
Abstract
Introduction
Cancer among the oldest-old (aged ≥85) is an escalating public health concern, particularly in the Middle East and North Africa (MENA), where demographic aging is advancing rapidly.
Methods
We analyzed cancer incidence and mortality trends among the oldest-old in MENA from 1990 to 2021 using Global Burden of Disease (GBD) 2021 data, and compared these trends to global patterns.
Results
Cancer incidence and mortality among the oldest-old in MENA increased substantially, surpassing global trends. Between 1990 and 2021, incidence rose by 54.2% in MENA vs 25.3% globally, while mortality increased by 17.6% vs 3.1% globally. Females experienced steeper rises in both incidence and mortality. Annual percent change (APC) in MENA incidence was +1.96 (95% CI: 1.28-2.64) for females and +0.83 (95% CI: 0.59-1.08) for males, compared to +0.28 (95% CI: 0.18, 0.38) and +0.47 (95% CI: 0.40, 0.55) globally. APC for mortality in MENA was +1.27 (95% CI: 0.66-1.88) for females and +0.33 (95% CI: 0.12-0.54) for males, vs −0.07 (95% CI: −0.13, 0.0) and +0.11 (95% CI: 0.03, 0.18) globally. Leading cancers were prostate, lung, and colorectal for males, and breast, colorectal, and lung for females, with variation across countries.
Conclusion
The rising cancer burden among the oldest-old in MENA underscores the urgent need for targeted interventions. Strengthening preventive measures, improving healthcare access, enhancing cancer registration, and implementing tailored screening and treatment strategies are critical. Policymakers must prioritize geriatric oncology and invest in healthcare infrastructure to ensure equitable, effective cancer care for the region’s aging population.
Plain Language Summary
Cancer among people aged 85 and older is becoming a growing public health issue, especially in the Middle East and North Africa (MENA) region, where the population is aging rapidly. This study examined how cancer rates and deaths have changed over time in MENA from 1990 to 2021 using data from the Global Burden of Disease (GBD) study and compared these trends to the rest of the world. The results show that cancer rates in MENA have increased more than the global average. Between 1990 and 2021, cancer cases among the oldest old in MENA grew by 54.2%, compared to a 25.3% increase worldwide. Cancer-related deaths also rose by 17.6% in MENA, while the global increase was only 3.1%. Women in MENA saw a greater rise in both cancer cases and deaths than men. Prostate, lung, and colorectal cancers were the most common in men, while breast, colorectal, and lung cancers were the most frequent in women. The trends varied by country within the region. These findings show an urgent need for better cancer prevention, early detection, and treatment for older adults in MENA. Improving healthcare access, strengthening cancer tracking systems, and developing specialized care for older cancer patients should be key priorities. Policymakers must take action to ensure that aging populations receive the necessary cancer care and support.
Introduction
The Middle East and North Africa (MENA) region is experiencing a significant demographic shift marked by rapid population aging. From 1990 to 2023, the total population nearly doubled, and life expectancy at birth rose from 64.4 to 74.7 years.1,2 As healthcare and socioeconomic conditions improve, the proportion of individuals aged 85 and above has steadily increased, particularly among women, who outlive men. 3 With declining fertility rates and increased longevity,4-6 age-related diseases such as cancer are becoming more prominent on the region’s public health agenda.
This demographic shift mirrors a global trend driven by similar underlying factors.7,8 Over the past seven decades, five out of the seven Global Burden of Disease (GBD) super-regions—broad global groupings based on geographic, epidemiologic, and socioeconomic similarities—have experienced continuous improvements in life expectancy at birth, with the MENA region being one of them. 8 Globally, life expectancy rose from 65.1 years in 1990 to 73.3 in 2023, 2 with women consistently living longer than men.4,5 While these trends highlight global aging, the MENA region’s unique cultural, socioeconomic, and healthcare dynamics call for region-specific data, particularly on the oldest-old, whose cancer burden remains underexplored.9-12
Cancer risk increases with age due to cumulative exposure to carcinogens, declining immune function, and genomic instability.13-15 Among older adults, the “oldest old” (aged ≥85 years) represent a rapidly expanding subgroup that differs substantially from the “younger old” (aged 65-84 years). They experience higher rates of multimorbidity, frailty, disability, cognitive impairment, and polypharmacy, which diminish physiological resilience and functional reserve, often resulting in social dependency and the need for more complex, continuous healthcare support.10-12,16,17 These factors complicate cancer diagnosis, treatment decisions, and outcomes, underscoring the need for tailored geriatric and public health strategies to address their specific vulnerabilities.10-12,16,17 Older adults are also underrepresented in clinical trials and often receive either overtreatment or undertreatment, driven by ageism and assumptions about limited benefit. 18 In the United States, individuals aged 85 and older account for 8% of new cancer diagnoses. 15 A National Cancer Institute–led webinar, in collaboration with the National Institute on Aging, emphasized the need for clinical trials tailored to older adults with comorbidities—trials that account for how comorbidities affect cancer development and treatment response in the oldest old. 10
Despite global advances, most published studies on cancer epidemiology in the oldest adults focus on Europe and the United States, leaving cancer patterns among the oldest-old in other regions, such as the MENA, largely unknown. 19 Most studies focus on broader elderly populations or specific cancers, overlooking those aged 85 and above. This study addresses this gap by analyzing the epidemiology and temporal trends of cancer in the oldest-old population in the MENA region using the latest GBD 2021 data. By leveraging the GBD 2021 dataset, our study provides an unprecedented, comprehensive assessment of cancer incidence and mortality patterns in this understudied demographic. The use of GBD 2021 data allows for standardized, comparable estimates across countries and time, offering unique insights into regional disparities and informing context-specific strategies to improve geriatric cancer care in MENA.
Findings aim to support the development of evidence-based, age-sensitive cancer care policies tailored to the MENA context and to contribute to global efforts in equitable geriatric oncology.
Materials & Methods
Background on the MENA Region and SDI Stratification Based on the GBD 2021
The MENA region includes countries spanning two geographically and economically distinct areas: the Middle East (such as Lebanon, Jordan, Iraq, Saudi Arabia, and the Gulf Cooperation Council [GCC] countries) and North Africa (including Egypt, Libya, Tunisia, Algeria, Morocco, and Sudan). This region is characterized by substantial diversity in Socio-Demographic Index (SDI) levels, which reflect a population’s average achievements in income, education, and fertility, based on the GBD 2021 data.20,21 MENA countries range from low SDI (Afghanistan, Yemen) and low-middle SDI (Egypt, Morocco, Sudan) to middle SDI (Algeria, Iran, Iraq, Oman, Syria, Tunisia), high-middle SDI (Bahrain, Jordan, Lebanon, Libya, Palestine, Turkey), and high SDI (Kuwait, Qatar, Saudi Arabia, United Arab Emirates). This heterogeneity in development and healthcare infrastructure significantly affects disease patterns, healthcare access, and health outcomes across the region, particularly among older adults.
