
Abstract
Background
This study meticulously outlines the evolution of the burden of malignant neoplasm of bone and articular cartilage (MNBAC) among different age and sex groups in China from 1990 to 2021, analyzes the global impact of the disease, and predicts the trend of disease burden up to 2035.
Methods
Leveraging public data from the Global Burden of Disease (GBD) database spanning 1990 to 2021, this study thoroughly analyzed the characteristics of the burden of MNBAC in China and globally, including its incidence, prevalence, mortality, and disability-adjusted life years (DALYs). The joinpoint analysis method was employed to calculate the average annual percentage change (AAPC) and its 95% uncertainty interval, revealing the trend of MNBAC’s impact. Furthermore, Bayesian age–period–cohort (BAPC) model was used to forecast changes in disease burden leading up to 2035.
Results
Between 1990 and 2021, the age-standardized incidence rate (ASIR) of MNBAC in China increased from 0.65 to 1.42 per 100 000 people, and the global ASIR rose from 0.97 to 1.11 per 100 000. The AAPC for China’s ASIR, age-standardized prevalence rate (ASPR), age-standardized mortality rate (ASMR), and age-standardized DALYs rate (ASDR) were 2.59%, 2.71%, 1.52%, and 1.26%, and the AAPC of ASIR and ASPR of the global burden of MNBAC were 0.44% and 0.51%, respectively. The effect of age and sex on the burden of MNBAC showed significant differences. Forecasting analyses suggest that from 2022 to 2035, the burden of MNBAC in China and globally will show a declining trend.
Conclusions
From 1990 to 2021, the disease burden of MNBAC in China has been rising among the population, particularly pronounced among older men. Although forecasts indicate a gradual reduction in the future burden of MNBAC, given China’s large population base and the increasing trend of population aging, MNBAC will pose a public health challenge in China.
Plain Language Summary
Background: This study examines the evolution of the burden of malignant neoplasm of bone and articular cartilage (MNBAC) in China and globally from 1990 to 2021 and predicts trends up to 2035. Methods: Using data from the Global Burden of Disease (GBD) database (1990-2021), incidence, prevalence, mortality, and disability-adjusted life years (DALYs) of MNBAC were analyzed in China and globally. In the joinpoint analysis, the average annual percentage changes (AAPCs) and 95% uncertainty intervals were calculated. The Bayesian age–period–cohort (BAPC) model forecasted disease burden up to 2035. Results: From 1990 to 2021, China’s age-standardized incidence rate (ASIR) of MNBAC increased from 0.65 to 1.42 per 100 000, whereas the global ASIR increased from 0.97 to 1.11 per 100 000. China’s AAPCs for ASIR, age-standardized prevalence rate (ASPR), age-standardized mortality rate (ASMR), and age-standardized DALYs rate (ASDR) were 2.59%, 2.71%, 1.52%, and 1.26%, respectively. Global AAPCs for ASIR and ASPR were 0.44% and 0.51%, respectively. Age and sex significantly affected the burden of MNBAC. Forecasting suggests a declining trend in the burden of MNBAC from 2022 to 2035. Conclusion: The burden of MNBAC in China increased from 1990 to 2021, particularly among older men. Despite a projected decline, MNBAC remains a significant public health challenge due to China’s large and aging population.
Introduction
The term “bone tumor” includes all tumors of the bone or its components, including primary, secondary, and metastatic bone tumors. Primary malignant bone tumors exhibit a wide range of clinical and biological heterogeneity and are a group of extremely rare tumors that arise from the skeleton. Currently, malignant bone tumors are often observed as osteosarcomas, chondrosarcomas, and fibrosarcomas of bone. 1 Osteosarcoma is the most common type of bone cancer in children and young people, characterized by a bimodal age distribution, with a peak occurring between 15 and 20 years and another at age >65 years.2,3 This rare bone tumor is recognized for its rapid growth. 4 Chondrosarcoma, a common primary bone tumor, is characterized by hyaline cartilage formation and is often observed in the aging population. 5 Additionally, the bones and bone marrow are the most common sites for cancer metastasis.6,7 Bone metastasis develops in approximately 1.1 years, with the rates of bone metastasis arising from solid tumors being 4.8% and 8.4% 1 and 10 years after diagnosis, respectively. 8 Notably, bone metastasis is identified in 11% of patients with advanced stage IV within just 30 days. Sadly, those with bone metastasis have a median survival span of 2-3 years. 9 Given the uncommon and heterogeneous nature of primary bone malignancies and the high prevalence of bone metastasis, malignant bone tumors represent a major public health challenge across the globe. Thus, a complete understanding of the disease burden and epidemiological trends associated with bone tumors is imperative.
Currently, reports on the burden of MNBAC in GBD studies have mainly focused on macro assessments at the global and regional levels. A study estimated the global trends and attributable risks of MNBAC from 1990 to 2021 to examine their relationship with socioeconomic development. 10 Globally, the ASIR for MNBAC is 0.8-1.2/105 in men and 0.5-1.0/105 in women. Although the incidence and mortality rates of MNBAC are increasing, the increase is relatively slow. Nevertheless, substantial variations are observed across different regions, with East Asia, Southeast Asia, and Central Latin America experiencing a particularly heavy burden. Furthermore, the global incidence and mortality of MNBAC exhibit a bimodal distribution, with high incidence rates in adolescents (15-19 years) and older adults (>60 years). Significantly, the incidence and mortality rates of MNBAC are negatively correlated with socioeconomic indicators such as the human development index and healthcare access. Regions with a low sociodemographic index face greater challenges in disease management. 11 However, existing investigations have mainly addressed the issue from a global perspective, without further exploring the heterogeneity among different nations and areas, overlooking the specific details within individual countries. China is one of the countries with the heaviest disease burden of MNBAC globally, contributing 28.39% and 27.35% of the global incident and death cases, respectively, in 2021. From 1990 to 2021, the crude incidence rate of MNBAC in China increased from 0.54/105 to 1.82/105, a growth rate that far exceeds the global level. 12 In addition, China, as one of the most populous countries in the world, has yet to see a thorough investigation into the trajectory of MNBAC within its demographic structure.
