
Abstract
Introduction
Cancer Health literacy (CHL) is the health literacy related to cancer knowledge, prevention, treatment, screening, and access to services. It is an important indicator of people’s adherence to screening and preventive measures, which helps to reduce the incidence and prevalence of cancer. The study assessed the CHL level and its association with relevant socio-demographic characteristics and sources of information among primary health care patients and visitors in the United Arab Emirates (UAE).
Methods
A cross-sectional study recruited survey participants who consented to respond to an interviewer-administered questionnaire. The assessment of CHL was done by using 15 questions. CHL level was measured as a median score and also categorized as poor/inadequate, moderate, good/excellent. Nominal logistic regression was used to analyze the relationship between CHL categories and participants’ sociodemographic characteristics and CHL sources of information.
Results
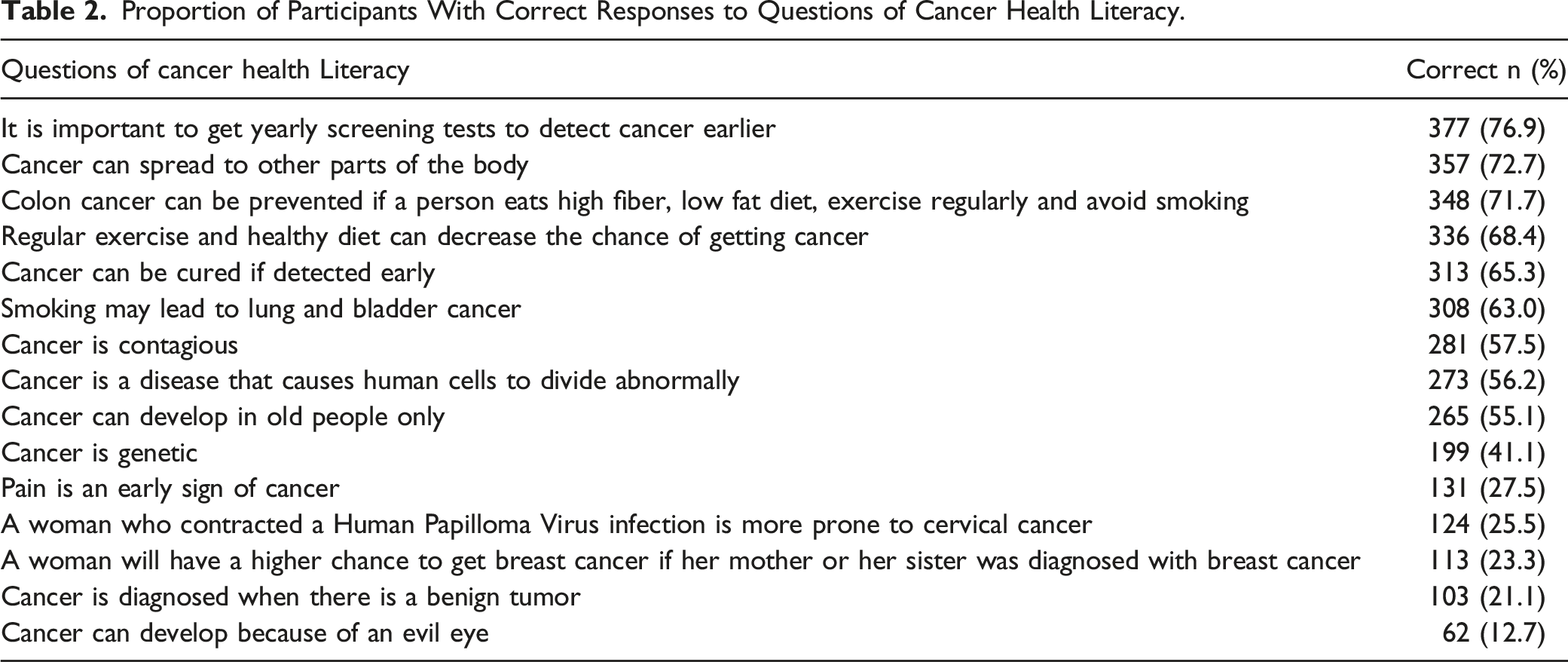
Of the total 492 participants, 45.5% were young adults (30-39 years old), 32.9% were males, and 70.8% were UAE nationals. The overall median CHL score was 8.0 (IQR = 5.0-10). 33.7% of the participants had a poor/inadequate level of CHL, 49.6% had a moderate level and 16.7% had a good to excellent level of CHL. 76.9% of the participants knew the importance of early cancer screening tests, 72.7% acknowledged the metastatic capacity of cancer, and the protective factors of cancer, especially, in colon cancer (71.7%). A high proportion of participants received health information about cancer via the internet (50.7%), television (45.3%), social media (40.2%), and doctors (43.6%). Nationality other than UAE (aOR = 1.62, 95% CI = 1.03-2.56, P = .038), having university education (aOR = 2.20, 95% CI = 1.21-3.99, P = .010) compared to those with lower than high school, and having a family history of cancer (aOR = 2.42, 95% CI = 1.33-4.41, P = .004) were positively associated with CHL. Older age (aOR = .36, 95% CI = .17-.75, P = .007 for 50-59 years, and aOR = .29, 95% CI = .11-.82, P = .019) for 60-69 years, higher-income (aOR = .57, 95% CI = .33-.99, P = .047 for 10,000-19,999 AED; aOR = .53, 95% CI = .33-.88, P = .013 for ≥20,000) compared with those earning <10,000 AED were negatively associated with CHL.
Conclusions
CHL among the resident UAE population was moderately adequate, therefore implementation of awareness campaigns seems to be warranted. Moreover, evaluation research targeting the CHL impact on cancer prevention practices and screening is also advocated.
Introduction
Health Literacy (HL) refers to an individual’s ability to obtain, process, and understand health information and services needed to make informed health decisions It encompasses communication with healthcare providers, social support, and self-management behaviors. Limited health literacy has been linked to more hospital visits, poor prognosis, complications, and recurrence of certain conditions.1,2 These conceptual dimensions extend beyond basic reading skills to englobe communication with health-care professionals, social encouragement, and self-management behaviors.3,4 It has been well-established that patients with a limited health literacy tend to have more hospital visits and stays as well as poor prognosis, complications, and recurrence of certain conditions.4-8
