
Abstract
Introduction
The aim of this study was to assess the effectiveness of visual-based education intervention on understanding cancer information.
Methods
We conducted a systematic review across PubMed, Embase and Scopus electronic databases using Preferred Reporting Items for Systematic Reviews and Meta-analysis, in July 2025. Randomized and non-randomized studies measuring impact of visual-based education interventions on health literacy, knowledge, comprehension, or understanding in cancer were considered for inclusion. Quality assessment was conducted using the Mixed Methods Appraisal Tool (MMAT). A descriptive analysis of included studies was performed, and a meta-analysis was performed for Randomised clinical trials (RCTs).
Results
Twenty-one studies were included in the review, 11 RCTs, seven non-RCTs, and three mixed methods design. The studies were conducted in seven countries across five continents. A high proportion of the included studies satisfied the MMAT quality assessment criteria. Visual-based interventions improved knowledge and comprehension compared to non-visual communication such as audio or basic text. In one study, video intervention increased knowledge with mean difference 3.96 ± 1.69 compared to pamphlet (1.76 ± 1.42). Crowd-figure-pictograms with numeric data increased knowledge by 2.42 compared to non-numeric controls (0.20). Furthermore, 3D printed models improved understanding compared to imaging alone (4.60-4.78/5 vs. 4.06-4.49/5), and visual-based treatment timelines improved comprehension compared to audio (0.84 vs 0.68). However, certain visual-based interventions had no impact over well-designed static materials in some contexts. Health literacy was a significant moderator of outcomes, and low health literacy was consistently associated with poor baseline knowledge and comprehension, regardless of visualization format.
Conclusion
Visual-based education interventions may improve knowledge, comprehension and understanding, overcoming barriers imposed by limited health literacy, hence empowering patients to self-manage their health across various cancer contexts.
Introduction
Understanding and addressing modifiable risk factors of cancer through prevention, early detection and effective management can reduce its impact. 1 Decision making for personal health necessitates more than just the provision of information by healthcare professionals. It also requires tailored information to the individual patient’s level of comprehension, ensuring that communication is accessible and actionable. 2 In high burden diseases like cancer, patients with limited health literacy have more difficulty in navigating the health care system and making informed decisions3,4 when compared to diseases with burden. Understanding health information during cancer enables individuals with lower health literacy to play an active role in improving their own health.2,5 As most cancer services are delivered through outpatient clinics, 6 supporting the person affected with cancer requires innovative ways to enable them access and understand information.7,8
Health literacy is defined as the degree to which individuals can obtain, process, understand, and communicate health-related information needed to make informed health decisions.5,9 It is a multifaceted concept that has evolved from a narrow focus on basic reading and numeracy to focus on individual skills that encompass a dynamic interaction between an individual and the demands of health systems and society.10-12 It concerns the knowledge and competences of individuals to meet the complexes of health, including understanding the factors that influence health and knowledge of how to address these factors. 11 Health literacy is linked to literacy and extends beyond basic reading and numeracy to include a broad set of skills encompassing knowledge, comprehension, self-care, communication skills, accessing, appraising and applying health information.11,13
Studies have shown that low health literacy is linked to poor health outcomes including lower implementation of preventative health and lower treatment adherence.4,14 Individuals with limited health literacy often struggle with navigating the health care environment, including accessing care across the cancer continuum resulting into errors, poor quality of care, and risks to patient safety.15,16 Attributing factors include reliance on written materials to communicate health information, such as doctors’ instructions, preventative guidance for healthy lifestyle choices, and medication dosage directions.4,17 With an estimated 750 million adults globally living with low literacy 18 both low literacy and limited health literacy present significant barriers for health professionals in delivering effective care. 17
Improving the understanding of health information through various educational interventions have been proven an effective way to increase a person’s ability to self-manage their health.19-21 A recent review found that visually enhanced education materials improve comprehension compared to traditional methods of oral or written material.15,22 Visual-based interventions are defined by the Centers for Disease Control and Prevention as images, videos, and similar tools used to communicate information about a specific topic and to simplify the comprehension process.15,23 Visualising health information through graphics, images, and videos enhances the communication of complex concepts, supports consumer understanding and contributes to improved patient safety and outcomes. 24 The effectiveness of visual-based interventions may be due to increased interactivity and reduced reading efforts.15,25
While systematic reviews3,15,16 have assessed the effect of various interventions on health literacy, none of the reviews specifically assessed the effects of visual-based education interventions on health literacy in cancer. A review by Housten et al. 16 revealed that education, communication, technology and multimodal strategies are commonly employed in cancer improving screening and comprehension. Galmari et al (2024) assessed the effectiveness of various visual-based interventions on health literacy in healthcare included eight cancer-based studies but did not comprehensively analyse for the impact of visual interventions in cancer. 15
A recent umbrella review by Jetaini et al (2025) that included 10 systematic reviews of cancer education confirmed that health literacy interventions targeting patient education and communication are the most common. 3 Similar to findings by Housten et al (2021), multimodal interventions showed positive effect in improving health literacy. 3 Among the included reviews, none primarily assessed the effect of visual-based education interventions on health literacy in cancer patients. 3
Building on these reviews, the present review aims to assess the effectiveness of visual-based education intervention on improving understanding of cancer.