This study, based on the latest GBD data, aimed to comprehensively analyze and compare the burden of MNBAC in China and the world from 1990 to 2021. The jointpoint regression analysis was applied to investigate the trend in MNBAC over time, and a detailed assessment of the variations in burden in relation to age and sex for 30 years was conducted. Employing the Bayesian age–period–cohort (BAPC) model, this study projected the burden trends for the next 15 years. The intention was to improve the understanding of the health effect on populations and guide the development of preventive strategies and health resource allocation.
Methods
Data Source
This study is an observational study. Data were collected from the GBD 2021 database (https://vizhub.healthdata.org/gbd-results/), which is freely accessible for download after registration. 13 Data collected included global and China-specific datasets, encompassing data on incidence, ASIR, prevalence, ASPR, mortality, ASMR, disability-adjusted life years, and ASDR from 1990 to 2021, along with data for various age groups. The International Classification of Diseases, 10th Edition (ICD-10), codes for MNBAC included C40–C40.92, C41.0–C41.4, and C41.8–C41.9. The ICD-9 codes are 170-170.9. 14 The requirement for ethical approval was waived because of the absence of direct human participant involvement.
Joinpoint Regression Model
Data were sourced from the GBD 2021 database, which can be downloaded for free upon registration. A comprehensive trend analysis of the ASIRs, ASPRs, ASMRs, and ASDRs for MNBAC was conducted using Joinpoint 4.9. 15 This joinpoint regression model is an extremely valuable tool because it can accurately identify significant change points, known as joinpoints, in the time trends of disease burden indicators such as incidence and mortality rates. These joinpoints skillfully divide long-term trends into multiple stages, thereby precisely depicting the dynamic changes in disease burden. 16 In this study, a log-linear model with a maximum of four joinpoints and 4499 Monte Carlo random sampling tests were employed to analyze these trends. The annual percentage change (APC) for each segment and the AAPC for the overall trend were also calculated. An AAPC (P < 0.05) that is positive or negative is considered a significantly increasing or decreasing trend. An AAPC with a P value >0.05 is presented as a nonsignificant increasing or decreasing trend. If the P value is > 0.05 and the AAPC is between −0.5 and +0.5, the trend is reported as stable. 17 Compared with traditional statistical techniques, joinpoint analysis has a greater advantage in dealing with complex trend data because it can sensitively capture nonlinear changes in the data without preassuming that the overall trend of the data is linear. However, the results of the joinpoint analysis are largely contingent upon the quality of the input data. In the presence of missing, inaccurate, or biased data, misjudging joinpoints or misinterpreting trends is possible. Although joinpoint analysis excels in handling complex trends, it is still based on some assumptions. If the actual data do not align with these assumptions, the result may be a poor model fit. Note that joinpoint analysis is essentially a descriptive statistical method, limiting drawing conclusions about causality. 18
Bayesian Age–Period–Cohort Model
This study employed the integrated nested Laplace approximation (INLA) framework combined with the Bayesian age–period–cohort (BAPC) model to forecast the disease burden of MNBAC in China and globally from 2022 to 2035. The standard age population data and projected population data for 2100 were sourced from relevant literature.19,20 The combination of the INLA framework and the BAPC model allows for the approximation of marginal posterior distributions, effectively avoiding the mixing and convergence issues associated with traditional Bayesian methods that depend on Markov chain Monte Carlo sampling. 21 The BAPC model’s capacity to simultaneously account for age, period, and cohort effects allows for a more thorough examination of the complex dynamics of disease burden. The Bayesian approach naturally accommodates data uncertainties and integrates them into the model estimation process. This is especially important when working with the GBD database, which may have missing or poor-quality data. Bayesian models provide not only point estimates but also credible intervals, which help in assessing the reliability of model predictions. Additionally, the Bayesian method allows researchers to include prior knowledge in the model, thereby improving its accuracy and robustness. 22 By considering multidimensional temporal effects, the BAPC model can more accurately predict future trends in disease burden. This is of great significance for public health decision-making, as it enables policymakers to develop more effective intervention measures.
Statistical Analysis
R version 4.3.2 in combination with the ggplot2 package from Joinpoint version 4.9 was utilized for the statistical analysis and visualization of the data. BAPC analyses were conducted using the R packages “BAPC” (version 0.0.36) and “INLA.” A P value of <0.05 was considered significant.
Ethical Statement
This study complied with the GATHER guidelines. 23 The data analyzed were aggregated, ensuring that no information about individual patients or public personnel was directly implicated.
Results
Description of the Burden of MNBAC in China and Its Incidence in China and Globally
All-Age Cases and Age-Standardized Incidence, Prevalence, Mortality, and DALYs Rates and Corresponding AAPC of MNBAC in China and Globally in 1990 and 2021

UI, uncertainty interval; AAPC, average annual percentage change; DALYs, disability-adjusted life-years; MNBAC, malignant neoplasm of bone and articular cartilage.
