The burden of LivCa is predicted to decline up to 2040. Efforts have been made to reduce the burden of LivCa across Asian countries, but considering the influence of etiologic, regional, and demographic disparities, a comprehensive program (to raise awareness, strengthen early assessment and screening for LivCa, promote population-wide vaccination coverage, develop targeted clinical treatments, and introduce preventive and regulatory policies, e.g., nationwide HBV and HCV vaccination programs, specific free screening policies, and community health education) is required to handle this public health issue. Meanwhile, more healthcare funds and resources should be invested to minimize the burden of LivCa in Asia in the future.
Supplemental Material
Supplemental Material - Asian Burden of Liver Cancer 1990-2021 and Predictions to 2040: An Analysis of the Global Burden of Disease Study 2021
Supplemental Material for Asian Burden of Liver Cancer 1990-2021 and Predictions to 2040: An Analysis of the Global Burden of Disease Study 2021 by Liandong Chen, Weibo Zheng, Haojie Ying, Xinyue Chen, Han Yan, Binzhe Zhou, Yuyuan Sun, Qihui Shao, Hanyu Xu, Bowen Jin, Haonan Jin and Bin Fu in Cancer Control.
Footnotes
Ethical Considerations
All original datasets were generated in compliance with the ethical standards of the institutions involved and adhered to the principles outlined in the Declaration of Helsinki. As such, Institutional Review Board (IRB) approval and Institutional Animal Care and Use Committee (IACUC) approval were not required for this study.
Author Contributions
All authors contributed to the study conception and design.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was funded by Youth Fund Project of Humanities and Social Sciences Research of Ministry of Education in 2024 (No. 24YJCZH448), The Second Batch of Provincial-Level Teaching Reform Project for Postgraduates in Zhejiang Province During the 14th Five-Year Plan Period (No. JGCG2024254), and Traditional Chinese Medicine Science and Technology Plan of Zhejiang Province (No. 2026ZF42).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.