Methods
The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statement (Supplementary File 1). 26
Search Strategy
An electronic search via title and abstract was conducted in PubMed, Embase and Scopus from database inception to 27th July 2025. The search terms included ‘visual intervention OR visual education’ AND ‘health literacy OR understanding’ AND ‘cancer OR oncology’, with additional relevant keywords expanded using the Boolean Operator OR. The search strategy is attached as Supplementary File 2.
Eligibility Criteria
Eligibility Criteria

Exclusion criteria: Studies that were not focused on cancer as the study area, as well as those that did not include any intervention or the outcome of interest. Additionally, studies with inappropriate designs such as abstracts, reviews, qualitative studies, cross-sectional studies, letters to the editor, commentaries, reports, and unpublished articles were excluded. Non-English studies and those without accessible full texts were also excluded from the review.
Outcomes of Interest
In this review, the outcomes of focus included health literacy measured as health literacy, knowledge, comprehension, or understanding. Measuring health literacy directly may be challenging due to its multidimensional nature leading to reliance on proximal outcomes such as knowledge, comprehension and understanding often measured through study-specific validated questionnaires.3,15 Knowledge, comprehension, and understanding are fundamental measures of health literacy11,16,27 justified by the definition of health literacy as the capacity to obtain, process, and understand basic health information11,28 and their status as confirmed measurable outcomes in intervention research.3,15,16 Considering the concerns from previous studies to the lack of standardised measures and tools in reporting the outcomes,3,15,16 the findings and tools of measurement are presented as reported in the included studies.
Selection Process
The results of the electronic search were imported to endnote 29 where duplicates were removed. The studies were then transferred to Covidence 30 for screening. After removal of duplicates identified by Covidence, screening of titles and abstract was done by one author, L.S. A hand search of the reference lists of included studies was also conducted to identify additional eligible studies. The full texts evaluation was conducted by two authors, EC and LS, and conflicts were resolved through discussion.
Data Extraction and Analysis
The data extracted from included studies were author’s name, year of publication, country, study setting/population, study design, aim of study, intervention employed, and outcomes reported. Data extraction was done using a standard data extraction form in excel. Descriptive analysis was used to summarize study findings. Additionally, meta-analysis of randomised clinical trials (RCTs) was conducted in Review Manager 5.4. 31
Quality Assessment
Quality assessment of studies was conducted by two researchers (LS and EC) by referring to the Mixed Method Appraisal Tool (MMAT). 32 Each study was assessed using the MMAT criteria based on its methodological design. For each criterion, a score of 1 was applied if yes, 0 if no or unclear, and 1 if the criteria did not apply to the study. The score for each study was determined by calculating the number of yes responses out of the total number of applicable criteria. While we calculated the average score for all studies, we endeavoured to provide a more detailed presentation of the ratings of each criterion to inform the quality of the included studies better as recommended. 32
Results
Characteristics of Included Studies
The systematic review included published studies of visual-based interventions in cancer. A total of 1298 studies were retrieved from search of electronic databases and four from reference searches. After removal of duplicates and generic references, 954 studies were considered for title and abstract screening, of which 85 studies were eligible for full-text screening. Finally, 21 studies were included in the final analysis (Figure 1). Prisma flow diagram
Summary of the 21 Included Studies in a Systematic Review

Outcomes Measured
General outcomes measured in the studies varied across studies but mainly included cognitive, affective and behavioural domains, see Table 2.