Prevalence of MNBAC in China and Globally
The prevalence of MNBAC in China has significantly increased, with cases increasing from 41 612 in 1990 (95% UI 27 308-73 249) to 166 569 in 2021 (95% UI: 104 517-219 818), a threefold increase. In contrast, the global prevalence has grown from 306 463 in 1990 (95% UI 276 180-356 571) to 598 638 in 2021 (95% UI 483 776-672 738), a 95.3% increase. The global ASPR has also increased from 6.25 per 100 000 people in 1990 to 7.3 per 100 000 people in 2021. In China, the ASPR has risen from 4.06 per 100 000 people in 1990 to 9.16 in 2021. Over the same period, the AAPC of China’s prevalence rate has increased by 2.71% (95% UI 2.37-3.05), whereas the AAPC of the global prevalence rate has seen a smaller increase of 0.51% (95% UI 0.40-0.62; Table 1).
MNBAC Mortality in China and Globally
Globally, the rate of mortality due to MNBAC increased, with 66 114 fatalities reported in 2021 (95% UI 53 305-74 467), representing a 15.60% increase since 1990. In contrast, China experienced a more pronounced increase in mortality rate, with an increase of 85.9% over the same period. The global ASMR demonstrated a minimal change, being 0.79 per 100 000 individuals in 1990 (95% UI 0.73-0.93) and persisting at 0.79 in 2021 (95% UI 0.64-0.89). However, China’s ASMR rose from 0.58 per 100 000 individuals in 1990 (95% UI 0.38-1.03) to 0.93 in 2021 (95% UI 0.58-1.23). Additionally, from 1990 to 2021, China’s mortality rate exhibited an AAPC increase of 1.5163% (95% UI 1.16-1.87), whereas globally, no notable variations were noted (Table 1).
DALYs of MNBAC in China and Globally
Globally, the DALYs for MNBAC increased from 1,578,316 in 1990 (95% UI 1,404,401-1,882,612) to 2,525,828 in 2021 (95% UI 2,064,233-2,844,215), which was a 60.0% increase compared with 2019 data. In China, a 1.43-fold rise in DALYs was noted from 1990 to 2021. The global ASDR remained relatively constant, with 31.03 per 100 000 people in 1990 (95% UI 27.79-36.86) and 31.06 in 2021 (95% UI 25.44-35.03). In China, the ASDR increased from 20.16 per 100 000 people in 1990 (95% UI 13.12-35.68) to 29.52 in 2021 (95% UI 18.92-38.67). During the same period, the AAPC in global DALYs showed no significant change, whereas China’s AAPC increased by 1.26% (95% UI 1.01-1.51; Table 1).
Joinpoint Regression Analysis of the Burden of MNBAC in China and Globally
Figures 1 and 2 depict the joinpoint regression analysis of the burden of MNBAC in China and globally from 1990 to 2021. In 1990-1992, the APC in China’s MNBAC ASIRs and ASPRs significantly declined. However, they increased from 1992 to 2007, slightly declined after 2008, and fluctuated (Figure 1A and B). Global ASIR and ASPR significantly increased overall from 1990 to 2005, plateaued from 2012 to 2018, and began to decrease from 2019 (Figure 2A and B). China’s ASMRs for MNBAC showed a notable decline from 1990 to 1992, increased significantly until 2007, and then gradually decreased, with a more significant reduction than is observed globally (Figure 1C). The global ASMR for MNBAC started to increase significantly from 2001, leveled off after 2004, and generally began to decline from 2007 (Figure 2C). China’s ASDR for MNBAC exhibited a downward trend from 1990 to 1992, significantly increased after 1992, stabilized after 2004, and started to significantly decrease after 2008 (Figure 1D). Globally, MNBAC’s ASDR exhibited a slight upward trend from 1990, fluctuated, and displayed an overall downward trend after 2005 (Figure 2D). Although the APC trends for ASIR and ASPR in China were comparable to the global trends, the declines in China’s ASMR and ASDR were more significant than the global declines. The APC of ASIR, ASPR, ASMR, and ASDR of MNBAC in China from 1990 to 2021. A: ASIR; B: ASPR; C: ASMR; D: ASDR The APC of ASIR, ASPR, ASMR, and ASDR of MNBAC in global from 1990 to 2021. A: ASIR; B: ASPR; C: ASMR; D: ASDR