Data Extraction
We utilized data from the Global Burden of Disease (GBD) 2021 database, which offers comprehensive estimates on cancer and other diseases. All primary cancers/neoplasms were classified according to the International Classification of Diseases, 10th Revision (ICD-10 codes C00–D49). The GBD initiative involves over 3600 researchers from nearly 200 countries and integrates data from various sources, including scientific literature, household surveys, national censuses, vital registration systems, and cancer registries such as Cancer Incidence in Five Continents (CI5), the Nordic Cancer Registries, and the European Network of Cancer Registries. 20
For this study, we used the GBD Results Tool (https://vizhub.healthdata.org/gbd-results/) to extract age-standardized incidence rates (ASIR) and age-standardized mortality rates (ASMR) for cancer globally, across the MENA region, and for individual MENA countries from 1990 to 2021. 21 We also retrieved age-specific incidence and mortality rates for individuals aged 85 years and older across the same regions and time period. Non-melanoma skin cancers (NMSC) were excluded from the analysis. All GBD estimates are reported with 95% uncertainty intervals (UIs), reflecting the range within which the true value likely lies. These are based on 1000 model iterations that account for variability in data inputs, transformations, and model choices, including the use of statistical frameworks such as the Cause of Death Ensemble Model (CODEm) for mortality and DisMod-MR, a Bayesian meta-regression model, for non-fatal outcomes. Wider UIs indicate greater uncertainty due to limited or conflicting data, while narrower UIs suggest more reliable estimates supported by robust and consistent data sources. 21
In the GBD tool, ASIR and ASMR are calculated as weighted averages of age-specific rates per 100 000 population, using the GBD standard population for weighting. Standardization enables valid comparisons across populations with different age structures. 22 Age-specific rates were calculated by dividing the number of new cases or deaths in a defined age and sex group by the mid-year population of that same group. 23
Trends Analyses
We used the Joinpoint Regression Program (version 5.1.0) to analyze trends in age-specific cancer incidence and mortality from 1990 to 2021. This software detects statistically significant changes in trends (joinpoints) and calculates the annual percent change (APC) for each segment, as well as the average annual percent change (AAPC) over the entire study period. Trend significance was assessed using a Monte Carlo permutation method, with a P-value threshold of less than 0.05. 24
Ethical Considerations
As this study is based on publicly available, de-identified secondary data, ethical approval was not required.
Hypothesis
We hypothesized that cancer trends among the oldest-old in the MENA region would parallel global patterns over the study period.
Results
Burden of Cancer in the Oldest-Old Population
Cancer Incidence
Age-Standardized (ASIR) and Age-Specific Cancer Incidence Rates and Trends in 2021
Globally, ASIR for total cancers (excluding NMSC) declined slightly but significantly from 207.8 in 1990 to 201.1 in 2021 (APC: −0.15; 95% CI: −0.20, −0.11), whereas in the MENA region, they increased from 112.9 to 146.1 (APC: 1.02; 95% CI: 0.89, 1.15).
The total cancer incidence rate (excluding NMSC) increases with age both globally and in the MENA region (Figure 1), peaking among individuals in their 80s, with the highest rates observed in those aged 85 and older. Total Cancers Incidence Rate Per 100,000 Population Per Age Group in 2021 (Excluding Non-Melanoma Skin Cancer)
Crude Numbers and Percentages of Cancer Incidence in the Oldest-old Population in 2021
Total Cancer Incidence Rates, Numbers and Percent (Excluding NMSC) in Males Aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2021 in the World, MENA Region and Countries

APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UAE, United Arab Emirates; UI, Uncertainty Intervals.
aIndicates that the APC is significantly different from Zero at the alpha = 0.05 level.
Total Cancer Incidence Rates, Numbers and Percent (Excluding NMSC) in Females aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2021 in the World, MENA Region and Countries

APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UAE, United Arab Emirates; UI, Uncertainty Intervals.
aIndicates that the APC is significantly different from Zero at the alpha = 0.05 level.
Age-Specific Cancer Incidence Rates and Trends in the Oldest-Old Population, 1990-2021
In the oldest-old population, global cancer incidence rates increased from 1659.7 in 1990 to 1893.1 in 2021 (+25.3%), while in the MENA region, rates rose from 831.2 to 1150.3 (+54.2%).
The increase in cancer incidence rates in the oldest-old population in the MENA region was more significant for females (+48.1%) compared to males (+26.7%). In contrast, globally, the percent increase was +8.2% for females and +16.2% for males. In the MENA region, the APC values were +1.96 (95% CI: 1.28-2.64) for females and +0.83 (95% CI: 0.59-1.08) for males, compared to +0.28 (95% CI: 0.18-0.38) and +0.47 (95% CI: 0.40-0.55) globally (Tables 1 and 2). In 2021, the cancer incidence rate among the oldest-old population showed a male-to-female ratio of 1.8 globally, compared to a lower ratio of 1.5 in MENA—indicating that while men continue to have higher cancer rates than women in both settings, the gender gap in incidence rates is narrower in the MENA region.