Fifteen of the included studies assessed knowledge as an outcome, five measured comprehension, and one evaluated understanding. The areas of focus were screening, treatments, anatomical understanding, medical terminology and risk information in cancer. The studies employed different validated questionnaires to assess outcomes and only two studies primarily used a validated health literacy tool.42,53
Other outcomes considered included affective aspects including anxiety, worry, and decisional conflict, and behavioural domains such as screening or treatment intentions, role preferences, hypothetical decisions and choices for care levels. Self-efficacy and confidence in decision making and information use was another aspect frequently measured, see Table 2.
Quality Assessment
The RCT studies met most of the MMAT quality criteria for RCTs. The most frequent reported limitation was lack of blinding in at least eight of the 11 RCTs36,43,44,46,47,49-51 and followed by lack of complete outcomes in three studies.44,49,50 Wake et al, (2019) scored the least in terms of MMAT quality due to lack of data on how randomization was performed, comparability of groups and it was also unclear whether blinding was performed. 50 The lack of blinding for researchers or assistants may have introduced bias by influencing subjective outcomes reporting, and participants may have provided socially desirable responses. Additionally, unblinded research assistants involved in data collection may have unintentionally given more guidance or support to the intervention group, potentially affecting the validity of the results.32,54 The quantitative non-RCTs also met most quality criteria, particularly concerning clear objectives and appropriate measurement tools, but showed a significant lack of accounting for confounders. The three mixed methods studies met all the MMAT quality criteria for mixed method studies. Supplementary File 3 presents the results of the quality assessment of the included studies conducted using MMAT.
Visual-Based Education Interventions Employed
Visual-based education interventions employed across studies included digital and audiovisual formats, such as video decision aids, interactive multimedia, tailored computer programs, web-based tailored information, and virtual reality educational interventions.33-36,38,41,43,46,48,49,52,53 Static print materials with visual components included informational brochures, pamphlets, illustrated flip charts, and paper-based decision aids with graphics and color-coded cards.40,51 Graphic designs and models included pictogram-based timelines, comics, photos, bar graphs, icon arrays, patient-reported outcome visualizations and 3D/augmented reality models.37,39,44,45,47
Impact of Visual-Based Education Intervention on Knowledge
Impact of Visual Interventions on Outcomes

Conversely, the non-RCTs consistently reported clear knowledge benefits: video decision aids improved cancer screening knowledge for ethnically diverse patients compared to brochures 34 and significantly increased advanced cancer goals-of-care knowledge post-intervention. 48 Furthermore, quasi-experimental designs indicated that videos significantly improved cervical cancer knowledge in mass screening participants in Tanzania. 33 Audio-visual sessions increased knowledge among rural Indian women 42 and increased cervical cancer literacy in Arabic-speaking women. 53 Also, a targeted decision aid utilizing graphics increased knowledge about colorectal cancer screening in older adults. 40
Mixed methods studies with a randomised controlled intervention component, including one comparing video, internet, and written materials 38 and another comparing animated vs. static pictographs, 37 found no statistically significant difference in knowledge scores between visual and non-visual presentations. Nguyen et a al 2024 a RCTs, found that intervention mode tailoring did not significantly increase knowledge before consultation, although higher pre-consultation knowledge predicted better information recall. 43 In another study, although an educational flip chart intervention found no significant difference between groups, it enhanced objective and subjective knowledge for African American patients undergoing breast biopsy. 51
Meta-Analysis Results
A meta-analysis was conducted for the RCT studies that provided relevant quantitative data on knowledge outcomes. Gao J (2022) 35 study labelled the outcome as comprehension, the authors stated that the tool used in the comprehension section specifically measured patient’s knowledge of radiotherapy, providing the quantitative data required for inclusion in the meta-analysis. For studies that did not report within-group mean ± SD differences, the mean change was calculated as the difference between post- and pre-intervention scores. The standard deviation of the mean change was then derived using the formula:
SD = √(SD2pre + SD2post - 2r × SDpre × SDpost), where the correlation coefficient (r) between pre- and post-intervention scores was assumed to be 0.5.