Burden of MNBAC in Different Age Groups in China and Globally
Figure 3 compares the incidence, prevalence, and mortality rates and DALYs of MNBAC in China for different age groups in 1990 and 2021, along with their corresponding crude incidence rates (CIR). The number of new cases revealed two peaks in MNBAC occurrence, one at age 10-14 years and the other at age 65-69 years, with the group aged 65-59 years having the highest case count. In 1990 and 2021, the Chinese group aged 85-89 years had the highest CIR for MNBAC. The incidence rates in 2021 were significantly higher across all age groups compared with data in 1990. In contrast, the global CIR for MNBAC in 2021 showed an increasing trend in all age groups; however, the increase was less pronounced than that in China. Similar trends were noted in the crude prevalence rates. The peak prevalence of MNBAC in China was noted in the group aged 75-79 years, in contrast to the global peak in the group aged 15-19 years. In terms of mortality, the group aged 70-74 years had the most deaths in both 1990 and 2021. The crude mortality rate (CMR) for MNBAC exhibited a minor peak at age 15-19 years and a major peak at 85-89 years, and the global CMR for MNBAC in 2021 revealed a significantly increasing trend in people aged >50 years compared with that in 1990. However, globally, mortality rates minimally fluctuated among age groups. The peak DALY in 1990 was noted in the group aged 15-19 years, shifting to the group aged 65-69 years by 2021. A marked increase in the crude disability rate (CDR) was also observed in older age groups, with no significant changes in the global CDR. The global burden across age groups is detailed in Supplemental Figure 1. A comparative study of disease incidence, prevalence, mortality, DALYs, and their crude ratios among various age cohorts in China between 1990 and 2021. A: incident cases and CIR; B: prevalent cases and CPR; C: death cases and CMR; D: DALYs cases and CDR. bar charts represent counts; lines represent crude rates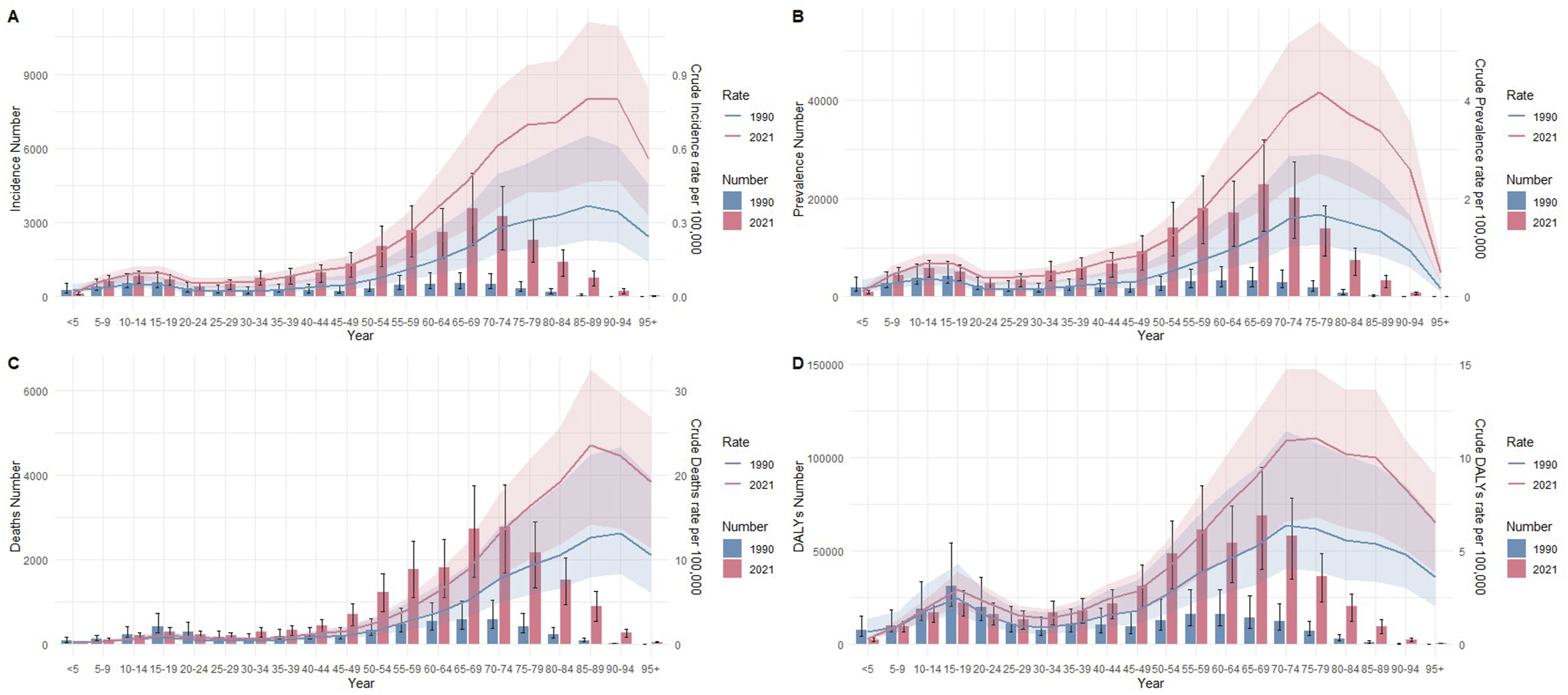
Sex Disparities in the Burden of MNBAC in Different Age Groups in China and Globally
Figure 4 illustrates the incidence, prevalence, and mortality rates and DALYs of MNBAC among different age groups of men and women in 1990 and 2021 in China. In 1990, the incidence in male teens peaked in the group aged 15-19 years, followed by the group aged 65-69 years, whereas for women, the incidence peaked in the group aged 10-14 years, followed by the group aged 70-74 years. Across all age groups (age 5-84 years), men consistently had a higher incidence of MNBAC than women. Fast forward to 2021, the incidence peak for both sexes was noted in the group aged 65-69 years, followed by those aged 70-74 years (Figure 4A). The prevalence results in China for 2021 were comparable to the incidence findings, whereas globally, the prevalence rates in men were significantly higher than those in women in 2021 (Figure 4B, Supplemental Figure 2). When comparing the number of deaths between men and women in 1990, more deaths were noted in all groups aged >90 years, with the peak mortality for men occurring at age 65-69 years and for women at 70-74 years. The group aged 15-19 years had a notably high proportion of deaths for