HL is very important for patients with chronic diseases including cancer due to the long-term treatment plans, complex therapeutic regimens, and the emotional burden arising from their conditions. 9 Research has shown that understanding of the disease, treatment plans, prognosis and management of complications have positive outcomes on cancer treatment and recuperation. 9 Some studies have pointed out that limitations in Cancer Health Literacy (CHL) may influence people’s awareness and knowledge of cancer-related health services, adherence to screening, and preventive measures that will help to reduce the incidence and prevalence of cancer.10,11 Recently, researchers in Europe are calling for a European Union framework on cancer literacy and that it should be adopted as a priority by policy makers. 12 Overall, individuals with limited health or cancer health literacy have less knowledge of their disease, which may affect their management and outcomes when compared to those with adequate health literacy.5,13
Furthermore, patients with limited CHL suffer from poor treatment compliance and knowledge of manifestations of cancer, negatively influencing their stage at diagnosis. In addition, poor cancer knowledge and literacy will reduce conversation and consultation about risks and advances of treatment preferences, and subject understanding of informed consent for the planned treatment protocol.14,15 A study conducted on factors affecting health literacy reported that finding and seeking health-related information is 1 important factor contributing to health literacy. 15 While cancer patients are advised to actively participate in their healthcare decisions, for better customized treatment to their specific needs, limited CHL may pose a barrier to screening and patient engagement.16,17
In the Arab world, cancer literacy is not well explored by researchers, and the few available studies indicated poor cancer literacy in the region. 18
There is an emerging need for research to assess CHL in the Arab world, particularly the UAE, with more calls from authorities to improve screening practices and screening awareness. 19 According to Silberman et al. there is an overall health literacy and CHL improvement in Arab countries, including the UAE. 20 In the UAE, there are mainly 3 cancer screening programs (Breast, Cervical and Colorectal) adopted by the Department of Health and the Ministry of Health and Prevention (MOHAP) Human Papilloma Virus vaccination (HPVV), the program was launched by the Department of Health in the year 2012 in Abu Dhabi Emirate for school girls. The MOHAP launched its official (HPVV) vaccination program in the year 2018. 19
Worldwide, the number of studies that have investigated CHL is increasing with the emergence of few in the overall Arab region. In the UAE, the burden of cancer has increased and continues to be a major health problem with significant morbidity, mortality, reduced quality of life, and healthcare costs.21,22 Cancer is currently ranked as the second leading cause of non-communicable disease associated mortality in the country.22,23 Although CHL could have an important role in mitigating this burden, there is no systematic evaluation of the level of CHL and the reasons and factors that may influence CHL in the UAE.
To our knowledge, this is the first study to explore CHL within the UAE. Our study aimed to assess the CHL level and its association with relevant socio-demographic characteristics and sources of information among primary health care patients and visitors in the Emirate of Abu Dhabi in the United Arab Emirates (UAE).
Materials and Methods
Study Design