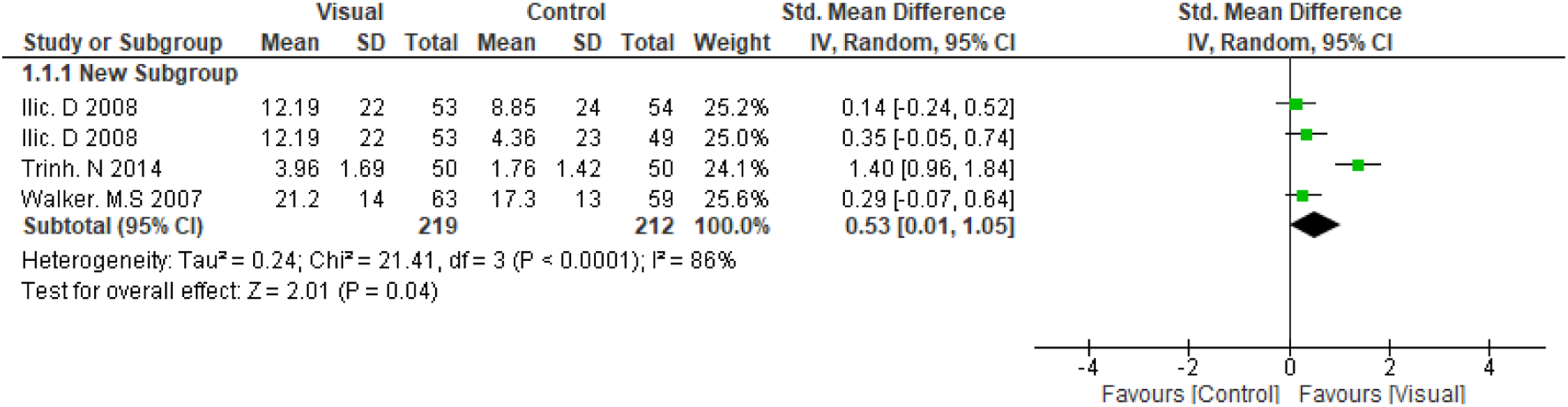
The overall pooled effect estimate was 0.98 (95 % CI: 0.22, 1.74), see Figure 2, indicating a statistically significant increase in knowledge in favour of visual-based education. However, there was substantial heterogeneity across the included studies (I2 = 94%). A subgroup analysis was performed by excluding the study by,
35
in which the intervention involved 3D virtual reality simulation, a more interactive and potentially more impactful intervention compared with conventional visual-based educational intervention used in the other studies. The resulting pooled estimate was 0.53 (95% CI: 0.01, 1.05), see Figure 3, showing that visual interventions continued to have a positive effect on knowledge, although the confidence interval crossed the line of no effect and heterogeneity remained high (I2 = 86%). A further subgroup analysis, limited to the two studies that reported within-group mean differences, yielded a pooled estimate of 2.17 (95% CI: 0.60, 3.75), I2 = 92%, see Figure 4. Subgroup analyses by cancer type, educational tool, or intervention duration could not be performed due to the small number and diversity of the included studies. The four included studies varied widely in cancer type, tool used, and exposure time, making it difficult to identify specific sources of heterogeneity or conduct reliable statistical comparisons. Meta-analysis for RCTs Subgroup analysis of conventional visual-based education interventions Sub-group analysis of the two studies that reported within group mean difference and SD

Impact of Visual-Based Education Intervention on Comprehension and Understanding
Studies that assessed the impact of interventions on comprehension show mixed results across study designs: RCTs demonstrated that visual-based treatment timelines significantly improved participant correct responses compared to audio-only information, 39 and a Virtual Reality system significantly increased radiotherapy comprehension scores compared to standard care. 35 Another RCT comparing visual formats (bar graphs, icon arrays) to a well-designed numerical text block found no enhancement in gist or verbatim comprehension regarding breast cancer survival rates. 47 Non-RCT studies consistently reported positive impacts, as a video-based tool significantly improved comprehension of prostate health terms by 68%. 52 In another non-RCT that studied longitudinal patient-reported outcome prototypes, Meter (visual analogy of size or time) achieved the best gist comprehension and Emoji had the highest verbatim comprehension, whereas Comic had the poorest comprehension. 45
One study evaluated the impact of intervention on understanding and findings showed that 3D printed models increased patient understanding of their anatomy, disease, tumour characteristics, and surgical procedure compared to imaging alone. 50
Association Between Baseline Health Literacy and Outcomes
Association Between Baseline Health Literacy and Outcomes

Health literacy was categorised as low/inadequate or high/adequate literacy levels.37,40,47,52 The association between health literacy and outcomes showed varied results regarding intervention effectiveness: an entertainment-based decision aid, inferred to be targeted at a low literacy site led to lower decisional conflict and greater self-advocacy for prostate cancer screening compared to a control audio booklet in that group, whereas no such difference was found at the high literacy site. 49 In Volk et al. 49 literacy was inferred from clinic location rather than measured for each patient, as some patients at the low-literacy clinic may actually have had high literacy, and vice versa, which may have affected the results. Differences in patient characteristics, such as education, income, and insurance, could also have influenced the findings A video-based educational tool improved patient comprehension of prostate health terminology effectively regardless of literacy level 52 and video education enhanced cervical cancer knowledge independent of literacy, although reading ability was a statistically significant factor in the magnitude of score change in multivariate analysis. 33 For visualization of patient-reported outcomes among a population with predominantly limited literacy, optimized graphics like the Meter and Emoji prototypes had better outcomes for comprehension. 45 However, comparisons involving formats for communicating complex data often found no significant differences in comprehension improvement across visual and well-designed numerical textual formats for survival, despite the lack of format advantage, baseline health literacy remained critical, as higher health literacy was associated with higher gist comprehension of survival information 47 and those with adequate literacy were more likely to be prepared for individualized decision-making than those with inadequate literacy regarding colorectal cancer screening. 40 Conversely, interventions designed to increase knowledge successfully resulted in a statistically significant increase in overall health literacy scores, especially in awareness, prevention and control domains. 53
