
Abstract
Background
Lung cancer is one of the most common malignant tumors in the world. It has become an increasingly important public health problem in China. In this study, we systematically assessed the lung cancer situation in China from 1990 to 2019 and provided an epidemiological knowledge base for the revision of health policies. The relevant data were extracted from the Global Burden of Disease (GBD) database.
Methods
Based on GBD 2019 data, we evaluated the incidence, prevalence, and death rates of lung cancer in China and their change trends from 1990 to 2019, making comparisons by gender and age.
Results
The age-standardized incidence and death rates (ASIR and ASDR, respectively) of lung cancer in China were higher than the average levels in Asia, Africa, Europe, and Oceania and also higher than those of neighboring Asian countries. Lung cancer rose from the seventh leading cause of death in 1990 to the fourth leading one in 2019, indicating that the disease burden of lung cancer is increasing. In 2019, the incidence, prevalence, and death rates of lung cancer were all higher in men than in women across all age groups. All three indices were lower in men and women <50 years old than in men and women >50 years. From 1990 to 2019, the ASIR, age-standardized prevalence rate (ASPR), and ASDR showed trends of increase (P < .05), and the rise in the ASPR (average annual percentage change [AAPC] = 1.9) was greater than those in the ASIR (AAPC = 1) and ASDR (AAPC = .8).
Conclusions
From 1990 to 2019, the incidence, prevalence, and death rates of lung cancer continued to increase in China. To reduce this burden, prevention and management of known risk factors should be promoted through national policies.
Introduction
Lung cancer is estimated to be the second most commonly diagnosed cancer and was the leading cause of cancer deaths worldwide in 2020, accounting for approximately 1 in 10 of all cancer cases (11.4%) and 1 in 5 cancer deaths (18.0%). It is the leading cause of cancer incidence and mortality in men, the third most common cause of cancer mortality overall, and the second most common cause of cancer mortality in women. The incidence and death rates of lung cancer in developing countries are three to four times higher than those in developed countries. 1 As one of the biggest developing countries, China has experienced rapid economic growth and healthcare reform, and risk factors for lung cancer in the country are also changing continually.2,3 According to the latest data released by the National Cancer Center in 2022, lung cancer ranks first in terms of incidence and death rates, 4 and the 5-year survival rate for lung cancer in China is 19.7%, lower than the global average of 40.5%. 5 With China’s industrialization, urbanization, and aging population, lung cancer has come to seriously threaten the health of China’s residents and become a major public health problem hindering the country’s economic development.2,6
For this study, we obtained Institute for Health Metrics and Evaluation Global Burden of Disease (GBD; https://vizhub.healthdata.org) data by geographical location, gender, age, and year. These data included 369 kinds of disease incidence, mortality, and disability, as well as 87 kinds of risk factors, to be quantified. 7 This provided a unique opportunity to understand the burden of lung cancer in China. By analyzing GBD data, we can better understand China’s global ranking in the distribution of lung cancer. Our findings should help us better understand lung cancer, evaluate current prevention strategies, plan for nationwide management of the burden imposed by lung cancer, and improve health management systems to meet future challenges.
Materials and Methods
Data Sources
This study analyzed the disease burden of lung cancer in China from 1990 to 2019. This burden was estimated using data from a variety of sources. Mortality data were mostly obtained from the National Disease Surveillance System, the Cause-of-Death Network Reporting System of the Chinese Center for Disease Control and Prevention, the Maternal and Child Health Monitoring System of China, the China Tumor Registry, cause-of-death reports from Hong Kong and Macao, and other published and unpublished reports. Incidence data mainly came from literature searches, survey data, monitoring data, clinical data such as those for hospitalizations and outpatient visits, and health insurance data. 8 The data used in this study are publicly available, and the means by which we recorded information for this article did not involve human tissues or samples, so this study is not required for the benefit of an international reader.