both sexes, a phenomenon that became less apparent by 2021. Comparing mortality in 1990, men had more deaths in all groups aged >90 years, with the peak mortality occurring for men aged 65-69 years and for men aged 70-74 years. The proportion of deaths was significantly in the group aged 15-19 years for both sexes, a trend that became less pronounced by 2021. In 2021, more deaths involved more men than women, with the peak mortality for both sexes occurring at age 70-74 years. MNBAC mortality rates increased with age for both sexes, peaking and then declining (Figure 4C). The peak DALYs for both sexes occurred in the group aged 15-19 years in 1990, shifting to the group aged 65-69 years by 2021, with men generally having more DALYs than women (Figure 4D). Comparison of the number of incidence, prevalence, mortality, and DALYs of MNBAC in males and females of different age groups in China in 1990 and 2021. A: 1990; B: 2021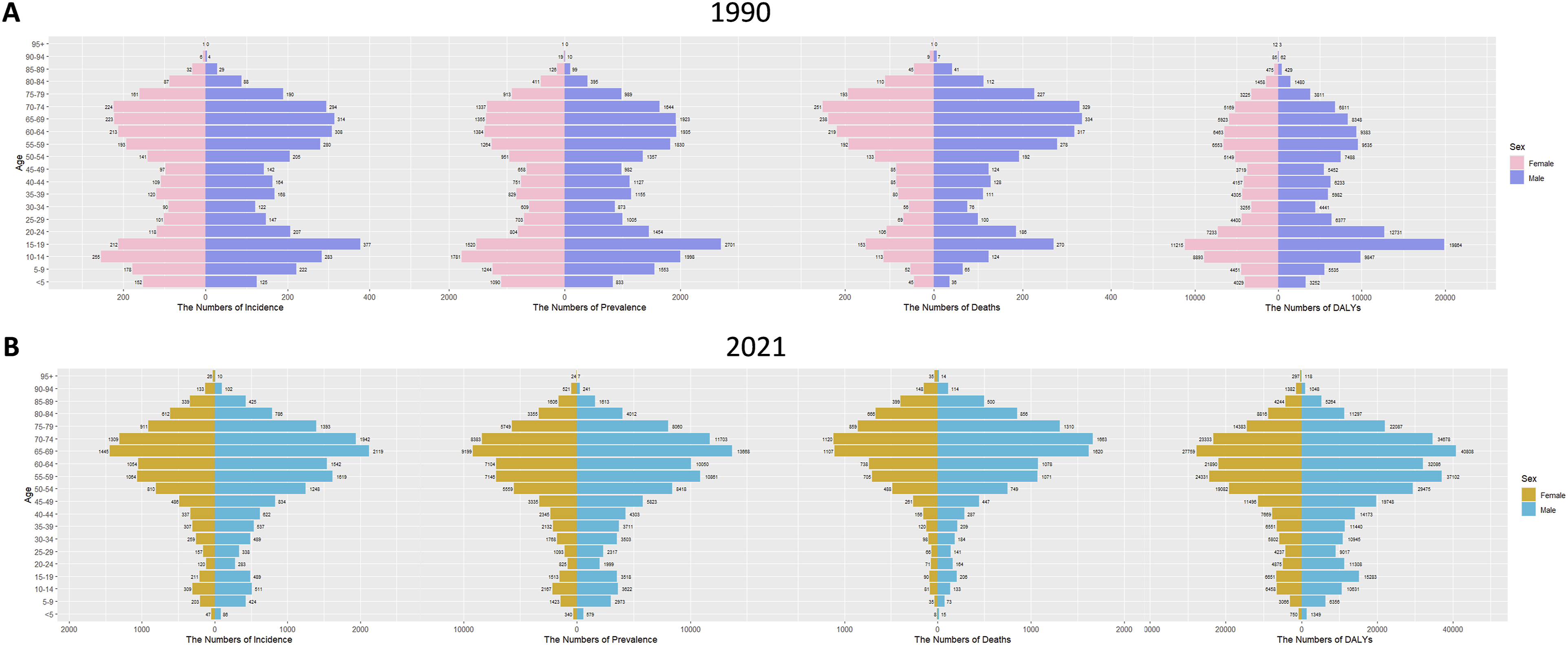
Figure 5 compares the disease burden and ASIR of MNBAC among various age groups for men and women in China from 1990 to 2021. As shown in Figure 5A, the ASIR for MNBAC peaked among women in 2009 and men in 2021, with the most significant disparity between the sexes noted in 2015. The ASPRs for MNBAC in men and women are analogous to the ASIR (Figure 5B), and the trends are in line with global trends (Supplemental Figure 3). Additionally, Figure 5C reveals that in 1990, a significant difference was noted in the number of deaths and ASMR for MNBAC between men and women, with men having a considerably higher ASMR than women. Over the years, the sex difference has progressively increased, with the ASMR increasing until 2015 before beginning to gradually decline. The ASDR for MNBAC follows a pattern akin to the ASMR. Globally, the ASMR and ASDR have remained stable, and the disparities between men and women have been sustained (Figure 5D, Supplemental Figure 3). A comparative analysis of total incidence, age-standardized incidence rate, prevalence, mortality, and DALYs for males and females in China spanning 1990 to 2021. A: incident cases and ASIR; B: prevalent cases and ASPR; C: death cases and ASMR; D: DALYs cases and ASDR. bar charts represent counts; lines represent age-standardized rates
Trends and Forecasts of the Burden of MNBAC in China and Globally
Between 1990 and 2021, a minor and consistent upward trend was noted in the ASIR and ASPR for global MNBAC. In contrast, China’s MNBAC ASIR and ASMR increased significantly, peaking by 2010, after which they stabilized and declined. Since 2002, China’s ASIR has exceeded the global level, and since 2001, its ASPR has also exceeded the global level. Additionally, although the global ASMR remained relatively stable, China’s MNBAC ASMR has been on an upward trajectory since 1990, peaking in 2007 and then dropping significantly; however, it has still been above the global average since the turn of the millennium. From 1990 to 2021, the global ASDR was generally stable despite minor fluctuations, whereas China’s ASDR exhibited a significant ascent before 2005, followed by a sustained decrease, with China’s ASDR exceeding the global level from 2003 to 2015 (Figure 6 and Table S1). A comparison of MNBAC trends and future projections in China and globally. A: ASIR; B: ASPR; C: ASMR; D: ASDR
Forecast of MNBAC in China and globally in the Following l4 years From 2021

UI, uncertainty interval; ASIR, age-standardized incidence rate;ASPR, age-standardized prevalence rate; ASMR, age-standardized mortality rate; ASDR, age-standardized dalys rate.