A cross-sectional study was conducted in 7 primary health care centers, also known as Ambulatory Health Services Clinics (AHS), in the city of Al Ain, in the UAE from September 2016 to December 2017. All residents of Al-Ain city, who visited (as patients or family members) primary health care centers and were at least 30 years of age and consented to participate were included in the study. Those with cognitive impairment were excluded. We used the 30 years of age as most of the screening programs are directed to those above 40. However, in some cases with a high prevalence of breast and cervical cancer at premenopausal age in the UAE, we lowered the age of participation to 30 years.19,24
Ethical Considerations
Ethics approval was obtained from the Ambulatory Healthcare Services Ethics Committee, Al Ain City, UAE on the first of July 2015. Written informed consent was obtained from each participant. All data collected from the participants were confidential with no personal identifiers.
Sampling Design
A targeted convenience sample of 511 Al Ain residents were invited consecutively from the pool of eligible patients and visitors to the primary health care centers. The final sample size was 492 and the response rate was 96%. As no previous studies have looked at CHL in the region, the sample size of 511 was calculated based on previous report of cancer screening knowledge prevalence. 24
Data Collection
Data were collected by a team of 3 trained researchers via interviewer-administered questionnaire. The interviewers were adequately trained to ensure valid data collection and minimize any form of potential interviewer bias. CHL was defined as knowledge about cancer, prevention, treatment, screening, and access to services.6,25 A CHL tool was adopted from various existing tools and consisted of 15 questions designed to assess knowledge about the etiology, screening and prevention of cancer. Responses were categorized as “Yes”, “No” or “Do not know”. The response “Do not know” was considered to be no knowledge. “Yes” or “No” was considered either the right answer, ie, knowledge, or the wrong answer, ie, no knowledge, based on the expected correct answer. For example, if the question required a “No” answer and the person replied “Yes” this was considered inadequate knowledge such as the question “Cancer can develop because of an evil eye”. If the question required a “Yes” answer and the person replied “Yes” this was considered adequate knowledge. The questionnaire was modified to improve its validity after it was piloted on 25 participants. The questionnaire was developed and administered in English and Arabic. An experienced and qualified researcher proficient in both English and Arabic translated the content from English to Arabic. Another senior researcher reviewed the initial translation focusing on ensuring linguistic accuracy, consistency, and adherence to cultural nuances. The translated version then was given to an English and Arabic proficient translator who translated the Arabic version into English. The back-translated English version was compared by the research team with the original English text. Discrepancies were carefully analyzed to pinpoint areas where the meaning may have changed. The final translated document was then refined based on the feedback from the back translation process. The final version was agreed upon by the research team. The questionnaire also included sociodemographic information, history of disease, use of alternative therapy and herbs, sources of information, and knowledge about breast, colorectal, and cervical cancer screening. We preferred to develop a tool that may represent cancer literacy among UAE residents based on the available screening programs and available cancer-related education.