Discussion
This systematic review studied the effectiveness of visual-based education interventions on understanding cancer education focusing on knowledge, comprehension and understanding of the information. Visual-based interventions presented in various formats were used across different cancer types, including prostate cancer,34,36,38,45,49,52 colorectal cancer screening,37,40,41 breast cancer screening, biopsy consent and adjuvant therapy decisions,44,47,51 and cervical cancer screening and human papillomavirus education33,42,53 alongside interventions for advanced cancer goals of care. 48 The target populations were often characterized by vulnerability, including low-literacy patients and ethnically diverse groups (African American, Latino, Arabic-speaking immigrants), as well as the elderly making individualized screening decisions.34,40,49,51-53 Intervention components ranged from basic formats like illustrated flip charts and pictogram enhanced print materials to complex multi-modal digital tools such as video decision aids, interactive mode-tailored websites, and virtual models like 3D printed anatomy models and virtual reality simulators.34,44,51
The findings revealed that structured educational videos and multimedia platforms enhanced understanding of complex medical concepts and terminology of cancer prevention and treatment compared to traditional brochures, thereby supporting informed decision-making.34,48,49 For instance, a video-based educational intervention significantly improved baseline knowledge of human papilloma virus and cervical cancer among women in Tanzania, independent of their existing education or literacy level. 33 Similarly, patients with advanced cancer demonstrated significantly improved knowledge scores after viewing an educational video on goals of care and in a study comparing video versus pamphlets for skin cancer education, the video group showed a significantly greater improvement in knowledge scores.46,48 In studies that employed specific visual aids, such as pictogram-based treatment timelines or crowd-figure-pictograms to illustrate population risk, effectively conveyed numeric leading to improved gist and verbatim comprehens 51 ion and recall.39,44,45 The focus on visualization addresses the limitations of low numeracy and reading literacy, leading to higher reported confidence and satisfaction especially in awareness, prevention and control domains.45,49,53 Although visual formats generally enhanced engagement and clarity, the effectiveness of visual aids over well-designed, structured text remains context-dependent, with some studies finding equally effective or even higher knowledge gains using comprehensive written materials for certain screening information.36,38,47 Text-based handouts can seem to perform better than video-based when they use clear structure, evidence-based content, plain language, and decision-support exercises.39,44,46,47 Conversely, visual tools sometimes fail to provide added benefits due to shallow information processing, content redundancy, or being perceived as inappropriate for serious medical topics.36,43,49 Additionally, the topic may have been relatively simple for the participants with high baseline knowledge creating a ceiling effect that limited further improvement.51,52 Ultimately, integrating visuals improves information readability, empowering patients in shared decision-making processes by making complex information more easily processed and retained.39,48
Previous systematic reviews have shown consistent benefits of visual-based education interventions on knowledge and comprehension,3,15,16,55 particularly focused for people with lower baseline health literacy or numeracy.15,56 Visualised information shows promising improvements on understanding of complex risk information and treatment goals for decision making. 56 Interventions designed to enhance understanding across varying health literacy levels can improve illness comprehension and promote more appropriate behaviours, including participation in cancer screenings, adherence to complex therapies, engagement in treatment, and effective self-management of everyday health. 3 Visual-based education interventions are beginning to become a focused strategy to communicate complex cancer information to patients, caregivers and the public. Visualised education represents a compelling method for improving patient knowledge and comprehension, critical components of health literacy, especially among populations facing educational or linguistic barriers.3,15,33,52,55