Cancer Incidence Rates per Site in Males Aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2019 in the World and MENA Region
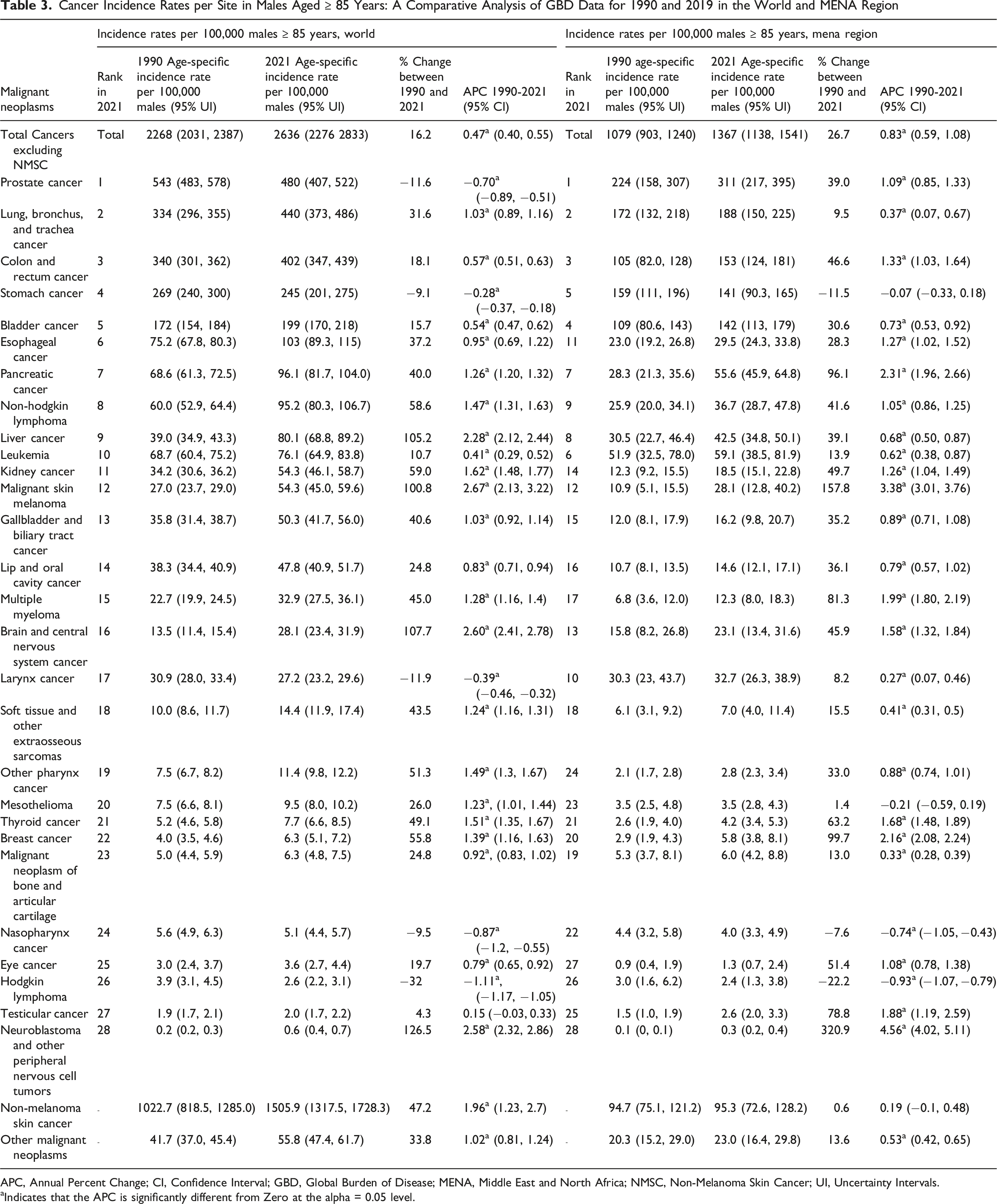
APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UI, Uncertainty Intervals.
aIndicates that the APC is significantly different from Zero at the alpha = 0.05 level.
Cancer Incidence Rates per Site in Females Aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2021 in the World and MENA Region
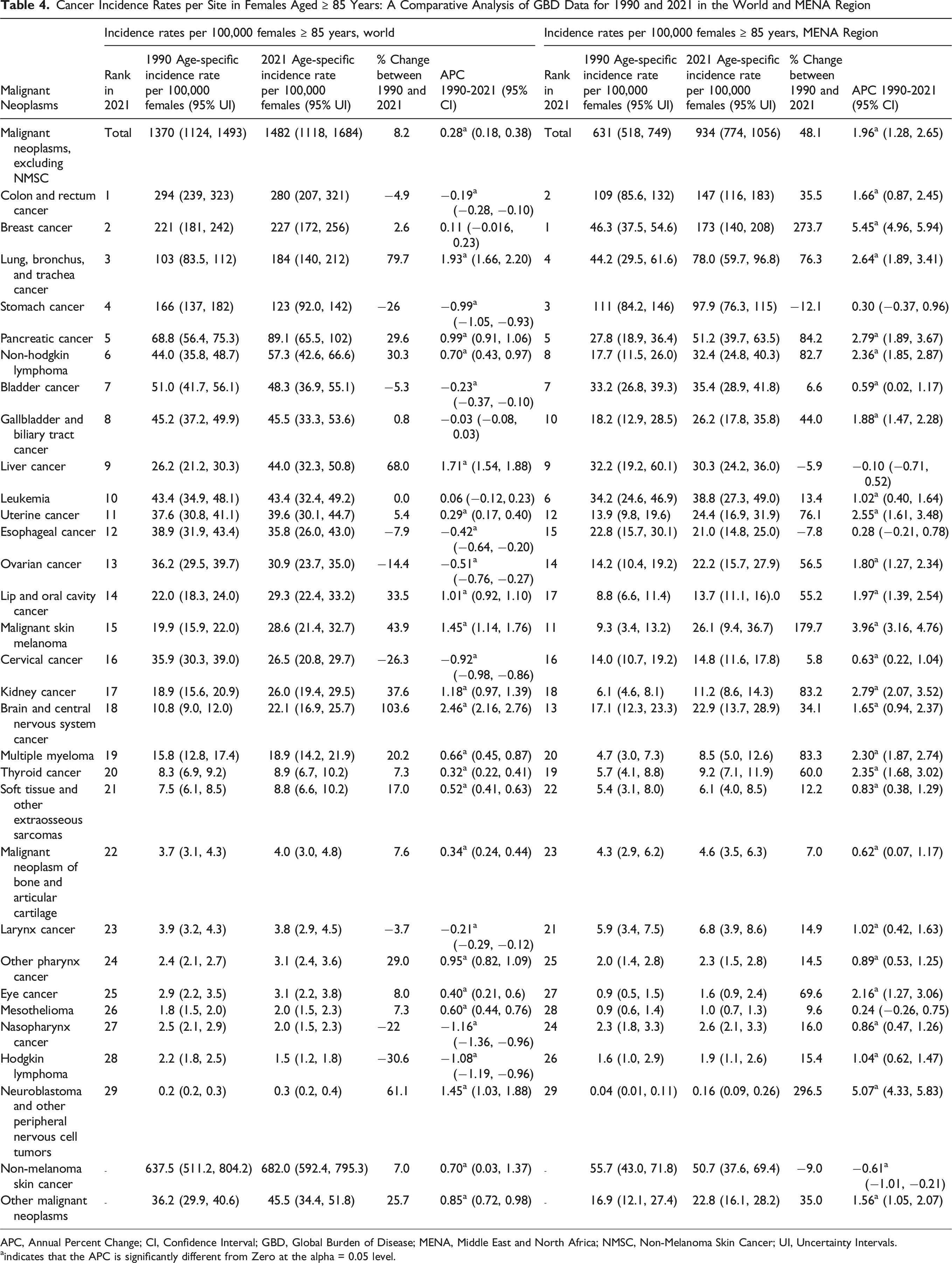
APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UI, Uncertainty Intervals.
aindicates that the APC is significantly different from Zero at the alpha = 0.05 level.