Discussion
Among bone tumors, malignant ones, such as osteosarcoma, though rare, have high mortality rates. 24 Metastatic bone tumors often lead to the occurrence of skeletal-related events, such as severe pain, pathological fractures, and hypercalcemia, which greatly diminish patients’ quality of life. All these types of bone tumors are public health concerns that warrant our attention.25,26 A previous study assessed the burden of MNBAC from a global and regional macro perspective, potentially neglecting the nuances of specific countries. 10 Given that GBD 2021 integrates over 328 000 data points, a significant increase compared with GBD 2019, and offers more detailed demographic and geographic information, incorporating new data sources such as the latest employment data from the International Labour Organization and data from cancer registries and specialized studies in more countries, we have opted to use GBD 2021 data to comprehensively analyze the current burden of MNBAC globally and in China. 27 Moreover, the study also investigated variations in the age and sex burden of MNBAC in China. Lastly, BAPC was employed to anticipate the future burden of MNBAC. The findings of this study furnish valuable data for health in China and the world, potentially facilitating a reduction in the burden of MNBAC in China and globally.
In this study, the incidence, prevalence, and mortality rates and DALYs of MNBAC in China and globally were comprehensively assessed over the past 30 years based on the GBD 2021 database. Disparities in the MNBAC disease burden between China and the global context were examined by age and sex. The data revealed an ascending trajectory in all burden of MNBAC indicators in China from 1990 to 2021. The incidence, prevalence, and mortality rates and DALYs associated with MNBAC were dependent on age, with 1990 demonstrating peak occurrences in the groups aged 10-19 years and 65-74 years. By 2021, a marked reduction in the aforementioned indicators was noted in the group aged 10-19 years, reflecting the significant role of demographic aging in shaping the burden of MNBAC. In terms of sex-specific analysis, men demonstrated both a higher incidence rate and a more pronounced mortality risk than women.
From 1990 to 2021, China experienced rapid social development, and changes in population structure and lifestyle have had a significant effect on public health, 28 leading to an overall increase in the burden of MNBAC. According to a GBD study, China recorded the highest number of incident cases and deaths from MNBAC globally in 2021. 10 This result is consistent with the findings of the present study that is, from 1990 to 2021, the number of new cases in China rose from 6382 to 25 938, more than tripling. China’s ASIR also increased from 0.65 to 1.42 per 100 000 people, and the AAPC increased by a scale factor of 2.59, indicating the need to accelerate efforts to effectively address the cancer burden. Regarding mortality, compared with the global increase of 15.60%, China’s mortality rate increased by 85.9% from 1990 to 2021. The DALY estimates, in addition to the traditional cancer incidence and mortality metrics, provide a perspective on the loss of healthy life years due to cancer. A 1.43-fold increase was noted in China’s DALYs from 1990 to 2021, with an AAPC increase of 1.26%. A GBD 2019 study indicated that the overall health loss due to cancer is primarily linked to premature death, with cancer being the second-leading cause of global disease and injury-related DALYs. 29 This finding emphasizes the need to strive for better survival outcomes for patients with cancer. This situation may be due to several reasons.