The GBD 2019 database was structured following the International Classification of Diseases, 10th edition. In this study, we used the GBD Results Tool to retrieve lung cancer disease burden data for China. “China” was selected as the location; “1990 to 2019” as the years; “Number and Rate” as metrics; “Incidence, Prevalence and Deaths” as measures; “Male, Female, Both” as genders; and “Lung cancer” as the cause. We reported 95% uncertainty intervals derived from 1000 draws from the posterior distribution of each step in the estimation process per established GBD methods.
Statistical Analyses
We conducted descriptive analyses of the incidence, prevalence, and death rates of lung cancer by gender, age, and year. The age groups we used were the same ones used in GBD 2019. Three rough age groups (15–49 years, 50–69 years, and ≥70 years) were analyzed for 1990 and 2019. In our detailed descriptions of 2019 lung cancer incidence, prevalence, and death rates, we grouped cases by age for every 5 years. Because such rates in patients <10 years old were nonexistent, we combined the age groups 0–4 years and 5–9 years into a single group.
The joinpoint model was used to analyze the time trend of the age-standardized incidence, prevalence, and death rates (ASIR, ASPR, and ASDR, respectively) of lung cancer from 1990 to 2019. To reduce the possibility of false trend changes during the reporting period, we restricted all models to a maximum of two joinpoints (three-line segments). 9 Trends were expressed as annual percentage change (APC), and the Z-test was used to assess whether APC was statistically different from zero. When describing trends, we used the term “increase” or “decrease” if the slope of the APC trend was statistically significant (P < .05). For nonstatistically significant trends, the term “stable” was used.
Results
Global Age-Standardized Death and Incidence Rates of Lung Cancer
Figure 1 shows the worldwide geographic distribution of the ASIR of lung cancer. This index was higher in China (41.71/100 000) than in Asia overall (27.82/100 000), Africa (10.46/100 000), Europe (33.37/100 000), and Oceania (21.63/100 000) and slightly lower than in North America (44.96/100 000). Furthermore, the ASIR of lung cancer was higher in China than in South Korea (35.60/100 000), Japan (30.66/100 000), North Korea (27.88/100 000), and India (7.70/100 000). Figure 2 shows the geographic distribution of the global ASDR of lung cancer. This index was higher in China (38.70/100 000) than in Asia overall (25.76/100 000), Africa (11.15/100 000), North America (35.89/100 000), Europe (29.55/100 000), and Oceania (22.89/100 000). Furthermore, the ASDR of lung cancer was higher in China than in North Korea (28.54/100 000), South Korea (26.30/100 000), Japan (21.21/100 000), and India (8.07/100 000). Geographical distribution of incidence rate per 100 000 lung cancer cases worldwide in 2019. Geographical distribution of death rate per 100 000 lung cancer cases worldwide in 2019.

Top 15 Causes of Death and Their Corresponding Rankings in 1990 and 2019
In China, as healthcare has progressed and medical/health awareness has been heightened, the death rates of lower respiratory disease and neonatal diseases have decreased significantly over the past 30 years. The diseases whose death rates have increased year by year are chronic noncommunicable diseases and geriatric diseases. In 1990, the death rate of lung cancer ranked seventh among all causes of death. Over the past 30 years, lung cancer has overtaken stomach cancer, lower respiratory disease, and neonatal diseases to become the fourth leading cause of death in 2019. This indicates that this type of cancer poses a very high burden among all causes of death. Because China has seen the aging of its population, urban industrialization, environmental pollution, and the advent of unhealthy lifestyles in recent years, the ranking of lung cancer among all other causes of death in China might continue to rise in the future (Figure 3). Ranking of death rate for death-related causes in China.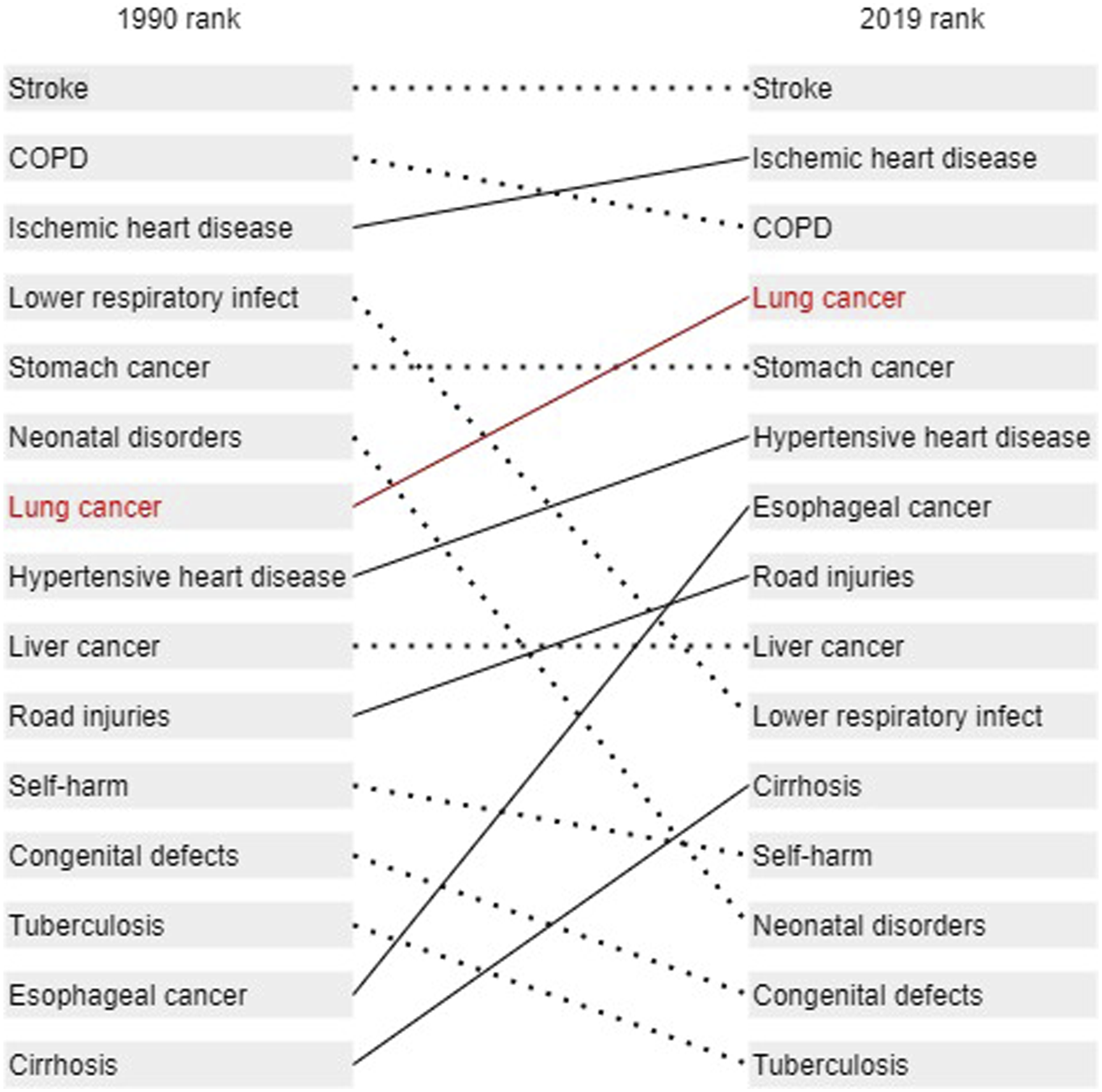
Age Characteristics in the Incidence, Prevalence, and Death Rates of Lung Cancer
Incidence, Prevalence, and Death Rate of Lung Cancer in China by Gender and Age in 2019 (per 100 000).

Trend Analysis of the Age-Standardized Incidence, Prevalence, and Death Rates of Lung Cancer
Age-Standardized Incidence, Prevalence, and Death Rate Trends of Lung Cancer by Sex.

Note:* Representative P<.05.

Age-standardized incidence, prevalence, and death rates of lung cancer in both genders, male and female only.