Statistical Analysis
All 15 questions of the CHL tool were summed into a score of CHL ranging from zero to 15. In addition, the score was categorized into levels of CHL; poor/inadequate knowledge (0-6 score), moderate knowledge,7-10 and adequate/excellent knowledge.11-15 To test the internal consistency of the tool we calculated the Cronbach’s alpha on a random sample of 100 participants for the 15 questions (α = .93) indicating a high internal consistency.
Categorical variables were presented as frequencies and percentages (%) and continuous variables as median and interquartile range (IQR). The distribution of CHL score was found to be skewed as confirmed by the Shapiro-Wilk test. Accordingly, the Mann-Whitney U test and the Kruskal-Wallis test were applied to compare the mean CHL score with sociodemographic characteristics and sources of information. Chi-square and/or Fisher’s Exact tests as appropriate were used to compare levels of CHL across sociodemographic characteristics and sources of information. Multivariable ordinal logistic regression analysis was further performed to assess the independent association between demographic characteristics and CHL. The outcome variable was CHL measured on an ordinal scale (inadequate, moderate, and adequate). The independent variables included in the model were age category, marital status, nationality, income, education and family history of cancer. All statistical analyses were performed using Stata version 16.1. 26 A P-value less than or equal to .05 was chosen to determine statistical significance. The reporting of this study follows The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 27
Results
Characteristics of Participants
Participants’ Characteristics, Cancer Health Literacy Score and Its Association With Demographic Characteristics (N = 492).

Bold signifies statistical significance; IQR – interquartile range.
NB: Totals do not add up to 492 due to missing data.
Cancer Health Literacy
The overall median CHL score was 8.0 (IQR = 5.0-10.0)). Around 33.7% of the participants had a poor/inadequate level of CHL, 49.6% had a moderate level and 16.7% had an adequate level of CHL (Table 1).
Proportion of Participants With Correct Responses to Questions of Cancer Health Literacy.
Sources of Cancer Health Literacy
Internet (50.7%) was the most common source of information among the participants, followed by television (45.3%), doctor (43.6%), and social media (40.2%) (Figure 1). Table 3 shows the comparison of the median CHL score and distribution of CHL levels among the categories of sources of information. Few cancer-related information sources were found to be associated with adequate cancer health literacy. The average CHL score was significantly higher among those seeking information via posters (9.0 vs 8.0, P = .011). Participants who sought information from booklets, books, and through awareness campaigns had significantly higher average CHL scores (P < .05) compared to those who did not use these sources. None of the sources of information showed a significantly different distribution of the CHL levels except awareness campaigns. The levels of moderate and adequate CHL levels were significantly higher in those receiving their information from awareness campaigns (P = .005). The proportions of those with moderate and adequate CHL increased with the increasing number of sources of information (P = .025). Participants’ sources of information.png. Distribution of Median Scores and Levels of Health Literacy by Sources of Information. Bold signifies statistical significance; IQR – interquartile range.

Comparison of CHL by Demographics Characteristics
Multivariable Regression Analysis for Association Between Demographic Factors and CHL.

Discussion
This study showed that only 16.7% of the participants had adequate to excellent cancer health literacy while 83.3% showed poor to moderate CHL. The level of CHL was higher among those who accessed more sources of information. Most of the socio-demographic variables (age, marital status (before adjustment), nationality, income, level of education and family history of cancer) were significantly associated with the level of cancer health literacy. On the other hand, sex, employment status, and marital status (after adjustment) were not significantly associated with CHL.