In 2021, cancer incidence rates per 100 000 among the oldest-old male populations in all MENA countries were lower than the global rate (2636) (Table 1). Bahrain (2587) had the highest rates, followed by Lebanon (2541), Qatar (2532), Palestine (2329), and Turkey (2100). Between 1990 and 2021, cancer incidence rates per 100 000 increased by 16.2% globally and by 26.7% in the MENA region (Table 1). Trend analyses of cancer incidence rates among the oldest-old male population from 1990 to 2021 revealed a significant positive APC globally (+0.47) and in the MENA region (+0.83). The highest APC values for cancer incidence trends among the oldest-old male population in the MENA region were in Oman (APC: +2.39), followed by Iraq (APC: +2.10), the UAE (APC: +2.08), Libya (APC: +1.78), and Kuwait (APC: +1.73). Tunisia and Bahrain had non-significant positive trends, while Turkey, Qatar, and Palestine had non-significant negative trends (Table 1).
In 2021, cancer incidence rates per 100 000 oldest-old female populations in the UAE (3694), Egypt (1703), Qatar (1514), and Bahrain (1504) were higher than the global rate (1482) (Table 2). All MENA countries recorded a higher percentage increase in cancer incidence rates than the global average between 1990 and 2021. The highest increases were estimated in the UAE, followed by Iraq and Egypt. With the exception of Qatar, all MENA countries showed significantly positive APC trends in cancer incidence among the oldest-old female population from 1990 to 2021. The highest APC values were in the UAE (APC: +8.11), followed by Egypt (APC: +4.23), Algeria (APC: +3.27), Iraq (APC: +2.48), and Libya (APC: +2.15) (Table 2).
Cancer Mortality
Age-Standardized (ASMR) and Age-Specific Cancer Mortality Rates and Trends in 2021
While cancer ASMR for total cancers (excluding NMSC) remained consistently higher globally (147.0 in 1990 and 115.1 in 2021) than in the MENA region (96.7 in 1990 and 89.6 in 2021), the decline in ASMR between 1990 and 2021 was smaller in the MENA region (APC: −0.11; 95% CI: −0.22, −0.005) compared to the global average (APC: −0.86; 95% CI: −0.90, −0.82).
The total cancer mortality rate (excluding NMSC) increases with age both globally and in the MENA region (Figure 2), peaking in men and women in their 80s, with the highest rates observed in those aged 85 and older. Total Cancers Mortality Rate Per 100,000 Population Per Age Group in 2021 (Excluding Non-Melanoma Skin Cancer)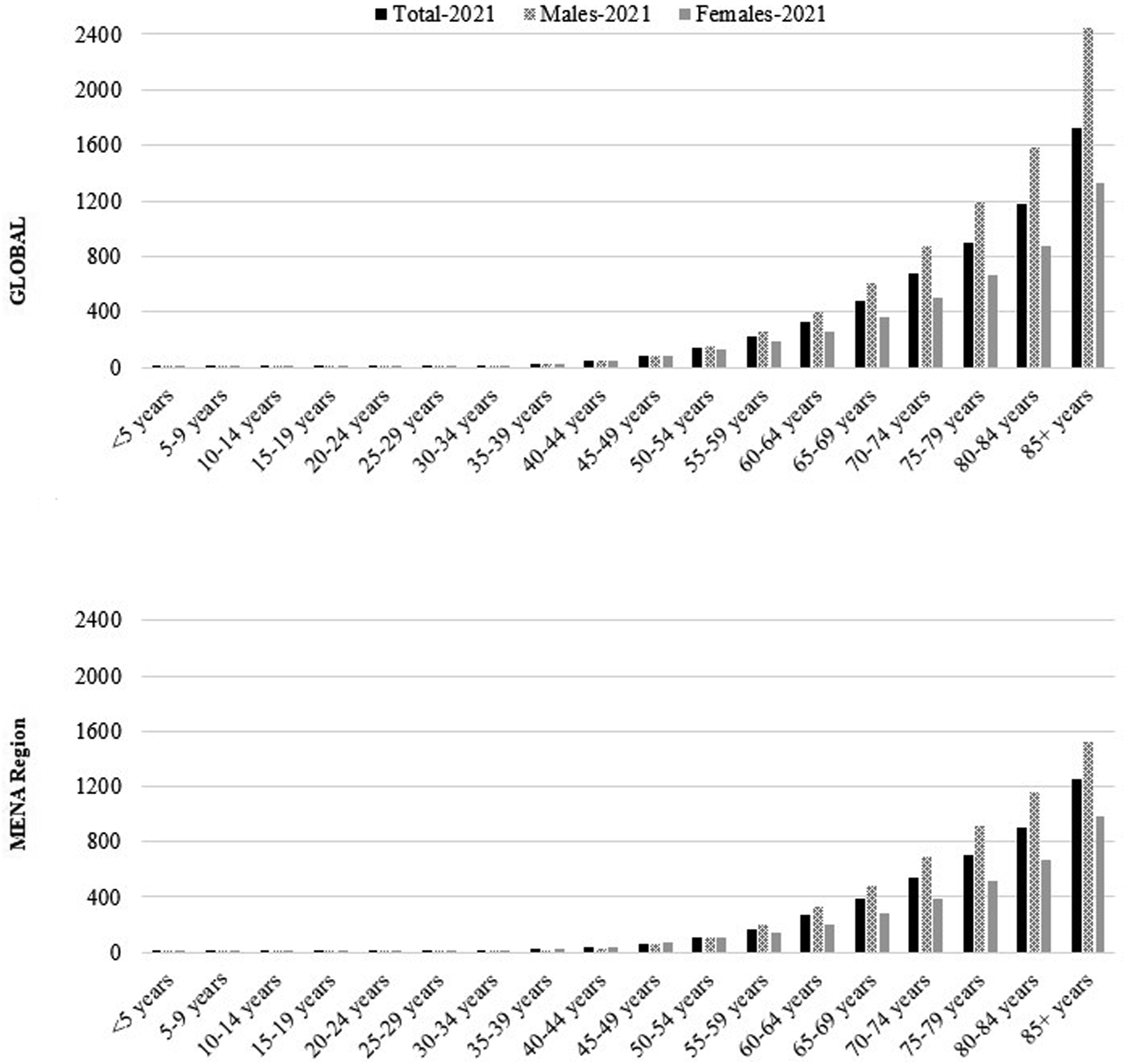
Crude Numbers and Percentages of Cancer Mortality in the Oldest-Old Population in 2021
Of all new cancer-related deaths in 2021, those occurring in the oldest age group (excluding NMSC) accounted for 12.2% globally (10.9% in males and 13.9% in females) and 7.3% in the MENA region (7.6% in males and 7.0% in females). This corresponds to approximately 1 191 538 deaths globally and 28 727 deaths in the MENA region in 2021.