Changes in the Incidence, Prevalence, and Death Rates of Lung Cancer in Different Age Groups Over the Past 30 Years
The incidence, prevalence, and death rates of lung cancer increased in all three age groups (15–49 years, 50–69 years, and ≥70 years) in 2019 over those in 1990, with the largest increases in the ≥70 age group (78%, 135%, and 58%, respectively). The increase was smallest in the 50–69 age group. In terms of gender differences, except in the 50–69 age group, the incidence and death rates of lung cancer increased more in men than in women, the incidence in all age groups, incidence and death rates in other age groups were higher in women than in men (Figure 5). Comparison of age-related incidence, prevalence, and death rates of lung cancer between 1990 and 2019.
Discussion
Lung cancer is a multistep, multifactorial disease with multiple histological subtypes and is the most fatal cancer worldwide. Its cause is unknown. Smoking and air pollution are two important risk factors;10,11 others, such as occupational exposure (e.g., asbestos), also play important roles in the occurrence and development of this cancer. 12 In recent years, lung cancer in both men and women in China has ranked first among all malignancies in both incidence and death rates, posing a huge threat to human health. 4 Therefore, clarifying lung cancer characteristics and trends by gender and age in China can provide basic information for cancer prevention and control and ultimately reduce the incidence and mortality of this disease.
With the rapid improvement in China’s economic level and the acceleration of urbanization and aging, the lifestyle and disease spectra of Chinese residents have changed greatly. 13 In 1990, lung cancer ranked seventh among all causes of death in the country but rose to fourth place by 2019, indicating that this form of cancer poses an increasingly serious disease burden. Death rates from lung cancer in China compared with the rest of the world are likely to continue to increase in the future. The global map of the disease’s geographic distribution shows that its ASIR and ASDR vary significantly by continent and country. A comparison with neighboring Asian countries showed that the ASIR and ASDR of lung cancer were higher in China than in North Korea, South Korea, Japan, and India. This higher burden was mainly due to China’s population growth and aging 14 and was therefore positively correlated with the country’s rising socioeconomic status. 15
Continuous monitoring of cancer data is vital to effective cancer control policy. Tracking trends in the incidence, prevalence, and death rates of cancer is important not only to cancer control planning and to evaluating the effectiveness of existing policy but also to generating etiological hypotheses and to identifying specific and potentially modifiable risk factors for specific cancers.16,17 The results of this study showed that the ASIR of lung cancer increased from 30.20/100 000 in 1990 to 41.71/100 000 in 2019 and its ASPR from 31.05/100 000 in 1990 to 55.13/100 000 in 2019. The ASDR of lung cancer increased from 31.18/100 000 in 1990 to 38.70/100 000 in 2019. These three indices showed trends of increase over time, more so for men than for women, and their AAPCs were statistically significant. Local-trend analysis showed that the ASIR and ASDR increased the most from 1996 to 2005 (respective APCs, 2.67 and 2.38). According to the China Statistical Yearbook, the total number of hospitalized lung cancer patients increased rapidly from 142 674 in 1996 to 364 484 in 2005. The total hospitalization cost of lung cancer increased by 16.15% annually, from Ұ1.547 billion in 1999 to Ұ3.799 billion in 2005. 18 A study by Zhang et al. reported that the per capita economic burden of lung cancer patients in China is $43,336, of which the direct cost is $42,540 (98.16%) and the indirect cost $795 (1.84%); the disease’s per capita economic burden in the first year after diagnosis is $30,277, accounting for 171% of annual family income. 2 Another study by Shi found that the average direct medical cost of lung cancer patients in China from 1996 to 2011 was Ұ10,415–Ұ27,595, with an annual growth rate of 2.2%. It has been suggested that the serious-illness insurance system should be further improved. 19 One reason for the increased incidence of lung cancer in China is that the country produces and consumes the most tobacco worldwide, accounting for approximately 30% of global tobacco use. According to relevant epidemiological data, 75.04% of male and 18.35% of female deaths from lung cancer can be attributed to tobacco use, indicating that smoking is the main risk factor for lung cancer.20,21 Cigarette smoke contains >60 known carcinogens, and the risk of lung cancer for smokers is 6–10 times that for nonsmokers. 