As noted in previous studies,3,10,57 health literacy was defined variably across studies, typically emphasizing the ability to access, understand, and use health information.47,53 For instance, one conceptualization views health literacy broadly, including reading, writing, numeracy, speech comprehension, and conceptual knowledge, 49 while another defines personal health literacy as the ability to find, understand, and use information to inform health-related decisions. 53 The focus in several studies is on the individual’s ability to understand and interpret abstract health information. 47 Health literacy was measured using diverse tools: The Short Test of Functional Health Literacy in Adults and the Brief Health Literacy Screener were used to categorize literacy levels,37,43 while the Rapid Estimate of Adult Literacy in Medicine measured patient reading levels. 52 Furthermore, self-reported measures like the Set of Brief Screening Questions were employed to assess the frequency of difficulty understanding written medical information. 47
Health literacy was a significant moderator of intervention outcomes, low health literacy was consistently associated with worse baseline knowledge and gist comprehension of concepts like survival rates, regardless of visualization format.45,47,52 Multimedia interventions tailored to low-literacy audiences can mitigate these disparities, leading to improvements in comprehension and increased self-advocacy.49,58 In one case, women with lower health literacy felt better informed than high-health literacy women when provided with visualized probability information without accompanying descriptions, demonstrating complex interaction effects on subjective measures. 47
Limitations
The review is not without limitations, firstly although a meta-analysis was conducted, substantial heterogeneity persisted across the included studies and could not be fully explained, despite efforts to explore potential sources through subgroup analyses. As a result, the findings should be interpreted with caution and underscore the need for further investigation. While the MMAT quality assessment indicated that the included studies were generally of good quality, most RCTs lacked assessor blinding, potentially introducing bias and affecting the validity of outcome assessments. Furthermore, there was an inadequate adjustment for confounding variables, which is essential to identify factors that may influence the observed effects of the intervention in non-RCTs. Additionally, the methodology for health literacy measurement is inconsistent, limiting direct cross-study comparisons of health literacy findings. However, studies demonstrated that knowledge, comprehension, and understanding are essential components of health literacy as measured by outcomes directly related to processing and interpreting health information. Although health literacy was rarely the primary outcome, its measurement using diverse tools like Short Test of Functional Health Literacy in Adults, Rapid Estimate of Adult Literacy in Medicine and Single Item Literacy Screener allowed researchers to assess its crucial role as a moderator, revealing that low health literacy is consistently associated with lower comprehension and knowledge. Consequently, success in improving patient knowledge and comprehension through visual education is seen as a direct way to mitigate the barriers imposed by limited health literacy, enabling more informed decision-making across various cancer contexts.
Conclusion
Overall, the findings of this review support the concept that visual-based education enhances knowledge, understanding, and comprehension of cancer prevention and treatment, particularly in relation to health literacy. This, in turn, empowers individuals to access and interpret health information more effectively, facilitates informed decision-making, and improves their ability to navigate the healthcare system.
Supplemental Material
Supplemental Material - Effectiveness of Visual-Based Interventions on Understanding Cancer Information: A Systematic Review
Supplemental Material for Effectiveness of Visual-Based Interventions on Understanding Cancer Information: A Systematic Review by Linda Siachalinga, Hansoo Kim, Karin Brochstedt Dieperink, and Elisabeth Coyne in Cancer Control.
Supplemental Material
Supplemental Material - Effectiveness of Visual-Based Interventions on Understanding Cancer Information: A Systematic Review
Supplemental Material for Effectiveness of Visual-Based Interventions on Understanding Cancer Information: A Systematic Review by Linda Siachalinga, Hansoo Kim, Karin Brochstedt Dieperink, and Elisabeth Coyne in Cancer Control.
Supplemental Material
Supplemental Material - Effectiveness of Visual-Based Interventions on Understanding Cancer Information: A Systematic Review
Supplemental Material for Effectiveness of Visual-Based Interventions on Understanding Cancer Information: A Systematic Review by Linda Siachalinga, Hansoo Kim, Karin Brochstedt Dieperink, and Elisabeth Coyne in Cancer Control.
Footnotes
Ethical Considerations
Ethics approval was not required for this study as it is a systematic review of previously published literature.
Author Contributions
All authors have contributed equally to the development and preparation of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.