Age-Specific Cancer Mortality Rates and Trends in the Oldest-Old Population, 1990-2021
Total Cancer Mortality Rates, Numbers and Percent (Excluding NMSC) in Males aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2021 in the World, MENA Region and Countries
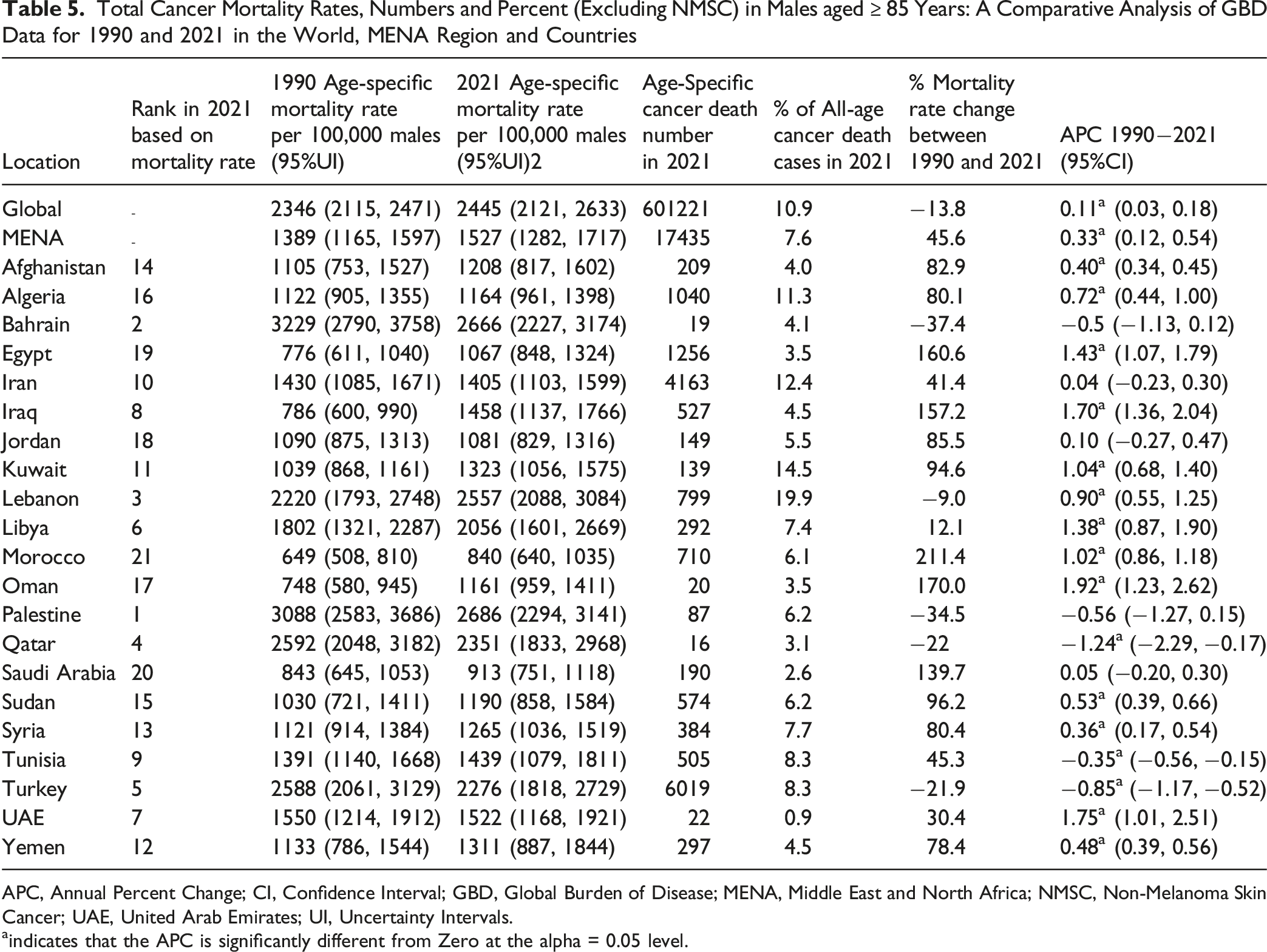
APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UAE, United Arab Emirates; UI, Uncertainty Intervals.
aindicates that the APC is significantly different from Zero at the alpha = 0.05 level.
Total Cancer Mortality Rates, Numbers and Percent (excluding NMSC) in Females Aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2021 in the World, MENA Region and Countries

APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UAE, United Arab Emirates; UI, Uncertainty Intervals.
aindicates that the APC is significantly different from Zero at the alpha = 0.05 level.
Cancer Mortality Rates per Site in Males aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2019 in the World and MENA Region
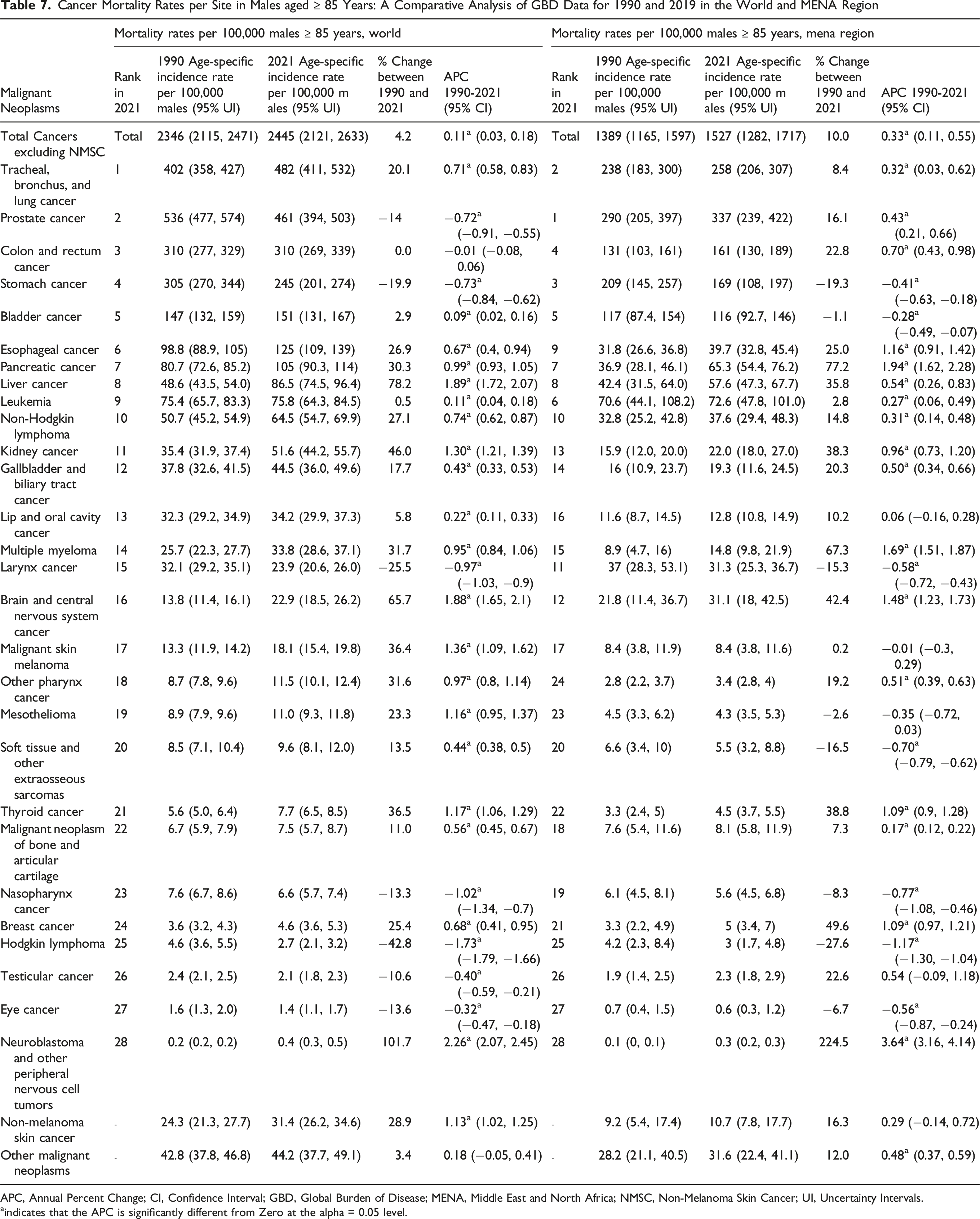
APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UI, Uncertainty Intervals.