22 An estimated 350 million people smoke in China, and 72.4% of nonsmokers in China are exposed to secondhand smoke. There have been no significant improvements in smoking rates, quitting rates, or rates of exposure to secondhand smoke.23,24 Indoor air pollution from unventilated coal stoves and cooking fumes might also be a major risk factor for lung cancer. 25 China’s rapid industrialization has improved the quality of life and health for its residents overall, but the concomitant rise in energy consumption has increased industrial waste emissions, which include toxic substances that degrade air quality and thus constitute another major risk factor for lung cancer.26,27 Therefore, taking population growth and aging into account, more work is needed to reduce the incidence of lung cancer through health education and science popularization. In the current study, local-trend analysis also showed that the ASDR showed a decreasing trend from 2005 to 2019 (APC = −.17) and that the decrease in men (APC = −.77) was greater than that in women (APC = −.37). This decrease might be related to improvements in lung cancer treatment, 28 the implementation of early-diagnosis and -treatment screening projects for lung cancer, 29 and the improvement of lung cancer screening technology, all of which boost the early-diagnosis and -treatment rates of lung cancer and in turn improve patients’ survival rates.
Our study showed that the incidence, prevalence, and death rates of lung cancer were relatively low below the age of 50 and increased significantly afterward. The disease burden represented by these three indices increased rapidly from age 50 onward. The Expert Consensus on Low-dose Spiral Computed-tomography (CT) Screening for Lung Cancer, published by the Cardiothoracic Group of the Radiology Society of the Chinese Medical Association in 2015, 30 and the Chinese Guidelines for Low-dose Spiral CT Screening for Lung Cancer, published by Zhou Qinghua et al in 2018, 31 agree that the initial age of lung cancer screening in Chinese population be set at 50 years. This is consistent with the age at which we found lung cancer to increase.
In this study, we divided subjects into three groups: 15–49 years, 50–69 years, and ≥70 years. The incidence, prevalence, and death rates in the ≥70 age group were highest and increased the fastest in 2019 than in 1990, indicating that disease burden was highest in this group. The possible reason is that it takes decades of smoking for lung cancer to occur and develop, and the elderly population has higher rates of basic diseases and lower immunity, causing the incidence, prevalence, and death rates of lung cancer to peak in this demographic.32,33 We also found that although all three indices were high in the 50–69 than in the 15–49 age group, the change rate of all three was higher in the latter than in the former, which might be related to the rising number of young smokers in recent years.34,35 Globally, it is estimated that approximately 15 million people aged 13–28 years are regular smokers and that a further 40 million in this age range smoke occasionally. In China, the average starting age for smokers is 19 years, and the smoking rate of men (60%) is much higher than that of women (<5%). However, compared with 1990, the incidence, prevalence, and death rates of lung cancer in China increased faster in women than in men in 2019, which might be related to women’s frequent exposure to secondhand smoke. Indoor air pollution from unventilated coal stoves and cooking fumes might be another major risk factor for women.36,37
There were some limitations to this study. Due to data limitations, we could not compare incidence and death rates of lung cancer among different provinces and regions in China and therefore could not reflect regional differences in these indices.
Conclusions
Lung cancer remains the malignant tumor that most endangers the health of China’s residents; its incidence, prevalence, and death rates remain high. In particular, the incidence rate of lung cancer in women has increased significantly. Lung cancer patients are still mainly elderly, but the disease has been trending obviously in younger people, causing a great economic burden. Therefore, we should continue to strengthen healthcare reform and expand health insurance coverage to reduce the financial burden on patients.
Footnotes
Author Contributions
(I) Conception and design: Huixin Sun; (II) administrative support: Haiyu Zhang; (III) collection and assembly of data: Huilong Cai and Weiguang Yuan; (IV) data analysis and interpretation: Fengjiao Wang and Yang Jiang; (V) manuscript writing: all authors; (VI) final approval of manuscript: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of Heilongjiang Province [No. YQ2021H021].