China is currently confronted with the challenge of an increasingly aging population, with the proportion of the older population rising continuously. Meanwhile, the incidence of MNBAC is relatively high among older adults. In comparison with other regions in the world, China’s population is aging at a much faster pace, resulting in a more pronounced upward trend in the number of MNBAC cases. Amidst the rapid economic development, significant changes have taken place in the lifestyle of Chinese people. Their dietary structure has gradually become more Westernized, with a growing intake of high-fat and high-calorie foods, resulting in an increase in the obesity rate. Moreover, modern people’s physical activity has been greatly reduced, and long-term sedentary behavior has become the norm. These unhealthy lifestyle habits may significantly increase the risk of MNBAC development. 30 Globally, the extent of lifestyle changes varied markedly across different regions. Some developed countries realized earlier that lifestyle has a huge effect on health and have taken many good measures. For example, in the United States, a law requires that any food containing >0.5 g of trans fat per serving must be clearly indicated on its label. This regulation aims to protect consumers’ right to information and improve their health. New York City is even more advanced. Since 2007, it has enforced laws to stop restaurants from using artificial butter and vegetable shortening and ban the sale of foods containing trans fat. This legislation has helped in reducing the risk of diseases attributed to trans-fat consumption, which was also a good example for other countries. 31
With rapid industrialization and urbanization, China is facing prominent environmental pollution problems. Air, water, and soil pollutions are particularly severe in some areas and may be associated with MNBAC. 32 Certain occupational groups with long-term exposure to chemical substances, radioactive materials, and other harmful substances have a significantly increased risk of developing diseases. A study reported that long-term exposure to black carbon particles was closely related to bone loss, and people living in areas with high concentrations of PM2.5 have a greater risk of osteoporotic fractures. 33 A Mendelian randomization study confirmed the causal link between chronic PM2.5 exposure and reduced bone density in the lumbar spine and femoral neck. 34 In China, air pollution is especially severe, with large cities and industrial-intensive areas being the most affected. The incidence of lung cancer and other cancer types is significantly higher among people exposed to polluted air for extended periods. Additionally, the release of large amounts of industrial and domestic wastewater has resulted in serious water pollution in many regions. Heavy metals and organic pollutants in water are closely related to cancers such as liver cancer and bladder cancer. A study also reported an increasing incidence of cancer related to water pollution in China. 35 Meanwhile, the excessive use of pesticides and fertilizers, as well as the improper disposal of industrial wastes, has worsened soil pollution. Heavy metals (such as cadmium, arsenic, and lead) and organic pollutants (such as polycyclic aromatic hydrocarbons and pesticide residues) in the soil can enter the human body through crops. Long-term accumulation may increase the risk of cancer. 36 In some agricultural areas, cancer incidence has increased because of soil contamination by chemical substances and heavy metals. 37 In addition, certain occupational groups who are exposed to chemical substances, radioactive materials, and other harmful substances for extended periods have an even higher risk of developing diseases. For example, workers exposed to certain pesticides have a significantly increased risk of non-Hodgkin’s lymphoma, and exposure to harmful chemical substances, such as benzene, is also closely related to the risk of cancer.38,39 Despite certain progress in environmental protection and occupational health in China, a gap remains when compared with developed countries in terms of supervision and protective measures. Soil pollution is severe in some regions, and relevant legislation and remediation measures are still being improved. Occupational exposure supervision and protective measures must be further strengthened in some industries and regions.
In recent years, China has made significant breakthroughs in medical technology, with diagnostic techniques, such as imaging, becoming increasingly widespread and accurate. This has enabled more patients with MNBAC to receive timely diagnoses. In the past, owing to limitations in diagnostic technology, some patients may not have been diagnosed. In contrast, some countries, such as the United States and Germany, have seen an increase in Ewing’s sarcoma research. 40 This reflects that they have achieved relatively mature control in all aspects of bone tumor prevention and treatment; thus, the relative increase in related medical burden is not significant. Despite China’s significant progress in medical technology, compared with high-income countries such as the United States and Japan, some gaps remain in medical resource allocation and tumor treatment levels in some regions. 41
The uneven distribution of medical resources between urban and rural areas, as well as differences in the concept of adjunctive therapy, is a potential factor contributing to the increasing burden of MNBAC in China. Medical resources are highly concentrated and abundant in urban areas, with advanced medical equipment, professional medical staff, and a large number of medical institutions. In contrast, rural areas suffer from a lack of medical resources, with insufficient basic medical facilities and professional medical personnel. Consequently, rural patients face various difficulties in the early diagnosis and treatment of diseases, which can easily lead to delays in the best treatment opportunities. For example, in 2015, the number of registered doctors per 1000 people in urban areas of China was 2.57 more than that in rural areas. 42 Urban residents generally have higher educational attainment, which gives them a stronger ability to acquire and understand health-related knowledge. They are also more receptive to adjunctive therapy and more willing to actively participate in auxiliary treatment programs, such as rehabilitation therapy and psychological counseling, to improve treatment outcomes and quality of life. Conversely, rural residents may lack relevant knowledge and information, so they do not understand the importance of adjunctive therapy. This lack of awareness often results in them seeking such services less frequently, which in turn affects the overall effectiveness of treatment. 43 Lifestyles and living environments in rural areas differ from those in urban areas, and rural residents may face more occupational exposure risks, such as long-term contact with chemical substances, like pesticides and fertilizers. These hazards increase the risk of bone and soft tissue malignant tumors. 44 In addition, the rural living conditions are relatively challenging, and the physical resistance of residents may be relatively low, making it easier for diseases to occur and worsen. 45 As regards access to medical services, rural areas are often far from medical institutions, with inconvenient transportation and high medical costs. As a result, some patients are reluctant or unable to go to the hospital in the early stages of illness. Even if they have medical insurance, the reimbursement ratio and scope may not be the same as in urban areas. Thus, rural patients face greater economic pressure, which in turn affects the continuity and completeness of their treatment. In developed countries like Japan, the distribution of medical resources is relatively balanced. The government ensures the fair allocation of medical resources through policies, with slight differences in medical standards between large cities and rural areas. Japan’s medical insurance system has a wide coverage, and nearly all citizens can enjoy high-quality medical services. 46
In this study, the joinpoint regression analysis detected a descending trend in China’s burden of MNBAC post-2007, with more pronounced declines in ASMR and ASDR. The APC for ASMR was −1.75 from 2007 to 2021. For ASDR, the APC was −2.43 from 2008 to 2013 and −1.52 from 2013 to 2021. Since 2007, China’s significant progress in medical insurance and healthcare services has helped reduce the burden of MNBAC. In terms of medical insurance, coverage has expanded rapidly from 13.4% in 2003 to 94.6% in 2023, reaching 92.4% by 2009. This expansion has offered robust financial support for patients, allowing more individuals to receive timely medical care. 47 For cancer prevention and control, China initiated multiple cancer screening and early diagnosis and treatment programs after 2007, including the Huai River Basin project. These efforts have improved the early detection rate of cancer and increased public awareness of prevention and treatment, thereby supporting the early intervention of MNBAC. 48 Regarding healthcare service improvement, hospital evaluations shifted to focus on medical quality and safety in 2005, paying attention to “medical quality” and “satisfaction indicators.” A comprehensive assessment system covering medical quality, safety, and operational management has enhanced the diagnostic and treatment capabilities of medical institutions and provided higher-quality medical services for patients. In conclusion, these policies and measures have collectively mitigated the burden of MNBAC. 49
This study indicates that the burden of MNBAC tends to increase significantly with age, although it remains considerably lower than that of older individuals. Moreover, a small peak was noted in the group aged 15-19 years, akin to the epidemiology of osteosarcoma, which exhibits a bimodal age distribution, with the second peak occurring in older adults.50,51 Globally, the peak in the group aged 15-19 years is even more pronounced, indicating that as China undergoes rapid population aging, the number of older patients is steadily increasing, highlighting the need for special attention to the burden on this demographic.