indicates that the APC is significantly different from Zero at the alpha = 0.05 level.
Cancer Mortality Rates per Site in Females Aged ≥ 85 Years: A Comparative Analysis of GBD Data for 1990 and 2019 in the World and MENA Region
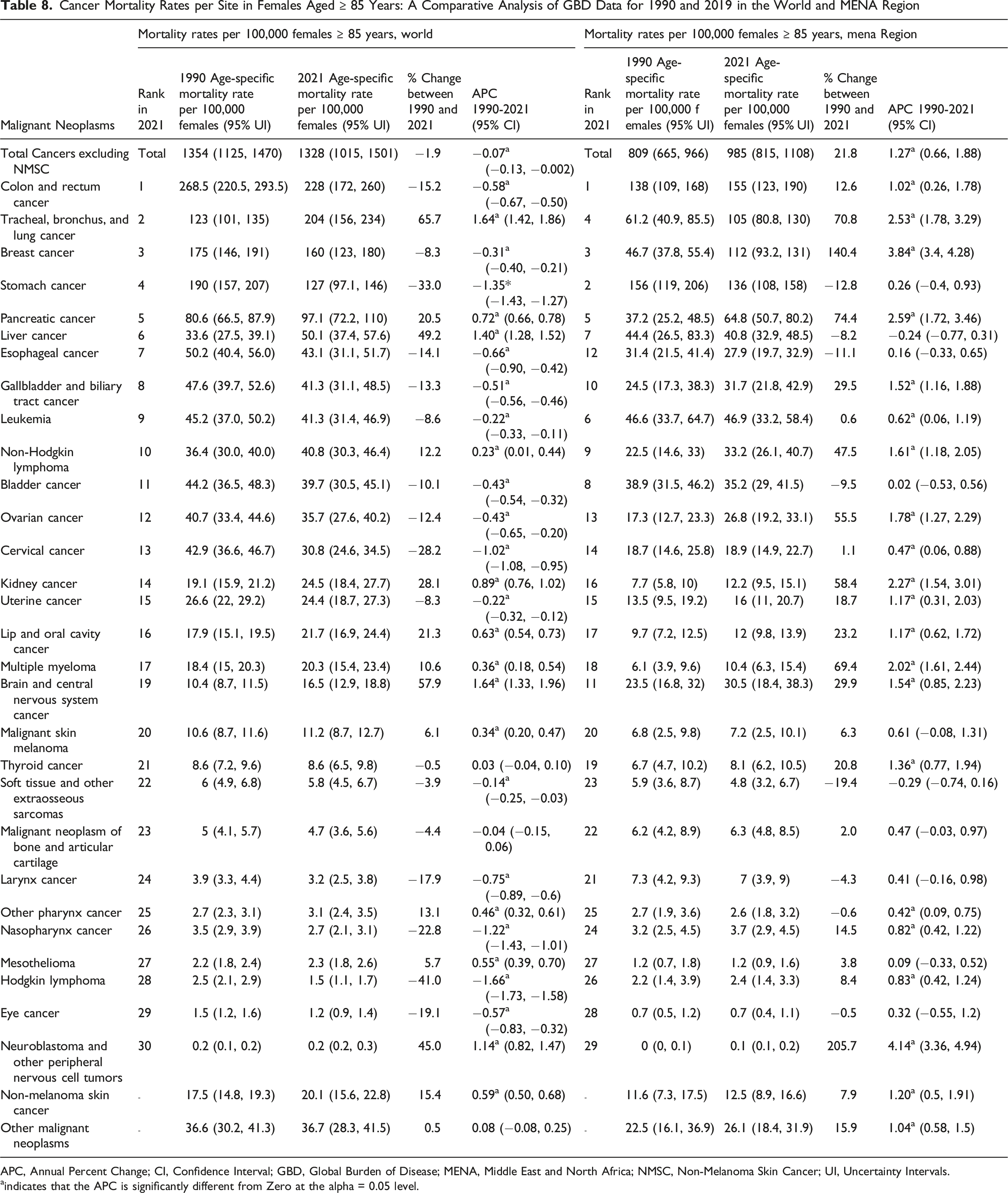
APC, Annual Percent Change; CI, Confidence Interval; GBD, Global Burden of Disease; MENA, Middle East and North Africa; NMSC, Non-Melanoma Skin Cancer; UI, Uncertainty Intervals.
aindicates that the APC is significantly different from Zero at the alpha = 0.05 level.
In 2021, the cancer mortality rates per 100 000 among the oldest-old male populations in Palestine (2686), Bahrain (2666), and Lebanon (2557) exceeded the global rate (2445). While the global rate declined by 13.8% between 1990 and 2021, the MENA region saw a sharp increase of 45.6% (Table 5). Trend analyses of cancer mortality rates among the oldest-old male population from 1990 to 2021 revealed a significant positive APC globally (+0.11) and in the MENA region (+0.33). Several MENA countries exhibited significant positive APCs, with the highest observed in Oman (+1.92), followed by the UAE (+1.75), Iraq (+1.70), Egypt (+1.43), and Kuwait (+1.04) (Table 6). Conversely, Qatar, Turkey, and Tunisia exhibited significant negative APCs (−1.24, −0.85, and −0.35, respectively), while Palestine and Bahrain showed non-significant negative APCs (Table 5).