The low to moderate CHL levels in this study aligned with another study conducted recently in Saudi Arabia (SA) and Nepal.17,28 A previous study also reported that the estimated health literacy in Europe was 50%. 29
Our study shows that older participants are most likely to have poor CHL level. Generational differences in access to health information and technology is a very important factor that may affect the CHL levels of the older population. Being a fairly young country with the advances in the health care system fairly new, it is very reasonable to find that the older people in the UAE have limited literacy and limited access to health information and technology. Although their access to health care has tremendously improved, the above-mentioned reasons can play a role in the CHL of this population.22,30,31
The study findings show an inverse correlation between participant’s income and CHL which is not consistent with other findings in the region that show higher-income people have better CHL. 28 This relationship could be explained by the fact that people in the UAE generally have equal access to services and education regardless of their income.
Higher education, particularly university-level education, was associated with higher CHL in the present study. This conforms with findings from a recent study conducted in China. 32
Interestingly, 12% of our sample believed that evil eye could cause cancer, which was also identified as a factor that might affect breast screening practices amongst women in the UAE. 24 This indicates that more health awareness about the causes and risk factors is highly important for better cancer prevention. Cultural and religious beliefs significantly influence the healthcare decisions of people in the UAE. 3 3 Fatalism is a common barrier that discourages individuals from seeking help and undergoing cancer screening and treatment. In fact, the stigma associated with cancer and the belief that it is caused by the evil eye or black magic contribute to delayed diagnoses. 34 Patients may initially turn to faith healers before seeking medical attention, resulting in worsened conditions upon arrival at the hospital.33,35,36 It was shown that higher cancer screening rates, screening follow-ups, 6 and advanced treatment are linked to a significant reduction in cancer-specific fatality rates.
CHL was also seen to be higher among non-Emiratis. In the UAE, expatriates or non-Emiratis come from more diverse backgrounds which brings different educational experiences and exposure to health information. This diversity can lead to a broader knowledge base and higher CHL as they may come from countries with healthcare systems that emphasize health education and awareness and better health promotion activities. Also, non-Emiratis may be more proficient in other languages which could enhance their ability to access and understand cancer-related information. Moreover, they might be more proactive in seeking healthcare. Finally, different socioeconomic backgrounds provide them with more resources and opportunities for better health literacy.22,30,37,38
Difficulty in understanding complex medical terminology as people age could be another contributing factor to low CHL among the older generation. To understand the precise factors driving the differences in CHL among different groups, further research, including detailed surveys, interviews, and statistical analyses, would be necessary. Additionally, healthcare providers and policymakers could conduct targeted interventions and education programs to address specific knowledge gaps and improve CHL across various demographics.
Health-related information sources play a critical role in defining health literacy level, where they can vary in reliability, validity, and credibility. This study showed that participants were more likely to get information from social media, television, healthcare professionals, journals, campaigns, booklets, and books. Similar to other studies that reported similar sources of information. 39 Previous reports also showed that healthcare workers, due to their professional education, credibility, and online health information sources, were the most preferred sources for health-related information.40,41 Furthermore, internet use and access are gradually increasing, resulting in a rise in social media and online medical information use. 42 Participants with low health literacy levels go through more trouble in understanding and using health-related information, in comparison to people with adequate health literacy. 43 They also suffer more from negative health outcomes, lower self-perceived health status, and increased risk of hospitalization and death.7,8
Our findings showed that participants with poor cancer health literacy used social magazines and television as the most health information sources. The lower literacy rate could be explained by the fact that these sources give inadequate quality health-related information when compared to information provided by healthcare professionals (doctors and nurses). It was shown that only 4 out of 18 websites were classified as good information quality sources. 44 In addition, our results suggested that participants with low cancer health literacy are less likely to use information provided by doctors and health care professionals; whereas a previous study reported that people with lower literacy levels usually distrust their doctors, or do not understand their instructions, or have bad perceptions due to their previous experiences.45,46