Furthermore, the burden of MNBAC was examined among patients of different sexes. Men exhibited significantly higher incidence, prevalence, and mortality rates and DALYs than women, which is associated with men’s higher attributable cancer burden. Several major risk factors for cancer contribute to this disparity, such as smoking, with 62% of smokers being male and 38% female. 52 Moreover, obesity, which is encountered in 5.5%–20% of patients with cancer, is more prevalent in men. 53 Another factor that is closely linked to obesity is inflammation. 54 Chronic inflammation is also recognized as a risk factor for cancer, 55 and because of genetics, age, and environmental factors, cancer is more common in men than in women. 56 Thus, sex-targeted strategies in cancer prevention and treatment must be employed to address the higher burden among men.
BAPC projection revealed that from 2022 to 2035, the burden of MNBAC in China and globally is expected to decline. Although the current burden of MNBAC in China is higher than the global average, it is anticipated to drop significantly in the coming years. This finding is largely credited to the initiatives on cancer prevention and management at the global and Chinese levels: (1) the implementation of population-based cancer screening initiatives, with the Chinese government initiating targeted cancer screenings in high-risk populations since 2006, which has the potential for a nationwide expansion in the near future 57 ; (2) the ongoing enhancement of healthcare accessibility and availability in China 58 ; (3) adoption of new anticancer drugs and treatment strategies in our China59,60; and (4) increasing awareness about healthy living habits through educational initiatives, which is also an effective approach to cancer prevention. 61
However, this study has some limitations. First, the availability and completeness of the GBD data may be insufficient, as these data are derived from mathematical models, particularly in low-income countries, which leads to differences in the accuracy of the estimates. Second, the low incidence of MNBAC did not allow further classifying specific tumors. Lastly, given the extensive geographical range of China and the potential for significant variations in disease burden among provinces, the burden of MNBAC mortality in individual provinces was not evaluated.
Conclusions
From 1990 to 2021, China demonstrated a significant increase in the relative burden of MNBAC, particularly among the older population who exhibited peak incidence and higher mortality rates. In this study, men were more susceptible to MNBAC and had a higher risk of death. Future projections reveal a steady decline in the burden of MNBAC, hinting at the efficacy of current health strategies. Nevertheless, the aging Chinese population signifies that MNBAC will continue to be a formidable public health issue.
Supplemental Material
Supplemental material - Trends, Global Comparisons, and Projections of the Burden of Malignant Neoplasm of Bone and Articular Cartilage in China Based on GBD 2021
Supplemental material for Trends, Global Comparisons, and Projections of the Burden of Malignant Neoplasm of Bone and Articular Cartilage in China Based on GBD 2021 by Baodong Wang, Jiling Zhang, Congying Zou, Tianyi Wang and Lei Zang in Cancer Control.
Supplemental Material
Supplemental material - Trends, Global Comparisons, and Projections of the Burden of Malignant Neoplasm of Bone and Articular Cartilage in China Based on GBD 2021
Supplemental material for Trends, Global Comparisons, and Projections of the Burden of Malignant Neoplasm of Bone and Articular Cartilage in China Based on GBD 2021 by Baodong Wang, Jiling Zhang, Congying Zou, Tianyi Wang and Lei Zang in Cancer Control.
Footnotes
Acknowledgments
The authors wish to thank the GBD study for sharing the data.
Ethical Considerations
Not applicable. This study complied with the GATHER guidelines. The data analyzed were aggregated, ensuring that no information about individual patients or public personnel was directly implicated.
Author Contributions
JZ: Formal analysis, Software, Writing–original draft. BW: Formal analysis, and Writing–review & editing. CZ: Formal analysis and Writing–review & editing. TW: Data curation and Writing–review & editing. LZ: Conceptualization, Methodology, Supervision, and Writing–review & editing. All authors approved the final version of the manuscript. The corresponding authors attest that all listed authors meet authorship criteria and that no others who meet these criteria have been omitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.