In 2021, the cancer mortality rates per 100 000 oldest-old female populations were highest in the UAE (3701), Egypt (1880), and Bahrain (1365), surpassing the global rate (1328). While the global rate declined by 1.9% between 1990 and 2021, the MENA region saw a sharp increase of 21.8% (Table 6). Trend analyses of cancer mortality rates among the oldest-old female population from 1990 to 2021 showed a minimal but significant global negative APC (−0.07) in contrast to a significant positive APC in the MENA region (+1.27). In the MENA region, Qatar and Tunisia were the only countries with significant negative APCs (−1.17 and −0.14, respectively), while Iran and Kuwait had minimal non-significant negative APCs. The remaining MENA countries demonstrated significant positive APCs, with the exception of Turkey and Bahrain, which had non-significant positive changes. The highest APC was in the UAE (+7.48), followed by Egypt (+3.72), Algeria (+2.61), Iraq (+1.94), and Libya (+1.72) (Table 6).
Discussion
Cancer Burden Among the Oldest-Old in the MENA Region—Implications for Care, Policy, and Research
The cancer burden among the oldest-old (85+) in the MENA region poses urgent challenges for public health, healthcare delivery, and policy. While studies have documented a rising cancer burden across the region,25-27 few have specifically examined this vulnerable and rapidly growing demographic. Evidence from Western countries similarly underscores the growing cancer burden in this age group. 19 In MENA, cancer incidence and mortality among the oldest-old remain below global levels, but their rise—especially among women—has been steeper than worldwide trends. In 2021, the oldest-old accounted for 3.7% of new cancer cases in MENA compared to 7.6% globally and 8% in the United States. 15 Despite the smaller share, this sharp increase highlights how regional health systems remain underprepared for demographic aging, underscoring the need for inclusive research, tailored interventions, and age-responsive policies.
Demographic and Epidemiological Drivers
Population aging in the MENA region—driven by declining fertility rates and increasing life expectancy3-6—is a central driver of this trend. Cancer risk rises with age due to cumulative exposures and biological changes.13,28 As life expectancy increases, the cancer burden in the oldest-old will continue to grow, straining already limited healthcare systems.
Challenges in Geriatric Cancer Care in MENA
Geriatric oncology is complex worldwide, but the challenges are heightened in MENA. The oldest-old often face frailty, comorbidities, cognitive decline, and altered drug metabolism, complicating treatment decisions.13,17 Yet they remain underrepresented in clinical trials, leading to reliance on protocols designed for younger patients. Ageism and limited use of tools like the Comprehensive Geriatric Assessment (CGA) further compromise individualized care.18,29
In MENA, scarce region-specific data and trials30,31 drive inappropriate extrapolations that overlook biological, pharmacological, and sociocultural differences. Systemic barriers—such as limited access to geriatric oncology services, weak health infrastructure, and the absence of regionally adapted guidelines—further undermine care.9,32 The lack of universal health coverage in most MENA countries restricts timely diagnosis and treatment, 33 while sociocultural factors, especially for older women, delay help-seeking. Economic constraints, political instability, and reliance on overburdened family caregivers32,34-37 intensify these challenges. Addressing them requires investment in geriatric oncology, infrastructure, workforce training, and policies tailored to the oldest-old.
Gender-Specific Disparities in Cancer Patterns and Care in the MENA Region
Gender strongly shapes cancer patterns and outcomes in the oldest-old through biological, behavioral, and systemic factors. In the MENA region, women live longer and have experienced sharper increases in cancer incidence since 1990—particularly for breast, colorectal, and lung cancers—yet their overall cancer rates at 85+ remain lower than men’s. This disparity, consistent with global trends, reflects both biological differences and historical exposures: men carry higher burdens of lung, bladder, and prostate cancers due to tobacco, occupational, and alcohol risks,38-40 while breast and cervical cancers in women often peak earlier in life. 21
However, gender inequities in healthcare exacerbate these differences. Oldest-old women are more likely to be underdiagnosed and undertreated due to limited access, sociocultural barriers, and symptom misrecognition.41,42 Alarmingly, cancer incidence and mortality in this group are rising. MENA recorded the world’s largest increase in breast cancer among women aged 70+ from 1990 to 2021, 43 driven by growing tobacco use, obesity, physical inactivity, and shifts in reproductive patterns.9,44,45 Similar surges in colorectal and lung cancers point to major gaps in awareness, prevention, and early detection.
The mortality burden is particularly concerning. Deaths from colorectal, lung, and pancreatic cancers are increasing, reflecting deficiencies across the cancer care continuum. Unlike high-income countries where colorectal cancer mortality is declining due to screening and timely treatment, MENA faces limited screening coverage, delayed diagnoses, and suboptimal treatment pathways. 46 Rising lung cancer among older women reflects both increasing smoking prevalence and persistent exposures to indoor air pollution and secondhand smoke.47,48
These patterns demand urgent action through gender-sensitive policies, stronger tobacco control, culturally tailored education, and expanded age-appropriate screening to address the distinct risks facing older men and women.
Interpreting Higher Mortality Than Incidence Rates Among the Oldest-Old
Our analysis revealed that cancer mortality rates among the oldest-old in MENA exceed incidence rates—an apparent paradox. This is partly driven by small and unstable denominators; as high all-cause mortality inflates per-100,000 estimates.13-15 Cancer is frequently underdiagnosed or missed because frailty, comorbidities, and limited access to diagnostic services preclude thorough investigations, and routine screening is typically discontinued in advanced age. 14 Consequently, deaths may be recorded as cancer-related based on clinical suspicion or proxy indicators without corresponding incidence entries, and inaccuracies in death certificates can further inflate mortality Figures.13,49 Registry limitations—particularly underreporting of non-biopsied cases—also suppress incidence, while mortality records tend to be more complete.
High case fatality contributes to the discrepancy, as the oldest-old often experience frailty, multiple comorbidities, delayed diagnosis, and limited eligibility for aggressive treatments.13,17 In many cases, diagnosis and death occur within the same year, further amplifying mortality relative to incidence. 49 Together, these factors underscore the urgent need to strengthen early detection, improve cancer registry completeness, and expand equitable access to age-appropriate diagnostic and treatment services for the oldest-old in MENA.32,50
Screening and Early Detection: Benefits, Limitations, and Gaps
In the oldest-old, reduced screening contributes to frequent late-stage diagnoses. 51 However, routine screening is often discouraged in this age group because of comorbidities, limited life expectancy, and the risks of overdiagnosis, psychological distress, and procedure-related harms.52-56 Many tumors are indolent and unlikely to affect survival given competing mortality risks. 51 For patients with a life expectancy under five years, screening offers little benefit; tools such as ePrognosis can support tailored decisions by estimating life expectancy and aligning care with patient values and preferences 52,57.