Recently, social media platforms like Facebook, Instagram and Twitter have facilitated and made it more convenient for patients and caretakers to support and connect with each other. 46 In addition, individuals with limited health literacy are somewhat more expected to use celebrity endorsements or bloggers when evaluating website health-related information quality. 47 For this reason, all medical institutions, including academic establishments, state offices, and health-linked associations should take advantage of social media platforms, to present reliable health information to the wider public. This was previously utilized in many tobacco-control campaigns where famous figures and personalities were recruited to promote the action of not smoking.46-48
Presenting a register of reliable and safe health-relevant online websites could promote the acquisition of knowledge by participants with inadequate health literacy. Educating individuals with poor health literacy and improving their ability to separate low-quality health information sources from acceptable quality ones is also suggested. The Quality Guidelines reported by the U.S. Department of Health and Human Services in 2016 mentioned guidance components on how to navigate and pick reliable and good quality online health information sources. 49 Numerous investigators are seeking out methods for affecting health communication through social media and networks. Future investigations are required to explore the elements that promote the usage of social media and blogs for health-related information sources among people with limited health literacy, as it was shown that individuals with inadequate health literacy prefer information sources such as social media and celebrity blogs rather than medical sites.
Supportive healthcare professionals, such as nurse practitioners, physician associates, assistants and librarians could also provide such support in improving their roles.5,50 Furthermore, high-quality health information sources should provide simple and comprehensible information to enable reaching all patients, including those with low health literacy.
Our results suggest that people most likely follow campaigns and awareness activities with moderate cancer health literacy. Given that television, social media, bloggers and celebrities are the platforms with the greatest reach and largest audience, healthcare workers and researchers could use them to provide high-quality health-related information in the form of campaigns and awareness messages. Generally, health literacy was also reported to be significantly associated with the antecedents of health inequalities. In 2015, Mantwill et al 50 performed a systematic review showing the association between health-related literacy levels, and racial/ethnic and educational variations. Another recent study suggested the amelioration of health literacy to improve health behavior and reduce health disparities. 51
This is the first study in the UAE investigating cancer health literacy and its association with several sociodemographic characteristics. The study included a relatively large sample size from various healthcare centers, thereby increasing external validation.
However, the lack of temporality associated with the cross-sectional design and the potential of social desirability bias pose limitations to the study. Moreover, while the findings of the present study can be generalized to the Al Ain Region, it may not be sufficient to generalize to the whole of the UAE as all participants were recruited from the Al Ain Region only.
Another major limitation for this study is that we used our own developed tool as we wanted to include some cultural beliefs that may be related to inadequate cancer knowledge and may impact on treatment and prevention. However, testing its internal validity has shown that can be usable. As this was beyond the scope of the study, we recommend further reliability and consistency testing for this tool.
Conclusions
From a universal health perspective, our results highlighted the value of tailoring instructive and informational communication interventions performed to promote cancer prevention and screening in various communities, especially in cases with low cancer health literacy. This might also help in their practical health literacy, as well as in establishing strategies to assess their progress and significantly improve their knowledge when it comes to making health decisions. Moreover, the cancer literacy score may offer researchers and public health administrators accurate reports on cancer health literacy and identify the population at risk with a poor knowledge level.
Footnotes
Acknowledgments
Authors would like to thank the participants who accepted to take part in this study and staffs of Primary Health Care Centers for support during data collection.
Authors’ Contributions
IE and FAM conceived the idea. IE, MAS and LAS conducted the study, FA and ASA analyzed the data. IE, FAM, FA, LA, ASA wrote the manuscript. All authors reviewed and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SURE grants from UAE University Fund codes # 31M226 & 31M227.
Ethics Statement
The Al-Ain Medical District Ethics Committee and the AHS Ethics Committee approved this study. Written informed consent was obtained from each participant.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.