Major guidelines—including those of the American Cancer Society (ACS), the United States Preventive Services Task Force (USPSTF), and the American Geriatrics Society—converge on the principle that screening eligibility should weigh life expectancy, the risk of overdiagnosis, and the burden of treatment.58-65
In MENA, these challenges are amplified by absent or inconsistently adopted guidelines, limited public awareness, and restricted access to screening technologies, leading to frequent late-stage presentation. Addressing this requires regionally adapted, age-sensitive screening protocols, stronger patient–provider communication, and greater investment in health literacy and geriatric oncology.
Regional and Socioeconomic Disparities in Cancer Outcomes
Cancer incidence and mortality vary widely across MENA, shaped by differences in healthcare capacity, economic development, and cancer surveillance. In higher-income countries such as the UAE and Qatar, recorded incidence is higher due to stronger screening and reporting systems, whereas lower-income or conflict-affected settings like Syria and Yemen often report lower incidence but face higher mortality because of late-stage diagnoses and limited access to care.
The steepest increases in cancer among the oldest-old have been observed in the UAE and Iraq, while Qatar and Palestine show slower rises or even declines. These divergent patterns reflect variations in healthcare infrastructure, socioeconomic conditions, cancer control programs, and demographic composition—particularly the role of expatriates, who may access better healthcare or be excluded from national statistics. In better-resourced systems, timely screening, earlier detection, and effective treatment help mitigate mortality despite rising incidence.
As life expectancy increases across the region, the financial burden of cancer care on older populations is intensifying. In many MENA countries, where universal health coverage is lacking, older adults face substantial out-of-pocket costs for diagnostics, treatment, and palliative care. Limited affordability and restricted access to advanced therapies further widen disparities, leaving the oldest-old particularly vulnerable to poor cancer outcomes.
Key Systemic and Social Challenges
Outside the GCC, most MENA countries face major obstacles in caring for their oldest-old due to limited economic development and weak healthcare infrastructure. Declining fertility and shrinking workforces strain social welfare and healthcare financing, while demographic aging increases demand for cancer and chronic disease management. Older adults often present with late diagnoses, multiple comorbidities, and mental health needs, yet geriatric and palliative care services remain scarce.32,36,37,66,67 Ethical dilemmas around aggressive treatment vs comfort-focused care are further complicated by the scarcity of specialized training in geriatrics and palliative medicine. Early integration of palliative care specialists can play a crucial role in ensuring goal-concordant, patient-centered care for this vulnerable population.
Shifting cultural norms—driven by urbanization, migration, and extended work hours—have eroded traditional family-based eldercare.32,35-37 Caregivers, often family members, face significant stress and burnout, which undermines care quality.68,69 In rural or underserved areas, older adults may be particularly vulnerable to isolation, inadequate access to services, and, in extreme cases, neglect or abuse.
Policy implementation is also constrained by bureaucratic inefficiencies and weak intersectoral coordination. While some progress has been made, comprehensive eldercare programs remain rare. 70 Addressing these challenges will require integrated, culturally sensitive strategies that strengthen health systems, expand geriatric and palliative services, support caregivers, and ensure inclusive, evidence-based policies for the oldest-old.
Policy and Research Recommendations
The rising cancer burden among the oldest-old in MENA requires a comprehensive, context-specific response. Early detection should be enhanced through age-appropriate, non-invasive screening and greater awareness among both providers and the public, guided by life expectancy tools such as ePrognosis to ensure screening benefits those likely to gain from it. 57 Decisions about screening and treatment must be anchored in shared decision-making that respects patient values and preferences.
Expanding specialized services is equally critical. Geriatric oncology programs should incorporate multidisciplinary assessments of functional status and comorbidities, while palliative and supportive care—particularly in underserved areas—must be strengthened to ensure affordable, age-sensitive services that prioritize quality of life. Greater inclusion of the oldest-old in clinical trials is also essential to build region-specific evidence for care.
Targeted public health measures can reduce preventable cancers and comorbid conditions by addressing tobacco use, poor diet, physical inactivity, and low uptake of preventive vaccinations such as HPV and hepatitis B. 45 At the system level, investments in aging-responsive health systems, comprehensive cancer registries, and workforce training are vital, alongside stronger community-based eldercare and caregiver support.
Finally, region-specific guidelines tailored to MENA’s sociocultural and economic contexts are urgently needed, with active involvement of the oldest-old in both policy design and research. 68 Emerging hotspots—such as Iraq and Egypt, where incidence and mortality are rising steeply—require targeted national cancer control strategies. Collectively, these steps underscore the urgency of implementing age- and gender-sensitive cancer policies to ensure equitable and effective care for the oldest-old across the region.
Limitations
This study has several limitations. Although GBD data are comprehensive and widely used, they rely on modeling and imputation to fill gaps in primary data, which can introduce uncertainties—particularly in regions like MENA, where cancer registration systems are often incomplete or inconsistent. Moreover, when available, most registries aggregate data into a final age category of 75 years and above, limiting age-specific analyses for the oldest-old population. The use of Joinpoint regression to assess trends is also sensitive to data quality; in low-resource settings, observed changes may partly reflect improvements in reporting or diagnostic capacity rather than true shifts in cancer burden. Cancer registration remains underdeveloped in many MENA countries due to logistical, political, and financial challenges, which undermines data reliability and comparability. 50
Furthermore, the analysis does not adjust for potential confounders such as comorbidities, lifestyle behaviors, or environmental exposures, all of which may influence cancer trends in the oldest-old. Future research should integrate more granular, country-specific data and account for these factors to provide a more nuanced understanding of cancer epidemiology in older populations. Such efforts will be essential for guiding tailored cancer control strategies and optimizing resource allocation in diverse and complex settings such as the MENA region.
Conclusion
Cancer among the oldest-old is an emerging public health priority in the MENA region, driven by rapid demographic aging and rising incidence and mortality. Addressing this challenge requires age-sensitive cancer control strategies, equitable access to healthcare, strengthened caregiver support, and interventions that overcome barriers such as low health literacy and high comorbidity rates. Reliable, age-specific data through strengthened cancer registries are essential to guide evidence-based planning and policy. Meaningful inclusion of the oldest-old in research, policy design, and service delivery is equally critical to ensure that their needs are not overlooked. Moving forward, MENA health systems must expand preventive strategies, invest in infrastructure, and develop geriatric oncology and palliative services tailored to this vulnerable and growing population—securing equitable and sustainable cancer care for the region’s oldest-old.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.